Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Tratamento da Dislipidemia no Paciente com DM2
Alexander Benchimol IEDE – PUC - RJ

2
Conflito de Interesse ABBOTT (BOARD E PESQUISA CLÍNICA)
ABBOTT NUTRITION (BOARD) LIBBS (SPEAKER) MSD (SPEAKER) NOVO NORDISK (BOARD) SANOFI AVENTIS (SPEAKER E PESQUISA CLÍNICA) TORRENT(SPEAKER)
 LIBBS (SPEAKER) MSD (SPEAKER) NOVO NORDISK (BOARD) SANOFI AVENTIS (SPEAKER E PESQUISA CLÍNICA) TORRENT(SPEAKER)")
3
Resistência à insulina
LDL-c pequena e densa Hiper- insulinemia Hipertri- gliceridemia HDL-c baixo Hipercoagu-labilidade Hipertensão Obesidade Diabetes Aterosclerose

4
Aterotrombose* é a principal Causa de Morte em todo o mundo**¹
AIDS 5% Morte Violenta 12% Doenças Respiratórias 14% Doenças Infecciosas 19% Atherothrombosis is the underlying condition that results in events leading to myocardial infarction, ischemic stroke, and vascular death. As such, the leading cause of death of the estimated 55,694,000 people worldwide who died in 2000 was atherothrombosis, manifested as cardiovascular disease, ischemic heart disease and stroke (52% of deaths). Other main causes of death were: AIDS (5%) violent death (12%) pulmonary disease (14%) infectious diseases (19%) cancer (24%). Câncer 24% Aterotrombose* 52% Mortalidade (%) 10 20 30 40 50 60 *Doença Cardiovascular, doença isquemica do coração e doença cerebrovascular **Região OMS (Africa, Americas, Europa, Leste Europeu, Sudeste da Ásia e Oeste do Pacífico) 1. The World Health Report Geneva: WHO; 2001. Reference: 1. The World Health Report Geneva: WHO; 2001.
. Other main causes of death were: AIDS (5%) violent death (12%) pulmonary disease (14%) infectious diseases (19%) cancer (24%). Câncer. 24% Aterotrombose* 52% Mortalidade (%) *Doença Cardiovascular, doença isquemica do coração e doença cerebrovascular. **Região OMS (Africa, Americas, Europa, Leste Europeu, Sudeste da Ásia e Oeste do Pacífico) 1. The World Health Report Geneva: WHO; Reference: 1. The World Health Report Geneva: WHO;")
5
Type 2 Diabetes Increases CHD Morbidity and Mortality
Ad sever/Medivia/Galida Slides/ ADA slide kit _v27 Type 2 Diabetes Increases CHD Morbidity and Mortality 10 15 20 25 30 35 40 45 50 5 No previous MI Previous MI 45.0% * MI at 7 years follow-up (%) 20.2% 18.8% Slide 3 3.5% Nondiabetic Diabetic * Mortality rates are not significantly different. P<.001 for diabetic vs nondiabetic. Haffner et al. N Engl J Med. 1998;339:
 20.2% 18.8% Slide % Nondiabetic. Diabetic. * Mortality rates are not significantly different. P<.001 for diabetic vs nondiabetic. Haffner et al. N Engl J Med. 1998;339:")
6
Quanto Mais Alto o Nível do Colesterol Maior a Taxa de Mortalidade
18 16 14 12 10 Taxa de mortalidade por 1000 homens 8 6 4 2 140 160 180 200 220 240 260 280 300 Colesterol Total (mg/dL) MRFIT study. Martin et al. Lancet 1986; ii:933–936
 MRFIT study. Martin et al. Lancet 1986; ii:933–936.")
7
Incidência de DAC em 14 anos
HDL-C Baixo Aumenta o Risco de DAC mesmo quando o Colesterol Total é Normal (Framingham) 12.50 11.91 11.91 14 9.05 10.7 12 11.24 10 6.6 5.53 3.83 Incidência de DAC em 14 anos 8 6.56 4.85 6 4.67 2.06 260 4.15 3.77 Low HDL-C Levels Increase CHD Risk Even When Total-C Is Normal (Framingham) Low high-density lipoprotein cholesterol (HDL-C) levels (< 40 mg/dL) are associated with an increased risk of coronary heart disease (CHD) even if the total cholesterol (Total-C) level is < 200 mg/dL. This slide shows the CHD incidence over 14 years among Framingham Study subjects who were aged 48–83 years at baseline. Among those with HDL-C levels < 40 mg/dL and Total-C < 200 mg/dL, 11.24% experienced a CHD event. This incidence was virtually the same as that (11.91%) for subjects with HDL-C levels between 40–49 mg/dL and Total-C 260 mg/dL. References: Castelli WP, Garrison RJ, Wilson PW, et al. Incidence of coronary heart disease and lipoprotein cholesterol levels: the Framingham Study. JAMA. 1986;256:2835–2838. 4 2.78 230–259 2 200–229 Total-C (mg/dL) < 200 < 40 40–49 50–59 60 HDL-C (mg/dL) Risk of CHD by HDL-C and Total-C levels; aged 48–83 y Castelli WP et al. JAMA 1986;256:2835–2838
 Incidência de DAC em 14 anos Low HDL-C Levels Increase CHD Risk Even When Total-C Is Normal (Framingham) Low high-density lipoprotein cholesterol (HDL-C) levels (< 40 mg/dL) are associated with an increased risk of coronary heart disease (CHD) even if the total cholesterol (Total-C) level is < 200 mg/dL. This slide shows the CHD incidence over 14 years among Framingham Study subjects who were aged 48–83 years at baseline. Among those with HDL-C levels < 40 mg/dL and Total-C < 200 mg/dL, 11.24% experienced a CHD event. This incidence was virtually the same as that (11.91%) for subjects with HDL-C levels between 40–49 mg/dL and Total-C 260 mg/dL. References: Castelli WP, Garrison RJ, Wilson PW, et al. Incidence of coronary heart disease and lipoprotein cholesterol levels: the Framingham Study. JAMA. 1986;256:2835– – –229. Total-C (mg/dL) < 200. < –49. 50–59. 60. HDL-C (mg/dL) Risk of CHD by HDL-C and Total-C levels; aged 48–83 y. Castelli WP et al. JAMA 1986;256:2835–2838.")
10
Estratégias no TTO da dislipidemia no DM2
Primary Strategy - Lower LDL cholesterol Secondary Strategy - Raise HDL cholesterol - Lower triglycerides Other Approaches - Non-HDL cholesterol - ApoB - Remnants Treatment Strategies for Diabetic Dyslipidemia According to the American Diabetes Association (ADA), the primary strategy in the treatment of diabetic dyslipidemia is to lower low-density lipoprotein (LDL) cholesterol, and the secondary strategy is to raise high-density lipoprotein (HDL) cholesterol and lower triglycerides. In addition, there are a number of other approaches, including reducing non-HDL cholesterol, which will probably be adopted as a secondary target by the National Cholesterol Education Program (NCEP) in their Adult Treatment Panel III recommendations. A number of investigators believe that apolipoprotein (apo) B may be even a better target than LDL cholesterol, but the measurement of apo B is not sufficiently standardized, at least according to the NCEP. A number of individuals also think that remnants may be better predictors of CHD, but lack of standardization of measurement presents potential problems with this target as well. References: American Diabetes Association. Management of dyslipidemia in adults with diabetes. Diabetes Care 2000;23 (suppl 1):S57-S60. Chait A, Brunzell JD. Diabetes, lipids, and atherosclerosis. In: LeRoith D, Taylor SI, Olefsky JM, eds. Diabetes Mellitus: a Fundamental and Clinical Text. Philadelphia: Lippincott-Raven, 1996: European Diabetes Policy Group A desktop guide to Type 2 diabetes mellitus. Diabet Med 1999;16: Adapted from American Diabetes Association. Diabetes Care. 2000;23(suppl 1):S57-S60; Chait A, Brunzell JD. Diabetes Mellitus. A Fundamental and Clinical Text. Philadelphia: Lippincott Raven, 1996; ; European Diabetes Policy Group Diabet Med. 1999;16:
, the primary strategy in the treatment of diabetic dyslipidemia is to lower low-density lipoprotein (LDL) cholesterol, and the secondary strategy is to raise high-density lipoprotein (HDL) cholesterol and lower triglycerides. In addition, there are a number of other approaches, including reducing non-HDL cholesterol, which will probably be adopted as a secondary target by the National Cholesterol Education Program (NCEP) in their Adult Treatment Panel III recommendations. A number of investigators believe that apolipoprotein (apo) B may be even a better target than LDL cholesterol, but the measurement of apo B is not sufficiently standardized, at least according to the NCEP. A number of individuals also think that remnants may be better predictors of CHD, but lack of standardization of measurement presents potential problems with this target as well. References: American Diabetes Association. Management of dyslipidemia in adults with diabetes. Diabetes Care 2000;23 (suppl 1):S57-S60. Chait A, Brunzell JD. Diabetes, lipids, and atherosclerosis. In: LeRoith D, Taylor SI, Olefsky JM, eds. Diabetes Mellitus: a Fundamental and Clinical Text. Philadelphia: Lippincott-Raven, 1996: European Diabetes Policy Group A desktop guide to Type 2 diabetes mellitus. Diabet Med 1999;16: Adapted from American Diabetes Association. Diabetes Care. 2000;23(suppl 1):S57-S60; Chait A, Brunzell JD. Diabetes Mellitus. A Fundamental and Clinical Text. Philadelphia: Lippincott Raven, 1996; ; European Diabetes Policy Group Diabet Med. 1999;16:")
11
Relative Risk for CHD (Log Scale)
“The Lower, the Better” 3.7 1 2.9 Relative Risk for CHD (Log Scale) 2.2 1.7 1.3 1.0 40 70 100 130 160 190 LDL-C (mg/dL) Grundy SM et al. Circulation 2004;110:227–239.
 LDL-C (mg/dL) Grundy SM et al. Circulation 2004;110:227–239.")
12
Tratamento Farmacológico: Estatinas
Inibem a síntese do colesterol, receptores de LDL Efeitos benéficos nos parâmetros lipídicos C-LDL 18%-55% C-HDL 5%-15% TG 7%-30% Redução relativa de 24% a 40% dos eventos coronarianos Efeitos adversos : miopatia, enzimas hepáticas e CK Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486.

