Carregar apresentação
A apresentação está carregando. Por favor, espere

1
TRATAMENTO DA HEPATITE C CRÔNICA
Paulo Roberto Lerias de Almeida Doutor em Hepatologia Comitê Estadual de Hepatites Virais SES/RS Coordenação da Política de Assistência Farmacêutica SES/RS

2
HISTÓRIA NATURAL DA INFECÇÃO VHC
exposição VHC Seeff, Hepatology 2002 infecção aguda infecção crônica ocorre em 50%-85% pacientes cirrose desenvolve em 2%-20% pacientes anos após infecção insuficiência hepática/descompensação carcinoma hepatocelular (2%-5% dos pacientes / ano) (1%-4% dos pacientes / ano)
 (1%-4% dos pacientes / ano)")
3
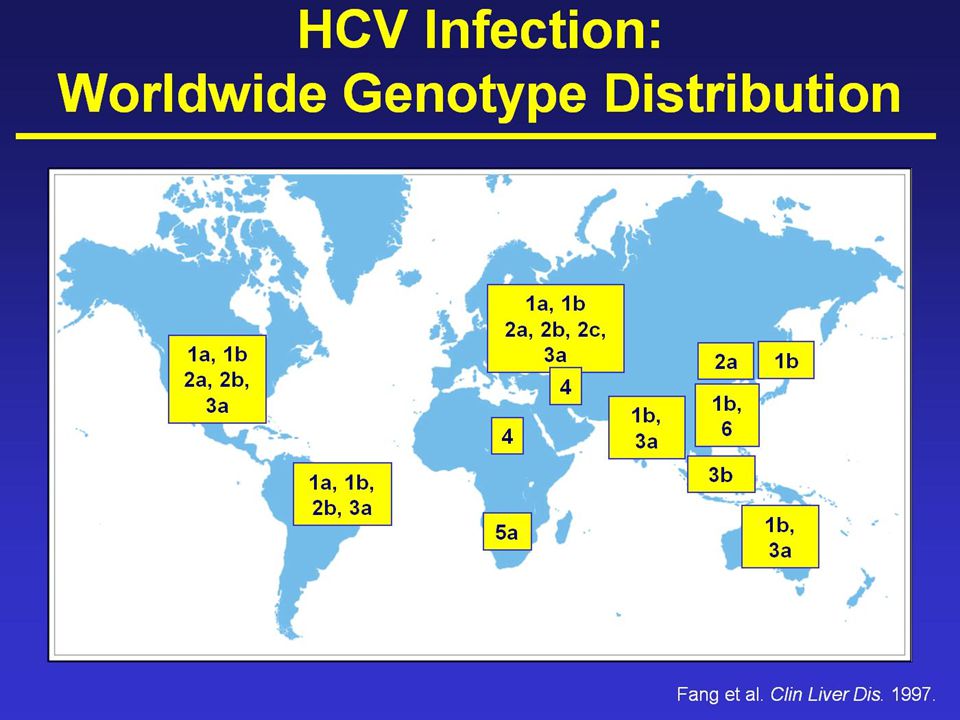
PREVALENCIA DA HEPATITE C

4
PREVALÊNCIA DA HEPATITE C
Estudo de Prevalência de Base Populacional das Infecções pelos vírus das Hepatites A, B e C nas capitais do Brasil 2.1% PREVALÊNCIA DA HEPATITE C média nacional 1,38% 10 a 69 anos DF 0.7% 0.9% 1.3% 1.3% Boletim Epidemiológico Hepatites Virais 2011 Ministério da Saúde 1.2%

6
PREVALÊNCIA DA HEPATITE C Epidemiologia da Hepatite C no Brasil : relatório da SBH GED, 1999

7
< 15% dos indivíduos com Hepatite Crônica C tratados
SES/RS PEGIFN n.o pacientes tratados 12.000 ~ 70% PCR + pacientes ? < 15% dos indivíduos com Hepatite Crônica C tratados 1,2 % anti-HCV + soropositivos Rio Grande do Sul Censo Demográfico 2010 habitantes HEPATITE C

8
Paulo Roberto Lerias de Almeida Secretaria Estadual da Saúde do RS
Doutor em Hepatologia Ministério da Saúde Comitê Assessor Departamento DST/AIDS/Hepatites Virais Hospital Nossa Senhora da Conceição Secretaria Estadual da Saúde do RS Comitê Estadual de Hepatites Virais Coordenação da Política de Assistência Farmacêutica

