Carregar apresentação
A apresentação está carregando. Por favor, espere

1
CÂNCER DE PRÓSTATA LOCALIZADO CIRURGIA
Dr. Luiz Ângelo Martins Serviço de Urologia do Hospital das Forças Armadas (HFA) Serviço de Urologia do Hospital Universitário de Brasília (HUB-UnB)
 Serviço de Urologia do Hospital Universitário de Brasília (HUB-UnB)")
2
QUESTIONAMENTOS Por que operamos? Quem operamos? Como operamos?
Quais as nossas limitações? O que nos reserva o futuro?

3
Por que operamos? Diminui a mortalidade e o surgimento de metástases (Bill-Axelson e col., NEJM 2002 e 2011; Schroder e col., NEJM 2012); Reduz em 40% a necessidade de bloqueio hormonal (Bill-Axelson e col., NEJM 2011); Técnicas cirúrgicas eficientes e reproduzíveis; Estadiamento patológico.
; Técnicas cirúrgicas eficientes e reproduzíveis; Estadiamento patológico.")
4
Cumulative Incidence, Absolute Risk Reduction, and Relative Risk for Death from Any Cause, Death from Prostate Cancer, and Development of Distant Metastases. Bill-Axelson A et al. N Engl J Med 2011;364:

5
Cumulative Incidence of Death from Prostate Cancer and Development of Metastases among Men with Low-Risk Prostate Cancer. Figure 2. Cumulative Incidence of Death from Prostate Cancer and Development of Metastases among Men with Low-Risk Prostate Cancer. The cumulative incidence of death from prostate cancer and the development of metastases among men with low-risk prostate cancer (PSA level of <10 and a tumor with a Gleason score of <7 or a WHO grade of 1) is shown. P values refer to absolute between-group differences at 15 years. I bars represent 95% confidence intervals for the cumulative incidence at the 5-year, 10-year, and 15-year follow-up points. Bill-Axelson A et al. N Engl J Med 2011;364:
 is shown. P values refer to absolute between-group differences at 15 years. I bars represent 95% confidence intervals for the cumulative incidence at the 5-year, 10-year, and 15-year follow-up points. Bill-Axelson A et al. N Engl J Med 2011;364:")
7
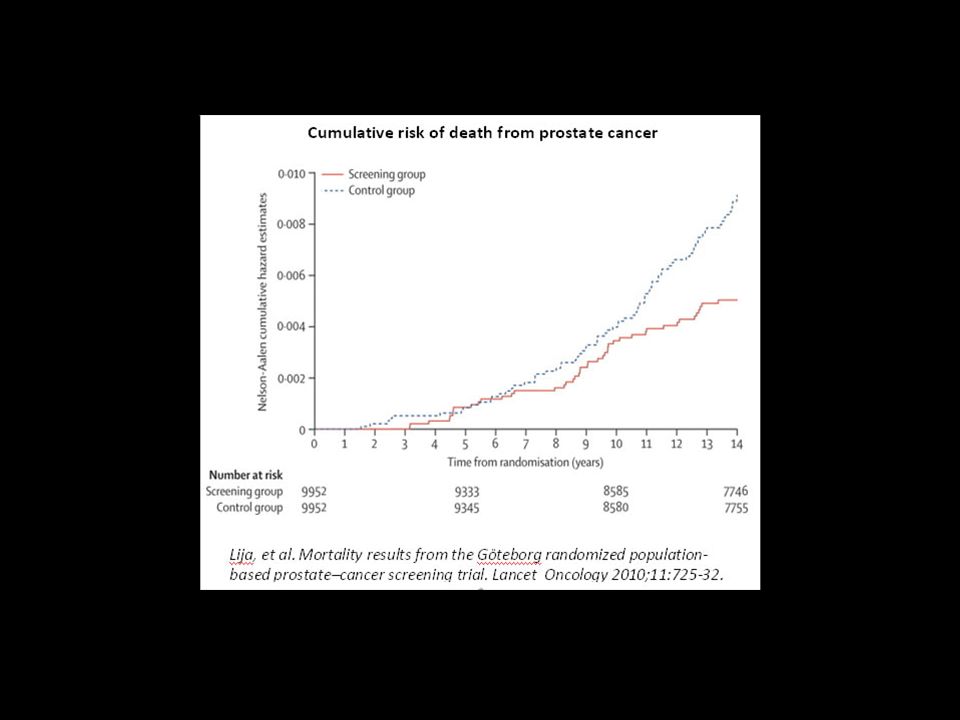
Cumulative Hazard of Death from Prostate Cancer among Men 55 to 69 Years of Age.
Figure 2. Cumulative Hazard of Death from Prostate Cancer among Men 55 to 69 Years of Age. Values are not included for centers in France because of the short follow-up period (median, 4.6 years). The Nelson–Aalen method was used to calculate the cumulative hazard of death from prostate cancer. Schröder FH et al. N Engl J Med 2012;366:
. The Nelson–Aalen method was used to calculate the cumulative hazard of death from prostate cancer. Schröder FH et al. N Engl J Med 2012;366:")
8
Por que operamos? Prostatectomia X EBRT – sobrevida geral e câncer específica tendem a favorecer a prostatectomia radical. Sthephen A. Boorjian e col.. European Urology 2012; 61:

9
Por que operamos? Sthephen A. Boorjian e col.. European Urology 2012; 61:

10
Quem devemos operar? VACURG (1995), USPTF (2011), PIVOT (2012) – overtreatment; Qualidade de vida (QoL) em maior destaque; Casos desafiadores: IMC>30, Cirurgia prostática ou pélvica prévias, Alto risco, Tamanho prostático.

11
Study Enrollment and Treatment.
Figure 1. Study Enrollment and Treatment. Of a total of 13,022 men who were screened for participation, 5023 were eligible for enrollment; of these, 731 were randomly assigned to radical prostatectomy or observation. Of the 364 men in the radical-prostatectomy group, 287 underwent attempted surgery, as did 37 of the 367 men in the observation group. EBRT denotes external-beam radiotherapy. Wilt TJ et al. N Engl J Med 2012;367:

12
Forest Plots for Primary and Secondary Outcomes.
Figure 3. Forest Plots for Primary and Secondary Outcomes. There were no significant between-group differences in all-cause mortality according to age, score on the Gleason histologic scale (<7 vs. ≥7 on a scale of 2 to 10, with 10 indicating the most poorly differentiated tumors),13 self-reported race, self-reported performance status (0 [fully active] vs. 1 to 4, with higher scores indicating poorer functional status), or score on the Charlson comorbidity index 12 (Panel A), but there was a significant interaction between study group and baseline PSA value (P=0.04 for interaction) and a borderline interaction (P=0.07) for tumor risk (D'Amico tumor risk score [low, intermediate, or high], which was based on tumor stage, histologic score, and PSA level 14). Prostate-cancer mortality did not differ significantly between the study groups according to age, race, score on the Charlson comorbidity index, or self-reported performance status (Panel B), although there was borderline evidence of an interaction for PSA value and tumor-risk category (P=0.11 for interaction for both comparisons). The bars indicate 95% confidence intervals, and the size of the symbol indicates the weight of the estimate. Wilt TJ et al. N Engl J Med 2012;367:
,13 self-reported race, self-reported performance status (0 [fully active] vs. 1 to 4, with higher scores indicating poorer functional status), or score on the Charlson comorbidity index 12 (Panel A), but there was a significant interaction between study group and baseline PSA value (P=0.04 for interaction) and a borderline interaction (P=0.07) for tumor risk (D Amico tumor risk score [low, intermediate, or high], which was based on tumor stage, histologic score, and PSA level 14). Prostate-cancer mortality did not differ significantly between the study groups according to age, race, score on the Charlson comorbidity index, or self-reported performance status (Panel B), although there was borderline evidence of an interaction for PSA value and tumor-risk category (P=0.11 for interaction for both comparisons). The bars indicate 95% confidence intervals, and the size of the symbol indicates the weight of the estimate. Wilt TJ et al. N Engl J Med 2012;367:")
13
Kaplan–Meier Plots of Mortality.
Figure 2. Kaplan–Meier Plots of Mortality. By the end of the study, 354 men (48.4%) had died from any cause (Panel A). Death attributed to prostate cancer or treatment occurred in 52 men (7.1%) (Panel B). Data from the radical-prostatectomy group are shown in red, and data from the observation group in blue. Wilt TJ et al. N Engl J Med 2012;367:
 had died from any cause (Panel A). Death attributed to prostate cancer or treatment occurred in 52 men (7.1%) (Panel B). Data from the radical-prostatectomy group are shown in red, and data from the observation group in blue. Wilt TJ et al. N Engl J Med 2012;367:")
14
A new study shows that prostate cancer surgery, which often leaves men impotent or incontinent, does not appear to save the lives of men with early-stage disease, who account for most cases, and many of these men would do just as well to choose no treatment at all. , ,July 18th, 2012

15
Prostate-Cancer Mortality in the Two Groups of the Scandinavian Prostate Cancer Study Number 4 Randomized Trial, as Compared with the University of Toronto Active Surveillance Cohort. Figure 1. Prostate-Cancer Mortality in the Two Groups of the Scandinavian Prostate Cancer Study Number 4 Randomized Trial, as Compared with the University of Toronto Active Surveillance Cohort. N Engl J Med 2011;365:

16
Mudança de paradigma?

17
Quem devemos operar?

18
Quem operamos? Quem beneficiamos?
Maiores benefícios: Idade < 65 anos, Gleason 7 ou 8 e estadio T2, PSA ≥ 10. Possíveis benefícios: Gleason 6 e T2 ou Gleason 7 e T1. Benefícios não comprovados: Idade > 70 anos, Gleason 6 e estadio T1.