13
Efeitos potenciais das estatinas ao longo do tempo
Estabilização das placas vulneráveis Redução de LDL-C* Redução da inflamação Restauração da função endotelial Redução dos episódios isquêmicos Redução de eventos cardíacos* Potential time course of statin effects CHD risk reduction with a statin appears to occur as a result of several related changes, including restoration of endothelial function, reduction in inflammation, and stabilization of vulnerable plaque. The time course for these antiatherosclerotic effects of statins ranges from days to years. Within weeks to months after beginning statin therapy, endothelial function of coronary arteries is restored. Concurrent with this or following by just a few months is a reduction in inflammatory markers, such as high-sensitivity C-reactive protein. These effects appear to coincide with the reduction in ischemic events demonstrated after about 18 months of statin therapy. After several years of therapy (i.e., 1.5–2.5 years), fatal and nonfatal myocardial infarction rates begin to decline in statin-treated patients, and after 5 years of therapy, significant reductions have been documented. These changes coincide somewhat with stabilization of vulnerable atherosclerotic plaque during which the lipid-rich core of plaque is replaced with connective tissue and matrix. Dias Anos * Time course established
, fatal and nonfatal myocardial infarction rates begin to decline in statin-treated patients, and after 5 years of therapy, significant reductions have been documented. These changes coincide somewhat with stabilization of vulnerable atherosclerotic plaque during which the lipid-rich core of plaque is replaced with connective tissue and matrix. Dias. Anos. * Time course established.")
14
REDUÇÃO RELATIVA DO RISCO
Redução do risco relativo de morte por DAC/ eventos coronarianos Prevenção Primária ou Secundária com vastatinas AFCAPS/ TexCAPS+ WOSCOPS CARE HPS 4S LIPID TNT –10 –20 REDUÇÃO RELATIVA DO RISCO (%) –20% –22% -24% –24% –30 –28% –40 –37% –42% –50 PREVENÇÃO PRIMÁRIA PREVENÇÃO SECUNDÁRIA Estudos independentes, não comparativos, com populações diferentes de pacientes AFCAP/TEXCAPS= Air Force/texas Coronary Atherosclerosis Prevention Study; WOSCOPS= West of Scotland Coronary Prevention Study; CARE= Cholesterol and Recurrent Events; 4S= Scandinavian Simvastatin Survival Study; LIPID= Long-term Intervation with Pravastatin in Ischemic Disease; TNT= Treating to New Targets. +Principais eventos coronarianos; morte relacionada à DAC em todos os outros estudos. Adaptado de Downs JR et al JAMA 1998;279(20):1615–1622; Sheperd J et al N Engl J Med 1995;333(20):1301–1307; Sacks FM et al N Engl J Med 1996;335:1001–1009; 4S study group LANCET 1994;344:1383–1389; LIPID study group N Engl J Med 1998;339(19):1349–1357; LaRosa JC et al. N Engl J Med 2005;352:1-11.
 –20% –22% -24% –24% –30. –28% –40. –37% –42% –50. PREVENÇÃO PRIMÁRIA. PREVENÇÃO SECUNDÁRIA. Estudos independentes, não comparativos, com populações diferentes de pacientes. AFCAP/TEXCAPS= Air Force/texas Coronary Atherosclerosis Prevention Study; WOSCOPS= West of Scotland Coronary Prevention Study; CARE= Cholesterol and Recurrent Events; 4S= Scandinavian Simvastatin Survival Study; LIPID= Long-term Intervation with Pravastatin in Ischemic Disease; TNT= Treating to New Targets. +Principais eventos coronarianos; morte relacionada à DAC em todos os outros estudos. Adaptado de Downs JR et al JAMA 1998;279(20):1615–1622; Sheperd J et al N Engl J Med 1995;333(20):1301–1307; Sacks FM et al N Engl J Med 1996;335:1001–1009; 4S study group LANCET 1994;344:1383–1389; LIPID study group N Engl J Med 1998;339(19):1349–1357; LaRosa JC et al. N Engl J Med 2005;352:1-11.")
15
CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses
Baseline LDL-C, mg/dl (mmol/L) LDL-C Lowering Study Drug No. Primary Prevention AFCAPS/TexCAPS Secondary Prevention CARE 4S LIPID Lovastatin Pravastatin Simvastatin 239 586 202 782 150 (3.9) 136 (3.6) 186 (4.8) 150* (3.9) 25% 28% 36% 25%* CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses Primary and secondary prevention trials of statin therapy have included a fairly large number of diabetic subjects. Mean baseline LDL cholesterol levels for the various trials have ranged from a low of 136 mg/dL in CARE to 186 mg/dL in the Scandinavian Simvastatin Survival Study (4S), and the degree of LDL cholesterol lowering has ranged from 25% in the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS) and the Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) to 36% in 4S. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyörälä K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: *Values for overall group Adapted from Downs JR et al. JAMA 1998;279: ; Goldberg RB et al. Circulation 1998;98: ; Pyörälä K et al. Diabetes Care 1997;20: ; Haffner SM et al. Arch Intern Med 1999;159: ; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339:
 LDL-C Lowering. Study. Drug. No. Primary Prevention. AFCAPS/TexCAPS. Secondary Prevention. CARE. 4S. LIPID. Lovastatin. Pravastatin. Simvastatin (3.9) 136 (3.6) 186 (4.8) 150* (3.9) 25% 28% 36% 25%* CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses. Primary and secondary prevention trials of statin therapy have included a fairly large number of diabetic subjects. Mean baseline LDL cholesterol levels for the various trials have ranged from a low of 136 mg/dL in CARE to 186 mg/dL in the Scandinavian Simvastatin Survival Study (4S), and the degree of LDL cholesterol lowering has ranged from 25% in the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS) and the Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) to 36% in 4S. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyörälä K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: *Values for overall group. Adapted from Downs JR et al. JAMA 1998;279: ; Goldberg RB et al. Circulation 1998;98: ; Pyörälä K et al. Diabetes Care 1997;20: ; Haffner SM et al. Arch Intern Med 1999;159: ; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339:")
16
CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses (cont’d)
CHD Risk Reduction (overall) CHD Risk Reduction (diabetes) Study Drug No. Primary Prevention AFCAPS/TexCAPS Secondary Prevention CARE 4S LIPID 4S-Extended Lovastatin Pravastatin Simvastatin 239 586 202 782 483 37% 23% 32% 25% 43% 25% (p=0.05) 55% (p=0.002) 19% 42% (p=0.001) CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses (continued) CHD risk reduction among diabetic subjects was greater in 4S and AFCAPS/TexCAPS than in CARE and LIPID. Perhaps more importantly, CHD risk reduction in the overall study groups was comparable or even less than in the diabetic subgroups, which is important in establishing a criteria for similar therapy in diabetics and in CHD patients. There is certainly no evidence that statin therapy is any less effective in diabetic patients than in patients without diabetes. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyörälä K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: Adapted from Downs JR et al. JAMA 1998;279: ; Goldberg RB et al. Circulation 1998;98: ; Pyörälä K et al. Diabetes Care 1997;20: ; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339: ; Haffner SM et al. Arch Intern Med 1999;159:
 CHD Risk Reduction (diabetes) Study. Drug. No. Primary Prevention. AFCAPS/TexCAPS. Secondary Prevention. CARE. 4S. LIPID. 4S-Extended. Lovastatin. Pravastatin. Simvastatin % 23% 32% 25% 43% 25% (p=0.05) 55% (p=0.002) 19% 42% (p=0.001) CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses (continued) CHD risk reduction among diabetic subjects was greater in 4S and AFCAPS/TexCAPS than in CARE and LIPID. Perhaps more importantly, CHD risk reduction in the overall study groups was comparable or even less than in the diabetic subgroups, which is important in establishing a criteria for similar therapy in diabetics and in CHD patients. There is certainly no evidence that statin therapy is any less effective in diabetic patients than in patients without diabetes. References: Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr, for the AFCAPS/TexCAPS Research Group. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 1998;279: Goldberg RB, Mellies MJ, Sacks FM, Moye LA, Howard BV, Howard WJ, Davis BR, Cole TG, Pfeffer MA, Braunwald E. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events (CARE) trial. Circulation 1998;98: Pyörälä K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G, Scandinavian Simvastatin Survival Study (4S) Group. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care 1997;20: Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339: Haffner SM, Alexander CM, Cook TJ, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: subgroup analyses in the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159: Adapted from Downs JR et al. JAMA 1998;279: ; Goldberg RB et al. Circulation 1998;98: ; Pyörälä K et al. Diabetes Care 1997;20: ; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339: ; Haffner SM et al. Arch Intern Med 1999;159:")