11
HEPATITE C – TRATAMENTO Quem tratar ?
Adultos e crianças maiores de 3 anos de idade Biópsia hepática com: - atividade inflamatória ≥ A2 e fibrose ≥F1 ou - fibrose ≥ F2 com qualquer atividade inflamatória Biópsia hepática desnecessária Biópsia hepática facultativa Cirrose Coagulopatias congênitas Manifestações extra-hepáticas Co-infecção HCV/HIV IRC Genótipo 2 e 3 Protocolo MS Portaria 221, de 13/07/2011 Modificada Ofício Circular 97/2011, de 17/08/2011

12
HEPATITE C – TRATAMENTO Quem não deve ser tratado ?
- Menores de 3 anos de idade - UDI e uso abusivo de bebidas alcoólicas que não estejam em programa de tratamento - Transplantados de pulmão, rim ou coração - Portadores de doenças auto-imunes ( IFN pode exacerbar ) - Cirrose descompensada - Co-morbidades importantes e/ou não compensadas - Gestantes - Homens e mulheres sem controle contraceptivo RBV é teratogênica Contracepção indicada até 6 m pós-tto Protocolo MS Portaria 221, de 13/07/2011 Modificada Ofício Circular 97/2011, de 17/08/2011
 - Cirrose descompensada. - Co-morbidades importantes e/ou não compensadas. - Gestantes. - Homens e mulheres sem controle contraceptivo. RBV é teratogênica. Contracepção indicada até 6 m pós-tto. Protocolo MS. Portaria 221, de 13/07/2011. Modificada Ofício Circular 97/2011, de 17/08/2011.")
13
Resistência a insulina Polimorfismo genético
A resposta ao tratamento da hepatite C com PEG-IFN e RBV é Influenciada por diversos fatores Moraes: pS54A, S55A; Davis: p648A Moraes: pS55B A, S56A; Moraes: pS54A, S55A; Fatores virais Fatores do Hospedeiro Moraes: pS54 A, S57B Davis: p648A Idade Genótipo Carga viral Gênero WHO Fact Sheet: p1A IMC Raça Fatores Sociais Pontos Importantes: O vírus da hepatite C (HCV) é um problema de saúde pública. Cerca de 130 a 170 milhões de pessoas estão cronicamente infectadas com o HCV em âmbito mundial, sendo que mais de 350 mil pessoas morrem por doenças hepáticas relacionadas com o HCV a cada ano3 A resposta ao tratamento do HCV pode ser influenciada por diversas variáveis relacionadas com fatores do vírus, do hospedeiro e sociais1,2 Informações Básicas: O genótipo do HCV é considerado o fator preditivo viral mais importante da resposta virológica sustentada (RVS) à terapia do HCV1 Muitos estudos que incluíram pacientes com genótipo 1 e genótipos 2 ou 3 demonstraram a associação entre a carga viral no período basal e a RVS, com RVS consistentemente mais elevada em pacientes com níveis baixos de ácido ribonucleico (carga viral) do HCV no período basal, independentemente do genótipo1 Vários estudos de pequeno porte observaram que pacientes afro-americanos com infecção crônica pelo HCV apresentam menores taxas de resposta à terapia antiviral em comparação com caucasianos1 O consumo de álcool pode reduzir a RVS indiretamente ao aumentar a replicação do HCV1 Resistência a insulina WHO Fact Sheet: p1A Adesão Consumo de álcool Moraes: pS54A, pS55A; Davis: p648A Fibrose Polimorfismo genético Moraes: pS55B Moraes: pS56A Moraes: pS57A Moraes: pS57B Moraes Coelho HS et al. Ann Hepatol. 2010;9(suppl):S54–S60. Davis GL et al. Hepatology. 2003;38:645–652. Folha de dados de hepatite C. Site da Organização Mundial da Saúde. Acessado em 23 de setembro de 2011. 13
 é um problema de saúde pública. Cerca de 130 a 170 milhões de pessoas estão cronicamente infectadas com o HCV em âmbito mundial, sendo que mais de 350 mil pessoas morrem por doenças hepáticas relacionadas com o HCV a cada ano3. A resposta ao tratamento do HCV pode ser influenciada por diversas variáveis relacionadas com fatores do vírus, do hospedeiro e sociais1,2. Informações Básicas: O genótipo do HCV é considerado o fator preditivo viral mais importante da resposta virológica sustentada (RVS) à terapia do HCV1. Muitos estudos que incluíram pacientes com genótipo 1 e genótipos 2 ou 3 demonstraram a associação entre a carga viral no período basal e a RVS, com RVS consistentemente mais elevada em pacientes com níveis baixos de ácido ribonucleico (carga viral) do HCV no período basal, independentemente do genótipo1. Vários estudos de pequeno porte observaram que pacientes afro-americanos com infecção crônica pelo HCV apresentam menores taxas de resposta à terapia antiviral em comparação com caucasianos1. O consumo de álcool pode reduzir a RVS indiretamente ao aumentar a replicação do HCV1. Resistência a insulina. WHO Fact Sheet: p1A. Adesão. Consumo de álcool. Moraes: pS54A, pS55A; Davis: p648A. Fibrose. Polimorfismo genético. Moraes: pS55B. Moraes: pS56A. Moraes: pS57A. Moraes: pS57B. Moraes Coelho HS et al. Ann Hepatol. 2010;9(suppl):S54–S60. Davis GL et al. Hepatology. 2003;38:645–652. Folha de dados de hepatite C. Site da Organização Mundial da Saúde. Acessado em 23 de setembro de")
14
Porquê ? MAXIMIZAR A ADESÃO