19
Como operamos? Procedimentos abertos: Retropúbico - A Perineal
Procedimentos minimamente invasivos: Laparoscopia - L Laparoscopia assistida por robô - R

20
Como operamos?

21
Como operamos? Dr. Patrick C. Walsh

22
Como operamos?

23
Como operamos?

24
Como operamos?

25
Como operamos?

26
Como operamos?

27
Como operamos? Resultados - QoL
QoL - difícil avaliar; Walsh (2000) – continência urinária – 93% - 18 meses (no pads); Walsh (2000) – ereção – 86% - 18 meses (com ou sem sildenafila); Variações na literatura: Continência urinária: 88 a 97% Ereção: 31 a 86% (JAMA 2000 – 44%)
 – continência urinária – 93% - 18 meses (no pads); Walsh (2000) – ereção – 86% - 18 meses (com ou sem sildenafila); Variações na literatura: Continência urinária: 88 a 97% Ereção: 31 a 86% (JAMA 2000 – 44%)")
28
Copyright © 2012 American Medical Association. All rights reserved.
From: Prediction of Erectile Function Following Treatment for Prostate Cancer JAMA. 2011;306(11): doi: /jama Alemozaffar, Regan e col. JAMA. 2011;306(11): n=511 – EF 35%(177) Figure Legend: Model-predicted probabilities based on pretreatment Expanded Prostate Cancer Index Composite sexual function score stratified by age, pretreatment prostate-specific antigen (PSA) level, and planned nerve sparing. Higher sexual function score denotes better sexual function. N=524 (66 [13%] with PSA level >10 ng/mL and 43 [8%] undergoing non−nerve-sparing surgery); median age, 60 years. Date of download: 11/17/2012 Copyright © 2012 American Medical Association. All rights reserved.
: doi: /jama Alemozaffar, Regan e col. JAMA. 2011;306(11): n=511 – EF 35%(177) Figure Legend: Model-predicted probabilities based on pretreatment Expanded Prostate Cancer Index Composite sexual function score stratified by age, pretreatment prostate-specific antigen (PSA) level, and planned nerve sparing. Higher sexual function score denotes better sexual function. N=524 (66 [13%] with PSA level >10 ng/mL and 43 [8%] undergoing non−nerve-sparing surgery); median age, 60 years. Date of download: 11/17/2012. Copyright © 2012 American Medical Association. All rights reserved.")
29
Como operamos? Dr. Hugh Hampton Young

30
Como operamos?

31
Como operamos?

32
Como operamos?

33
Como operamos?

34
Como operamos?

35
Como operamos?

36
Como operamos? PR assistida por robô.
Intuitive Surgical Report 2012

37
Como operamos? A x R – Margem +
Eur Urol 2012, 62:

38
Como operamos? A x R – Margem + T2
Eur Urol 2012, 62:

39
Como operamos? L x R – Margem +
Eur Urol 2012, 62:

40
Como operamos? L x R – Margem + T2
Eur Urol 2012, 62:

41
Como operamos? A x R – Continência urinária
Eur Urol 2012, 62:

42
Como operamos? L x R – Continência urinária
Eur Urol 2012, 62:

43
Como operamos? A x R – Ereção
Eur Urol 2012, 62:

44
Como operamos? L x R – Ereção
Eur Urol 2012, 62:

45
Como operamos? Lavery et all, NCI – Cancer Bulletin Report, Aug 2011

46
Como operamos?

47
Como operamos?

48
Como operamos?

49
Quais as nossas limitações?
Trabalhos científicos adequados; Ferrramentas confiáveis para o diagnóstico e avaliação prognóstica; Morbidade mínima reprodutível.

50
O que nos reserva o futuro?
Resultados do estudo ProtecT; Marcadores genéticos; Melhora dos métodos de imagem; Terapias menos invasivas e mais eficientes; Otimização de custos.

51
“Not everything that can be counted counts, and not everything that counts can be counted.”

Apresentações semelhantes





: (based on and the message from INPAs General Director, Dr Adalberto Val, and on former.>")



. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")
 Rector of University.>")