17
4S: Effect of Statin Therapy on Hospital Stay
Bed Days (per 100 Pts) 4S: Effect of Statin Therapy on Hospital Stay In an economic analysis of the effect of simvastatin on hospital stay in 4S, there was a 55% reduction with simvastatin therapy in patients with diabetes (using the ADA criterion), a 38% reduction in patients with impaired fasting glucose, and a 28% reduction in patients with normal fasting glucose. This suggests that the economic benefit of simvastatin therapy is, if anything, somewhat greater in patients with diabetes or impaired fasting glucose than in nondiabetic patients. This analysis also found that the cost of medical care in diabetics in 4S was lower in the simvastatin group than in the placebo group, because the reduction in hospitalization was so great it offset the increased cost of medical therapy for simvastatin. Reference: Herman WH, Alexander CM, Cook JR, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Effect of simvastatin treatment on cardiovascular resource utilization in impaired fasting glucose and diabetes. Findings from the Scandinavian Simvastatin Survival Study. Diabetes Care 1999;22: Simvastatin Placebo Simvastatin Placebo Simvastatin Placebo Normal fasting glucose Impaired fasting glucose Diabetes mellitus Adapted from Herman WH et al. Diabetes Care 1999;22:
 4S: Effect of Statin Therapy on Hospital Stay. In an economic analysis of the effect of simvastatin on hospital stay in 4S, there was a 55% reduction with simvastatin therapy in patients with diabetes (using the ADA criterion), a 38% reduction in patients with impaired fasting glucose, and a 28% reduction in patients with normal fasting glucose. This suggests that the economic benefit of simvastatin therapy is, if anything, somewhat greater in patients with diabetes or impaired fasting glucose than in nondiabetic patients. This analysis also found that the cost of medical care in diabetics in 4S was lower in the simvastatin group than in the placebo group, because the reduction in hospitalization was so great it offset the increased cost of medical therapy for simvastatin. Reference: Herman WH, Alexander CM, Cook JR, Boccuzzi SJ, Musliner TA, Pedersen TR, Kjekshus J, Pyorala K, for the Scandinavian Simvastatin Survival Study Group. Effect of simvastatin treatment on cardiovascular resource utilization in impaired fasting glucose and diabetes. Findings from the Scandinavian Simvastatin Survival Study. Diabetes Care 1999;22: Simvastatin. Placebo. Simvastatin. Placebo. Simvastatin. Placebo. Normal fasting glucose. Impaired fasting glucose. Diabetes mellitus. Adapted from Herman WH et al. Diabetes Care 1999;22:")
18
Objetivo do estudo CARDS
Avaliar a eficácia e segurança da atorvastatina 10mg administrada 1x/dia vs. placebo, na prevenção primária da doença cardiovascular (DAC e acidente vascular cerebral) em pacientes com diabetes tipo 2, sem aumento nos níveis de colesterol.
 em pacientes com diabetes tipo 2, sem aumento nos níveis de colesterol.")
19
Endpoints CARDS Primários Secundários
Tempo a partir da randomização até a primeira ocorrência de: • Evento coronariano importante (IM fatal ou não fatal, outra morte por DCV) • IM silencioso • AVC • Parada cardíaca com reanimação • Procedimento de revascularização coronariana • Angina instável Secundários Tempo a partir da randomização até a primeira ocorrência de um endpoint clínico primário ou secundário (isto é, morte, angina, ataque isquêmico transitório não fatal, doença vascular periférica e outros eventos cardiovasculares não fatais). Tempo a partir da randomização até a morte por qualquer causa (mortalidade por todas as causas). Lípides e lipoproteínas. No estudo CARDS, o objetivo primário do estudo é investigar se o tratamento com atorvastatina reduz os principais eventos coronarianos (fatais ou não fatais), acidente vascular cerebral, parada cardíaca reanimada, procedimentos de revascularização coronariana e angina instável. Os objetivos secundários do estudo são: (i) examinar se o tratamento em andamento com atorvastatina reduz a incidência de morte e outros endpoints cardiovasculares, (ii) examinar o efeito do tratamento com atorvastatina sobre as concentrações séricas de lipídios e lipoproteínas e (iii) avaliar a segurança da terapia crônica à base de atorvastatina. Colhoun HM, Thomason MJ, Mackness MI, et al. Design of the Collaborative AtoRvastatin Diabetes Study (CARDS) in patients with Type 2 diabetes. Diabet Med. 2002;19: Colhoun HM, Thomason MJ, Mackness MI, et al. Diabet Med ;19:
 • IM silencioso. • AVC. • Parada cardíaca com reanimação. • Procedimento de revascularização coronariana. • Angina instável. Secundários. Tempo a partir da randomização até a primeira ocorrência de um endpoint clínico primário ou secundário (isto é, morte, angina, ataque isquêmico transitório não fatal, doença vascular periférica e outros eventos cardiovasculares não fatais). Tempo a partir da randomização até a morte por qualquer causa (mortalidade por todas as causas). Lípides e lipoproteínas. No estudo CARDS, o objetivo primário do estudo é investigar se o tratamento com atorvastatina reduz os principais eventos coronarianos (fatais ou não fatais), acidente vascular cerebral, parada cardíaca reanimada, procedimentos de revascularização coronariana e angina instável. Os objetivos secundários do estudo são: (i) examinar se o tratamento em andamento com atorvastatina reduz a incidência de morte e outros endpoints cardiovasculares, (ii) examinar o efeito do tratamento com atorvastatina sobre as concentrações séricas de lipídios e lipoproteínas e (iii) avaliar a segurança da terapia crônica à base de atorvastatina. Colhoun HM, Thomason MJ, Mackness MI, et al. Design of the Collaborative AtoRvastatin Diabetes Study (CARDS) in patients with Type 2 diabetes. Diabet Med. 2002;19: Colhoun HM, Thomason MJ, Mackness MI, et al. Diabet Med. 2002;19:")
20
Risco cumulativo para o endpoint primário
Redução do risco relativo de 37% (IC de 95%: ) 15 P=0,001 Placebo 127 eventos 10 Risco Cumulativo (%) Atorvastatina 83 eventos 5 1 2 3 4 4,75 Anos Placebo 1410 1351 1306 1022 651 305 Atorvastatina 1428 1392 1361 1074 694 328
 15. P=0,001. Placebo. 127 eventos. 10. Risco Cumulativo (%) Atorvastatina. 83 eventos ,75. Anos. Placebo Atorvastatina")
21
Resinas Mecanismo: liga-se com os ácidos biliares, interrompendo a circulação entero-hepática do colesterol, diminuindo a concentração hepática de colesterol e o aumentando a atividade do receptor de LDL. Principais Agentes: colestiramina (Questran), colestipol, coleveselan HDL metabolism as a therapeutic target: potential strategies (II) Another approach to targeting HDL would be to promote the process of reverse cholesterol transport.
, colestipol, coleveselan. HDL metabolism as a therapeutic target: potential strategies (II) Another approach to targeting HDL would be to promote the process of reverse cholesterol transport.")
22
SEQUESTRANTES DE ÁCIDOS BILIARES
Resinas SEQUESTRANTES DE ÁCIDOS BILIARES - CT e LDL (até 30%), pode TG (10-20%) HDL (até 8%) - Indicados para tto de hipercolesterolemia em crianças e mulheres em idade fértil sem método contraceptivo ou gestantes - EC: obstipação intestinal, náuseas, meteorismo, dor abdominal, esteatorréia, vitaminas lipossolúveis
, pode TG (10-20%) HDL (até 8%) - Indicados para tto de hipercolesterolemia em crianças e mulheres em idade fértil sem método contraceptivo ou gestantes. - EC: obstipação intestinal, náuseas, meteorismo, dor abdominal, esteatorréia, vitaminas lipossolúveis.")
23
Inibidores seletivos da absorção do colesterol: Ezetimiba
Mecanismo de ação e seletividade Bloqueia a absorção do colesterol na borda em escova intestinal Sem efeito na absorção das vitaminas lipossolúveis Farmacologia Localização na parede intestinal Circulação êntero-hepática Mínima exposição sistêmica Experiência clínica e papel no manejo Monoterapia Combinação