15
N = 3070 74 70 61 Peg2b1,5/ R Peg2b1,0/ R Peg2a/ R 20 16 10 80/80/80 não 80/80/80 McHutchison JG et al, NEJM, 361(1)580-93, 2009
580-93,")
16
CAPACITAÇÃO E PERÍCIA DA EQUIPE
Como ? CAPACITAÇÃO E PERÍCIA DA EQUIPE

17
Seguimento Farmacoterapêutico na Hepatite C Crônca
Experiência de um Centro de Referência CAMMI Hospital Nossa Senhora da Conceição Coorte tratamentos com PEG/RBV 745 pacientes intervenções farmacêuticas : 311 (42%) pacientes Contato farmacêutico-médico : 264 (35%) pacientes; média 2,4/paciente (1-14) tratamentos suspensos por RAM: 78 (11%) abandono de tratamento: 14 (2%) Feltrin A, Costa G, Bynstronsky, Camargo A, Almeida P Congresso da Sociedade Brasileira de Farmácia Hospitalar, Salvador 2011
 pacientes. Contato farmacêutico-médico : 264 (35%) pacientes; média 2,4/paciente (1-14) tratamentos suspensos por RAM: 78 (11%) abandono de tratamento: 14 (2%) Feltrin A, Costa G, Bynstronsky, Camargo A, Almeida P. Congresso da Sociedade Brasileira de Farmácia Hospitalar, Salvador")
18
HEPATITE C – TRATAMENTO G2 e G3 - Como tratar ?
Sem fatores preditivos de má resposta - IFN convencional 3 MU 3x/sem + Ribavirina 15 mg/kg/d - 24 semanas Com fatores preditivos de má resposta - PegIFN + Ribavirina 15 mg/kg/d - 24 a 48 semanas Cirrose clínica ou Escore METAVIR F3/F4 ou CV > UI/mm3 Fatores preditivos de má resposta Protocolo MS - Portaria 221, de 13/07/2011 Modificada Ofício Circular 97/2011, de 17/08/2011

19
Protocolo MS - Portaria 221, de 13/07/2011
Modificada Ofício Circular 97/2011, de 17/08/2011

20
HEPATITE C – TRATAMENTO Como tratar ?
Genótipo 1 ► 48 semanas ► RBV: 15 mg/kg/d ► PEG-IFN α2b 1,5ug/kg/sem PEG-IFN α2a 180 ug/sem Protocolo MS Portaria 221, de 13/07/2011 Modificada Ofício Circular 97/2011, de 17/08/2011

21
Protocolo MS - Portaria 221, de 13/07/2011 Modificada Ofício Circular 97/2011, de 17/08/2011

22
Tratamento atual da hepatite C
PEGINTERFERON + RIBAVIRINA , SEMANAS , MONOINFECTADOS FIBROSE AVANÇADA Manns: F3+F % Fried: F % Hadzyiannis: F3+F % SES: F3+F % Prophesys: F % % RVS 35 G1 G2/3 Manns Manns Fried Fried Hadziyannis SES/RS Hadziyannis Almeida PRL et al, Hepatogastroenterol 2009