24
Ezetimiba e LDL-C Plasmático: Dose-Resposta
5 Ezetimiba 0,25 mg (n=47) Ezetimiba 1 mg (n=49) Ezetimiba 5 mg (n=49) Ezetimiba 10 mg (n=46) Placebo (n=52) –5 Alteração % média no LDL-C + –10 + –15 + Slide 8 Dois estudos fase II, com 12 semanas de duração, multicêntricos, controlados com placebo, duplo-cegos, randômicos, de grupos paralelos, avaliaram a capacidade de reduzir o LDL-C do ezetimibe em monoterapia. O estudo de dose-resposta envolveu uma gama de doses de ezetimibe e seu desenho foi o seguinte: após estabilização com dieta (National Cholesterol Education Program Fase I ou dieta mais rigorosa), washout de medicamentos modificadores de lípides e um período de seis semanas com placebo, os pacientes com idade entre 18–75 anos e níveis plasmáticos de LDL-C no período basal entre 3,4 e 6,5 mmol/l (131 e 251 mg/dl) e de triglicérides (TG) 3,4 mmol/l (300 mg/dl) foram distribuídos de modo randômico para receber 0,25 mg, 1, 5 mg ou 10 mg de ezetimibe ou placebo uma vez ao dia, antes da primeira refeição do dia. No estudo de dose-resposta (n=243), doses de 0,25 mg a 10 mg/dia de ezetimibe reduziram o LDL-C em 9,9 % a 18,7% em comparação com o placebo no final de 12 semanas (todos os valores de p<0,01 vs. placebo).3 + –20 2 4 6 8 10 12 Endpoint (±EPM) Período basal Tempo (semanas) EPM= erro-padrão da média +p<0,01 vs. placebo . Bays HE et al Clin Ther 2001;23:
 Ezetimiba 1 mg (n=49) Ezetimiba 5 mg (n=49) Ezetimiba 10 mg (n=46) Placebo (n=52) –5. Alteração % média no LDL-C. + –10. + –15. + Slide 8. Dois estudos fase II, com 12 semanas de duração, multicêntricos, controlados com placebo, duplo-cegos, randômicos, de grupos paralelos, avaliaram a capacidade de reduzir o LDL-C do ezetimibe em monoterapia. O estudo de dose-resposta envolveu uma gama de doses de ezetimibe e seu desenho foi o seguinte: após estabilização com dieta (National Cholesterol Education Program Fase I ou dieta mais rigorosa), washout de medicamentos modificadores de lípides e um período de seis semanas com placebo, os pacientes com idade entre 18–75 anos e níveis plasmáticos de LDL-C no período basal entre 3,4 e 6,5 mmol/l (131 e. 251 mg/dl) e de triglicérides (TG) 3,4 mmol/l (300 mg/dl) foram distribuídos de modo randômico para receber 0,25 mg, 1, 5 mg ou 10 mg de ezetimibe ou placebo uma vez ao dia, antes da primeira refeição do dia. No estudo de dose-resposta (n=243), doses de 0,25 mg a 10 mg/dia de ezetimibe reduziram o LDL-C em 9,9 % a 18,7% em comparação com o placebo no final de 12 semanas (todos os valores de p<0,01 vs. placebo).3. + – Endpoint. (±EPM) Período basal. Tempo (semanas) EPM= erro-padrão da média. +p<0,01 vs. placebo. . Bays HE et al Clin Ther 2001;23:")
25
186 eventos em 4,407 homens (entre 40-65 anos)
Risco de DAC de acordo com os níveis de HDL Prospective Cardiovascular Münster Study 120 110 186 eventos em 4,407 homens (entre anos) Incidência por 1000 (em 6 anos) 30 21 < 35 35–55 > 55 HDL-C (mg/dL) Assmann G, ed. Lipid Metabolism Disorders and Coronary Heart Disease. Munich: MMV Medizin Verlag, 1993
 Incidência por (em 6 anos) < –55. > 55. HDL-C (mg/dL) Assmann G, ed. Lipid Metabolism Disorders and Coronary Heart Disease. Munich: MMV Medizin Verlag,")
26
Incidência de DAC de Acordo com os Níveis de HDL em Diversos Trials
Homens Mulheres -2 % de redução de risco para cada incremento de 1 mg/dL no HDL -4 -6 -8 -10 FHS LRCF CPPT MRFIT FHS LRCF 95% confidence intervals (CIs) for adjusted proportional hazards regression coefficients. FHS = Framingham Heart Study; LRCF = Lipid Research Clinics Prevalence Mortality Follow-up Study; CPPT = Lipid Research Clinics Coronary Primary Prevention Trial; MRFIT = Multiple Risk Factor Intervention Trial Gordon DJ et al. Circulation 1989;79:8–15
 for adjusted proportional hazards regression coefficients. FHS = Framingham Heart Study; LRCF = Lipid Research Clinics Prevalence Mortality Follow-up Study; CPPT = Lipid Research Clinics Coronary Primary Prevention Trial; MRFIT = Multiple Risk Factor Intervention Trial. Gordon DJ et al. Circulation 1989;79:8–15.")
27
Funções Potencialmente Anti-Aterogênicas da HDL
Promoção do efluxo de colesterol (transposte reverso) Propriedades anti-oxidantes Propriedades anti-trombóticas Propriedades Anti-inflammatórias Barter P. The Future Forum Conference
 Propriedades anti-oxidantes. Propriedades anti-trombóticas. Propriedades Anti-inflammatórias. Barter P. The Future Forum Conference.")
28
Efeitos de Drogas nos Níveis de HDL
Ácido Nicotínico 15–35% Fibratos 10–15% Estatinas 5–10% Ezetimibe 0–5% Belalcazar LM et al. Progress in Cardiovascular Disease 1998;41:

29
Ácido Nicotínico: Mecanismo de Ação
Mobilização de AGL Apo B VLDL sérico resulta em redução da lipólise a LDL-C VLDL VLDL Síntese de TG Secreção de VLDL LDL LDL Hepatócito Circulação HDL A niacina diminui a remoção do HDL -

30
Ácido Nicotínico: Metabolismo
Liberação Intermediária Liberação Rápida Liberação Prolongada 50% cada via Conjugação Oxidação HEPATOXICIDADE FLUSHING

31
Eficácia da Niacina de liberação Intermediária
HDL-c 30 30% 29.5% 20 26% 22% 10 15% 10% –3% –9% Alteração dos valores basais -10 –14% –12% –17% –5% –21% –17% –22% LDL-c -20 –11% –24% Lp(a) -30 –28% –30% –26% -40 –35% –44% TG –39% -50 500mg 1000 mg 1500 mg 2000 mg 2500 mg 3000 mg Goldberg A et al. Am J Cardiol 2000;85:
 -30. –28% –30% –26% -40. –35% –44% TG. –39% mg mg mg mg mg mg. Goldberg A et al. Am J Cardiol 2000;85:")
32
O QUE DIZEM AS SOCIEDADES?
OH N “Entre os agentes modificadores dos lipídios, o ácido nicotínico parece ser o mais eficaz para alterar favoravelmente todas as anormalidades lipoproteicas associadas à dislipidemia aterogênica.” Programa Nacional de Educação sobre o Colesterol Relatório do Painel III – Tratamento de Adultos Expert Panel. Circulation 2002;106:

33
O QUE DIZEM AS SOCIEDADES?
“Ácido nicotínico não é apenas o agente mais potente em aumentar o HDL-C, mas também é efetivo em reduzir componentes lipídicos aterogênicos-chave como: triglicérides, VLDL-C, LDL-C e lipoproteína (a) .” “O ácido nicotínico torna-se estratégico na dislipidemia aterogência da Síndrome Metabólica e do Diabetes Tipo 2, seja em monoterapia ou em associação a estatina.” Position Paper – European Consensus Panel on HDL-C Cur Med Res Opin 2004; 20(8):
 . O ácido nicotínico torna-se estratégico na dislipidemia aterogência da Síndrome Metabólica e do Diabetes Tipo 2, seja em monoterapia ou em associação a estatina. Position Paper – European Consensus Panel on HDL-C. Cur Med Res Opin 2004; 20(8):")
34
O QUE DIZEM AS SOCIEDADES?
“Um dos agentes de escolha para combinação com estatina é o ácido nicotínico por existirem evidências de redução no risco cardiovascular com seu uso, tanto em monoterapia quanto em terapia combinada.” “´´Ácido nicotínico não promove elevação significativa de HbA1c.” Consensus statement from American Diabetes Association e American College of Cardiology Foundation Diabetes Care 2008;31:

35
Niacina e proteção cardiovascular
Estudo Coronary Drug Project (CDP) 1,2 Stockholm Ischaemic Heart Disease study (IHD) 3 Tratamento(s) Ácido nicotínico Ácido nicotínico + clofibrato Dur. 5 anos 15 anos Resultados IM não fatal 27% Derrame/TIA 24% Mortalidade total 11% Mortalidade total 26% 1. CDP Research Group. JAMA 1975;231: Canner PL et al for the CDP Research Group. J Am Coll Cardiol 1986;8: Carlson LA & Rosenhamer G. Acta Med Scand 1988;223:405-18
 1,2. Stockholm Ischaemic Heart Disease study (IHD) 3. Tratamento(s) Ácido nicotínico. Ácido nicotínico + clofibrato. Dur. 5 anos. 15 anos. Resultados. IM não fatal 27% Derrame/TIA 24% Mortalidade total 11% Mortalidade total 26% 1. CDP Research Group. JAMA 1975;231: Canner PL et al for the CDP Research Group. J Am Coll Cardiol 1986;8: Carlson LA & Rosenhamer G. Acta Med Scand 1988;223:")
36
Niacina e proteção cardiovascular: regressão das lesões ateroscleróticas
Estudo CLAS1,2 FATS3 UCSF- SCOR4 HATS5 Tratamento(s) Ácido nicotínico + colestipol vs. placebo Ácido nicotinico + colestipol ou lovastatina + colestipol vs. controle Nicotinic acid + colestipol lovastatin + colestipol vs. cuidados usuais Ácido nicotínico + sinvastatina ± vitaminas antioxidantes vs. placebo Dur. 2-4 anos 2-5 anos 2 anos 3 anos Resultados Não-progressão: 52% drogas vs. 15% placebo Regressão: 15% drogas Não-progressão: 39% ácido nicotínico/colestipol 32% lovastatina/colestipol Regressão: 33% droga vs. 13% cuidados usuais Regressão vs. progressão: -0.4% ácido nicotínico + sinvastatina vs. +3.9% placebo 1. Blankenhorn DH et al. JAMA 1987;19;257: ; 2. Cashin-Hemphill L et al. JAMA 1990;264:3013-7; 3. Brown G et al. NEJM 1990;323: ; 4. Kane JP et al. JAMA 1990;264: ; 5. Brown BG et al NEJM 2001;345:
 Ácido nicotínico + colestipol vs. placebo. Ácido nicotinico + colestipol ou lovastatina + colestipol vs. controle. Nicotinic acid + colestipol lovastatin + colestipol vs. cuidados usuais. Ácido nicotínico + sinvastatina ± vitaminas antioxidantes vs. placebo. Dur. 2-4 anos. 2-5 anos. 2 anos. 3 anos. Resultados. Não-progressão: 52% drogas vs. 15% placebo Regressão: 15% drogas. Não-progressão: 39% ácido nicotínico/colestipol 32% lovastatina/colestipol. Regressão: 33% droga vs. 13% cuidados usuais. Regressão vs. progressão: -0.4% ácido nicotínico + sinvastatina vs. +3.9% placebo. 1. Blankenhorn DH et al. JAMA 1987;19;257: ; 2. Cashin-Hemphill L et al. JAMA 1990;264:3013-7; 3. Brown G et al. NEJM 1990;323: ; 4. Kane JP et al. JAMA 1990;264: ; 5. Brown BG et al NEJM 2001;345:")
37
FIBRATOS - síntese hepática de VLDL, lipólise de VLDL e a remoção de seus remanescentes por atividade da LLP - TG e VLDL (até 60%), CT e LDL (até 20%) e HDL (até 20%) - Escolha nas hipertrigliceridemias e nas hiperlipidemias mistas quando TG muito elevados - EC: sintomas TGI, tontura, cefaléia, insônia, colestase, da libido, mialgia e miosite, de TGO, TGP, CK e creatinina
, CT e LDL (até 20%) e. HDL (até 20%) - Escolha nas hipertrigliceridemias e nas hiperlipidemias. mistas quando TG muito elevados. - EC: sintomas TGI, tontura, cefaléia, insônia, colestase, da libido, mialgia e miosite, de TGO, TGP, CK e creatinina.")
38
Baseline LDL-C, mg/dl (mmol/L)
CHD Prevention Trials with Fibrates in Diabetic Subjects: Subgroup Analyses Baseline LDL-C, mg/dl (mmol/L) Drug Dose LDL-C Lowering CHD Reduction Study No. Primary Prevention Helsinki Heart Study Secondary Prevention VA-HIT Gemfibrozil (1200 mg/d) 135 627 203 (5.2) 112 (2.9) 6% – 68% NS 24% p=0.05 CHD Prevention Trials with Fibrates in Diabetic Subjects: Subgroup Analyses Trials of fibrate therapy that included diabetic subgroups were the primary-prevention Helsinki Heart Study and the secondary-prevention Veterans Affairs HDL Intervention Trial (VA-HIT). There were only 135 diabetic patients in the Helsinki Heart Study, and the CHD reduction was 68%, which was not statistically significant because of low power. VA-HIT had a much larger number of diabetic subjects, and this subgroup had a statistically significant 24% reduction in CHD events. In VA-HIT, mean baseline LDL cholesterol was only about 112 mg/dL; HDL cholesterol was also low at 32 mg/dL, and triglyceride levels were modest at 160 mg/dL. Gemfibrozil produced relatively little LDL cholesterol change in either study. In VA-HIT, HDL cholesterol was increased by about 6% and triglyceride was reduced by about 30% References: Koskinen P, Mänttäri M, Manninen V, Huttunen JK, Heinonen OP, Frick MH. Coronary heart disease incidence in NIDDM patients in the Helsinki Heart Study. Diabetes Care 1992;15: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: Adapted from Koskinen P et al. Diabetes Care 1992;15: ; Rubins HB et al. N Engl J Med 1999;341:
 Drug Dose. LDL-C Lowering. CHD Reduction. Study. No. Primary Prevention. Helsinki Heart Study. Secondary Prevention. VA-HIT. Gemfibrozil (1200 mg/d) (5.2) 112 (2.9) 6% – 68% NS. 24% p=0.05. CHD Prevention Trials with Fibrates in Diabetic Subjects: Subgroup Analyses. Trials of fibrate therapy that included diabetic subgroups were the primary-prevention Helsinki Heart Study and the secondary-prevention Veterans Affairs HDL Intervention Trial (VA-HIT). There were only 135 diabetic patients in the Helsinki Heart Study, and the CHD reduction was 68%, which was not statistically significant because of low power. VA-HIT had a much larger number of diabetic subjects, and this subgroup had a statistically significant 24% reduction in CHD events. In VA-HIT, mean baseline LDL cholesterol was only about 112 mg/dL; HDL cholesterol was also low at 32 mg/dL, and triglyceride levels were modest at 160 mg/dL. Gemfibrozil produced relatively little LDL cholesterol change in either study. In VA-HIT, HDL cholesterol was increased by about 6% and triglyceride was reduced by about 30% References: Koskinen P, Mänttäri M, Manninen V, Huttunen JK, Heinonen OP, Frick MH. Coronary heart disease incidence in NIDDM patients in the Helsinki Heart Study. Diabetes Care 1992;15: Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J, for the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341: Adapted from Koskinen P et al. Diabetes Care 1992;15: ; Rubins HB et al. N Engl J Med 1999;341:")
39
FIELD (200 mg dia) Fenofibrate Placebo
9795 pacientes, Idade anos, diabetes tipo 2 diagnosticado após os 35 anos, sem indicação clara de terapia com hipolipemiante no baseline (Colesterol Total mg/dL, + Colesterol Total/HDL ≥4.0 ou Triglicéries >88.6 mg/dL Fenofibrate (200 mg dia) n=4895 Placebo N=4900 Endpoints: Primario – Morte CV e IAM não-fatal após 5 anos Secondary – Composite of total CV events, CV mortality, total mortality, stroke, coronary revascularization and all revascularization at 5 year follow-up FIELD study investigators. Lancet. 2005;366:1849–1861.
 n=4895. Placebo. N=4900. Endpoints: Primario – Morte CV e IAM não-fatal após 5 anos. Secondary – Composite of total CV events, CV mortality, total mortality, stroke, coronary revascularization and all revascularization at 5 year follow-up. FIELD study investigators. Lancet. 2005;366:1849–1861.")
40
FIELD: Desfecho Primário
Morte CV e IAM não fatal após 5 anos (% em cada grupo) p=0.16 O desfecho primário não foi diferente entre o grupo tratado com fenofibrato e o grupo placebo FIELD study investigators. Lancet. 2005;366:1849–1861.
 p=0.16. O desfecho primário. não foi diferente entre. o grupo tratado com. fenofibrato e o grupo. placebo. FIELD study investigators. Lancet. 2005;366:1849–1861.")
41
FIELD: Secondary Endpoint
Componentes Individuais de Endpoint Secundário P=0.001 P=0.003 O Percentual de revascularização Coronária e todas as revascularizações foi significativamente menor no grupo fenofibrato FIELD study investigators. Lancet. 2005;366:1849–1861.