23
Hepatogastroenterology, 2009
Paulo R L Almeida Hepatogastroenterology, 2009 INÍCIO TRATAMENTO 323 SEM RVP 75 EFEITOS ADVERSOS 33 SEM 12 23,2% 10,2% SEM 48 215 PCR Θ 169 RVS 35,3% PCR 46 66,6% 52,3% 14,3% PCR 52 PCR 114 3 perdas SEMANA 72

24
Mortalidade em pacientes VHC em tratamento PEG + RIBAVIRINA - um estudo de “vida real” -
CAMMI (Centro Aplicação e Monitorização Medicamentos Injetáveis da SES) Hospital Nossa Senhora da Conceição – Porto Alegre março 2004 – junho 2013 1059 pacientes: (27%) cirrose 776 (73%) não cirrose Mortalidade global 18 mortes (1.7%) Pôster 2383 , Congresso Brasileiro de Hepatologia, RJ, outubro/2013
 Hospital Nossa Senhora da Conceição – Porto Alegre. março 2004 – junho pacientes: 283 (27%) cirrose. 776 (73%) não cirrose. Mortalidade global. 18 mortes (1.7%) Pôster 2383 , Congresso Brasileiro de Hepatologia, RJ, outubro/2013.")
25
Mortalidade em pacientes VHC tratados com PEG+RIBAVIRINA - um estudo de “vida real” -
% 18/1059 05/776 13/283

26
A EVOLUÇÃO DO TRATAMENTO
HEPATITE CRÔNICA C A EVOLUÇÃO DO TRATAMENTO ? 2015 ?... pegIFN pegIFN ? pegIFN Inibidor HCV Inibidor HCV Ribavirina Ribavirina Inibidor HCV Ribavirina ? Inibidor HCV Boceprevir Telaprevir

27
Tratamento do HCV Genótipo 1
Boceprevir Telaprevir + Peg IFN Ribavirina

28
Tratamento do HCV Genótipo 1
Boceprevir Telaprevir + Peg IFN Ribavirina

29
SPRINT-2 naive, gen 1, Boceprevir
RVRe PCR indetectável semana 8 e semana 24 Sem 8 Teste Sem 24 Teste Lead-in P + R B+P+R 24 semanas RVR Follow-up BOC/TGR N=368 no RVR placebo +P+R 20 semanas Follow-up não RVRe PCR + semana 8 e PCR Θ semana 24 P + R B+P+R 44 semanas Follow-up BOC/PR48 N=366 P + R placebo +P+R 44 semanas Follow-up 48 P/R N=363 36 24 12 48 60 8 4 28 72 Poordad et al., N Engl J Med 2011;364: 29 29

30
RVRe PCR indetectável semana 8 e semana 12 32 semanas não RVRe
Teste Sem 12 Teste 32 semanas não RVRe PCR + semana 8 e PCR Θ semana 12 44 semanas 44 semanas

31
Tratamento do HCV Genótipo 1
Boceprevir Telaprevir + Peg IFN Alfa 2a Ribavirina

32
RVRe PCR indetectável semana 4 e semana 12
Teste Sem 12 Teste Jacobson IM et al, NEJM 2011; 364(25):
:")
33
Zeuzem S et al, NEJM 2011; 364(25): 2417-28
:")
34
TELAPREVIR E BOCEPREVIR em pacientes naïves: RVS
Estudo ADVANCE TELAPREVIR Estudo SPRINT -2 BOCEPREVIR 69 67 75 69 53 42 44 40 23 34

35
TELAPREVIR E BOCEPREVIR
em retratamentos: RVS Estudo REALIZE TELAPREVIR Estudo RESPOND -2 BOCEPREVIR 86 75 69 57 52 40 31 29 24 15 5 7 35

36
Boceprevir e Telaprevir: Eficácia conforme diferentes grupos
100 75-83[1,2] 80 68-75[3,4] 42-62[3,4] 53-62[3,4] 60 40-59[1,2] RVS (%) 29-40[1,5] 40 20 SVR, sustained virologic response; TVR, telaprevir. On this slide, these are the pooled arms in phase III clinical trials of boceprevir and telaprevir, analysis was performed based on prior treatment response history, such that relapsers experienced excellent rates of response when subsequently retreated with peg, ribavirin, and telaprevir or boceprevir. Partial responders did less well, and null responders did least well. Null responders are defined as those patients who failed to experience a 2 log or greater HCV RNA decline with peginterferon- and ribavirin-based therapy. You will note that in subgroups that included cirrhotics—so when histology was considered, cirrhotic null responders had an even more poor response, namely, 14% in the REALIZE trial. So it’s fairly clear, then, that there is a descending order of efficacy based on the difficult-to-treat nature of the patients, whether it’s in regard to prior null response or advanced liver histology. 14[6]* Recidivantes Naive Caucasianos Naive Cirróticos Naive Negros Resp Parciais Cirróticos Resp Nulos Resp Nulos 1. Zeuzem S, et al. N Engl J Med. 2011;364: Bacon BR, et al. N Engl J Med. 2011;364: Jacobson IM, et al. N Engl J Med. 2011;364: Poordad F, et al. N Engl J Med. 2011;364: Bronowicki J, et al. EASL Abstract Zeuzem S, et al. EASL Abstract 5. *estudo REALIZE 36 36 36
 29-40[1,5] SVR, sustained virologic response; TVR, telaprevir. On this slide, these are the pooled arms in phase III clinical trials of boceprevir and telaprevir, analysis was performed based on prior treatment response history, such that relapsers experienced excellent rates of response when subsequently retreated with peg, ribavirin, and telaprevir or boceprevir. Partial responders did less well, and null responders did least well. Null responders are defined as those patients who failed to experience a 2 log or greater HCV RNA decline with peginterferon- and ribavirin-based therapy. You will note that in subgroups that included cirrhotics—so when histology was considered, cirrhotic null responders had an even more poor response, namely, 14% in the REALIZE trial. So it’s fairly clear, then, that there is a descending order of efficacy based on the difficult-to-treat nature of the patients, whether it’s in regard to prior null response or advanced liver histology. 14[6]* Recidivantes. Naive Caucasianos. Naive Cirróticos. Naive Negros. Resp Parciais. Cirróticos Resp Nulos. Resp. Nulos. 1. Zeuzem S, et al. N Engl J Med. 2011;364: Bacon BR, et al. N Engl J Med. 2011;364: Jacobson IM, et al. N Engl J Med. 2011;364: Poordad F, et al. N Engl J Med. 2011;364: Bronowicki J, et al. EASL Abstract Zeuzem S, et al. EASL Abstract 5. *estudo REALIZE")
37
Boceprevir & Telaprevir Aumento significativo taxas RVS
Tratamento com Boceprevir & Telaprevir Aumento significativo taxas RVS Aumento complexidade Aumento paraefeitos Aumento dos riscos Aumento dos custos Baixa RVS em subgrupos

38
AVALIAR PREDITORES DE RVS
Otimização da terapia tripla QUANDO PODEMOS ENCURTAR ? QUANDO DEVEMOS INTERROMPER ? TERAPIA TRIPLA OU DUPLA ? 38

39
QUANDO DEVEMOS INTERROMPER ?
...o valor das “ Regras de Parada ” Otimização da terapia tripla QUANDO DEVEMOS INTERROMPER ? 39

40
REGRAS DE PARADA ( STOPPING RULES)
Regras que buscam identificar pacientes que não irão responder à TT e que podem ser precocemente identificados através dos níveis de HCVRNA em determinados momentos do tratamento. Previne desenvolvimento de resistência, minimiza efeitos adversos e racionaliza custos, frente a um paciente com mínimas ou nulas chances de obter RVS

41
(NAÏVES E EXPERIMENTADOS) (NAÏVES E EXPERIMENTADOS)
TELAPREVIR (NAÏVES E EXPERIMENTADOS) >1.000 (mil) UI semana 4 ou 12 Qualquer VIREMIA semana 24 Hepatology 2012;56: BOCEPREVIR (NAÏVES E EXPERIMENTADOS) >100 (cem) UI semana 12 Qualquer VIREMIA semana 24 Liver International 2013;33:IS s1:23-29
 >1.000 (mil) UI semana 4 ou 12. Qualquer VIREMIA semana 24. Hepatology 2012;56: BOCEPREVIR. (NAÏVES E EXPERIMENTADOS) >100 (cem) UI semana 12. Qualquer VIREMIA semana 24. Liver International 2013;33:IS s1:")
42
Protocolo Brasileiro Janeiro 2013 F3 e F4 - naives e retrat
F2 - retratamentos

43
“ REGRA DE PARADA ”

44
“ REGRA DE PARADA ”