42
Associar para atingir as metas !!

43
Porque os pacientes que aderem ao tratamento não atingem as metas ?
–6% –6% –6% 20 mg 40 mg 80 mg Estatina 10 mg 10 20 30 40 50 60 % redução do LDL-C Stein E Eur Heart J Suppl 2001;3(suppl E):E11–E16.
:E11–E16.")
44
Estatina + Fibrato O risco de miopatia e rabdomiólise é potencializado nas seguintes situações: - Altas doses de estatinas - Insuficiência Renal (Cr > 2.0) - Medicações Concomitantes: Itraconazol, Ketoconazol Ciclosporina A Eritromicina - Idade > 70 anos Preferir fenofibrato Statin plus fibrate combination therapy Combining a fibrate with a statin raises safety concerns because of the potential for myopathy and overt rhabdomyolysis. However, almost all reports of such adverse effects have been in particular situations, in which one should avoid administering this drug combination. Higher doses of statins, particularly simvastatin 80 mg/d or atorvastatin 80 mg/d, should not be combined with any fibrate. Also, because fibrates are renally excreted, plasma levels are increased in patients with renal insufficiency, thereby increasing the risk for drug–drug interactions. In addition, the combination of a fibrate and a statin should not be used with agents that interfere with clearance of statins because the statin will then interact with the fibrate; the immunosuppressive agent tacrolimus may also have this effect. Finally, because of problems with renal and hepatic function, patients older than 70 years should not be treated with a fibrate plus a statin.
 - Medicações Concomitantes: Itraconazol, Ketoconazol Ciclosporina A Eritromicina. - Idade > 70 anos. Preferir fenofibrato. Statin plus fibrate combination therapy. Combining a fibrate with a statin raises safety concerns because of the potential for myopathy and overt rhabdomyolysis. However, almost all reports of such adverse effects have been in particular situations, in which one should avoid administering this drug combination. Higher doses of statins, particularly simvastatin 80 mg/d or atorvastatin 80 mg/d, should not be combined with any fibrate. Also, because fibrates are renally excreted, plasma levels are increased in patients with renal insufficiency, thereby increasing the risk for drug–drug interactions. In addition, the combination of a fibrate and a statin should not be used with agents that interfere with clearance of statins because the statin will then interact with the fibrate; the immunosuppressive agent tacrolimus may also have this effect. Finally, because of problems with renal and hepatic function, patients older than 70 years should not be treated with a fibrate plus a statin.")
45
Passos para minimizar os efeitos da interação Estatinas + Fibratos
Monoterapia com estatinas para metas de colesterol não- HDL Uso de niacina ou ezetemiba ao invés de fibratos Manter doses baixas de estatinas e fibratos Dose de fibrato pela manhã e de estatina à noite Evitar (ou usar com cautela) a combinação em pacientes com insuficiêncai renal Assegurar que não existam outras interações Ensinar o paciente a reconhecer sintomas musculares Descontinuar o tratamento se sintomas musculares e CK 10 x acima do limite superior da normalidade
 a combinação em pacientes. com insuficiêncai renal. Assegurar que não existam outras interações. Ensinar o paciente a reconhecer sintomas musculares. Descontinuar o tratamento se sintomas musculares e. CK 10 x acima do limite superior da normalidade.")
46
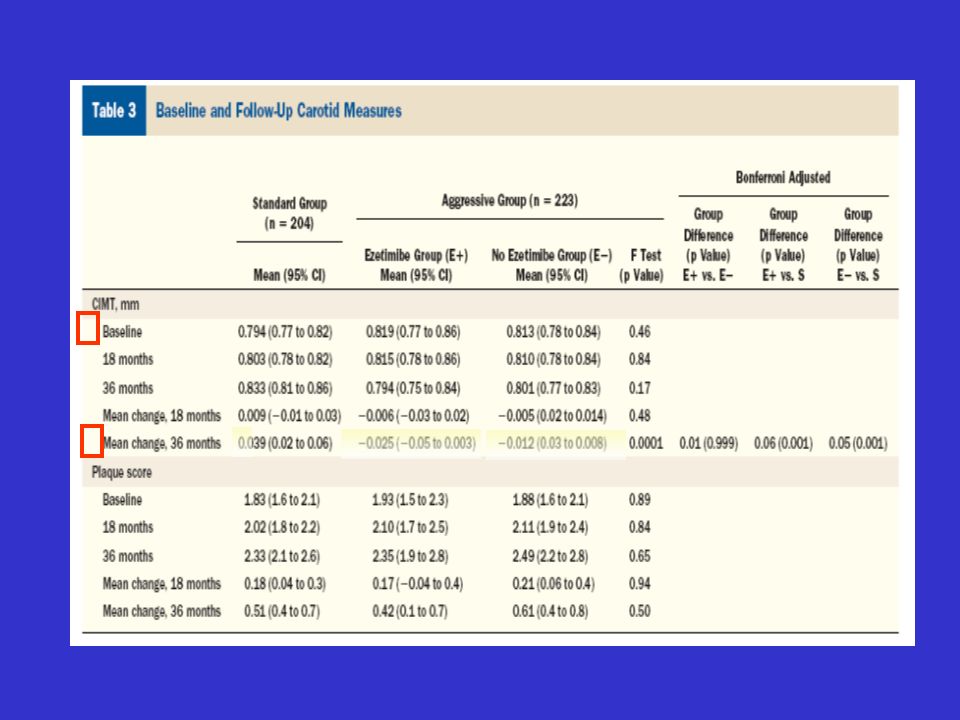
SANDS (Stop Atherosclerosis in Native Diabetics Study) (JAMA 2008;299:1678-89)
499 homens e mulheres com diabetes, sem doença arterial coronariana (DAC) 40 anos de idade PAS>130, LDL>100 Metas convencionais LDL-C <100; PAS <130 Col não-HDL <130 N=247 Metas agressivas LDL-C <70; PAS <115 Col não-HDL-C <100 N=252 Avaliação com ECO carotídeo e cardíaco no período basal, aos 18 meses e após 3 anos de intervenção Desfecho primário—alteração na EIMc
 40 anos de idade. PAS>130, LDL>100. Metas convencionais. LDL-C <100; PAS <130. Col não-HDL <130. N=247. Metas agressivas. LDL-C <70; PAS <115. Col não-HDL-C <100. N=252. Avaliação com ECO carotídeo e cardíaco. no período basal, aos 18 meses e. após 3 anos de intervenção. Desfecho primário—alteração na EIMc.")
47
Métodos Participantes nos dois grupos avaliados a cada 3 meses
Algoritmo para os lípides: Todos os pacientes receberam sinvastatina e quando a meta de LDL-C não fosse alcançada, a ezetimiba foi adicionada (o que ocorreu em 1/3 dos pacientes do grupo agressivo); Para o colesterol HDL foi associado fenofibrato ou niacina a fim de se atingir as metas.
; Para o colesterol HDL foi associado fenofibrato ou niacina a fim de se atingir as metas.")
48
Alterações Médias nos Lípides
mg/dL

50
Taylor AJ et al. Circulation 2004;110:3512-7
ARBITER 2 Estudo duplo-cego. Avaliar a variação da espessura íntima-média de carótida (EIMC) através de USG em 167 pacientes. Pacientes com DAC estabelecida com LDL abaixo de 100mg/dl (diabetes mellitus 28% & síndrome metabólica 50%). Randomizados para NLI 1 g/d ou placebo (ambos os grupos com uso de estatina). 12 meses de follow-up. 170 mg/dL 40 mg/dL 88 mg/dL Baseline T G H D L -C L D L -C Taylor AJ et al. Circulation 2004;110:3512-7
 através de USG em 167 pacientes. Pacientes com DAC estabelecida com LDL abaixo de 100mg/dl. (diabetes mellitus 28% & síndrome metabólica 50%). Randomizados para NLI 1 g/d ou placebo (ambos os grupos com. uso de estatina). 12 meses de follow-up. 170 mg/dL. 40 mg/dL. 88 mg/dL. Baseline. T G. H D L -C. L D L -C. Taylor AJ et al. Circulation 2004;110:")
51
ARBITER 2 Adapted with permission from Taylor AJ et al. Circulation 2004;110:

52
Mechanisms Contributing to Arterial Disease in Type 2 Diabetes
Ad sever/Medivia/Galida Slides/ ADA slide kit _v27 Mechanisms Contributing to Arterial Disease in Type 2 Diabetes Slide 4 Adapted from Libby et al. Circulation. 2002;106:

53
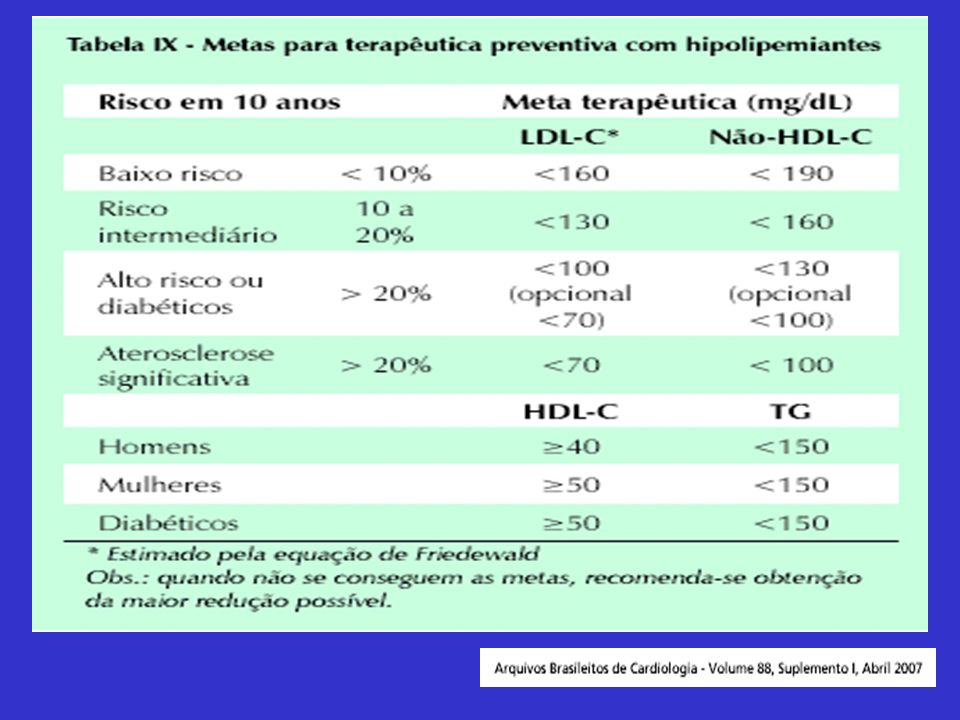
Conclusão – Metas para diminuir o RCV
Glicemia capilar pré-prandial – 110 Glicemia capilar pós-prandial 2h 140 Hba1c < % Colesterol total 200 HDL 50 LDL 100 ou 70 Triglicérides 150 IMC a 25 Pressão arterial 130 X 80

Apresentações semelhantes

















.>")