45
Experiência do CAMMI HNSC – PoA Judiciais e acesso expandido (2011-2013)
24 pacientes em terapia tripla (12 B + 12 T) n = 24 13 (54%) F4 01 por EAS (4,1%) 04 por não resposta (16.6%) 19 (79,1%) finalizaram o tratamento 14 (58,3%) com CV indetectável 05 (20,8%) com CV detectável 02 (8,3%) recidivantes 11 (45,8%) com RVS 01 (4,1%) aguarda CV da semana 24 pós tto Almeida PRL,Tovo CV. Submetido, 2014
 n = (54%) F4. 01 por EAS (4,1%) 04 por não resposta (16.6%) 19 (79,1%) finalizaram o tratamento. 14 (58,3%) com CV indetectável. 05 (20,8%) com CV detectável. 02 (8,3%) recidivantes. 11 (45,8%) com RVS. 01 (4,1%) aguarda CV da semana 24 pós tto. Almeida PRL,Tovo CV. Submetido,")
46
Experiência do CAMMI HNSC – PoA De acordo com o protocolo do MS (a partir de agosto/2013)
Boceprevir iniciados 16 (55%) cirróticos 13 (45%) ñ cirróticos Telaprevir 68 iniciados 34 (50%) cirróticos 34 (50%) ñ cirróticos
 cirróticos. 13 (45%) ñ cirróticos. Telaprevir. 68 iniciados. 34 (50%) cirróticos. 34 (50%) ñ cirróticos.")
47
Experiência do CAMMI HNSC – PoA De acordo com o protocolo do MS (a partir de agosto/2013)
Boceprevir iniciados 05 (17%) interromperam 04 por não resposta (14%) 01 por EAS (3%) Telaprevir 68 iniciados 09 (13%) interromperam 04 por não resposta (6%) 05 por EAS (7%) 1 óbito = 1.03 %
 interromperam. 04 por não resposta (14%) 01 por EAS (3%) Telaprevir. 68 iniciados. 09 (13%) interromperam. 04 por não resposta (6%) 05 por EAS (7%) 1 óbito = 1.03 %")
48
Boceprevir e Telaprevir Limitações e Desafios
EVENTOS ADVERSOS MAIS FREQUENTES Anemia e neutropenia Disgeusia Rash Sintomas anoretais DESAFIOS À ADESÃO múltiplos comprimidos e dose TID ingestão obrigatória com lanche/refeição BOC, boceprevir; EPO, epoetin alfa; N/A, not applicable; PI, protease inhibitor; PR, peginterferon/ribavirin; RGT, response-guided therapy; T12, telaprevir for 12 weeks. The addition of a protease inhibitor unfortunately relies on a preexisting backbone of peginterferon and ribavirin. So it’s not surprising, therefore, that adverse events not only related to the inclusion of a peginterferon/ribavirin regimen, but those attributable to the addition of the protease inhibitor itself, are in fact even more common in persons on triple therapy compared to those on double therapy, and that’s illustrated in this slide. In particular, when one considers rash, there was a higher discontinuation rate because of the telaprevir-specific rash that did produce grade 3 or higher rash in 7% of patients in the triple therapy arm compared to 1% in the peg/ribavirin control arm. Furthermore, anemia was a major problem in both the ADVANCE and SPRINT-2 trials insofar as there was an excess frequency of anemia and even more severe anemia seen in the triple-therapy arms compared to the double-therapy arms. And moreover, when one considers the SPRINT-2 trial and the boceprevir registrational trial, where the use of erythropoiesis-stimulating agents was permitted, there was a very high frequency of use of EPO among those patients receiving triple therapy. So adverse effects are in fact common, and even more common, in the triple-therapy context. 48

49
Rash cutâneo Rash Grau 3 4% - 6%

50
Boceprevir e Telaprevir Limitações e Desafios
TOLERABILIDADE MENOR EM CIRRÓTICOS (estudo CUPIC) eventos adversos sérios: 29% - 51% anemia < 10 g/d: 37% - 46% transfusão: 6% - 18% INTERAÇÕES MEDICAMENTOSAS com drogas de uso frequente na prática clínica BOC, boceprevir; EPO, epoetin alfa; N/A, not applicable; PI, protease inhibitor; PR, peginterferon/ribavirin; RGT, response-guided therapy; T12, telaprevir for 12 weeks. The addition of a protease inhibitor unfortunately relies on a preexisting backbone of peginterferon and ribavirin. So it’s not surprising, therefore, that adverse events not only related to the inclusion of a peginterferon/ribavirin regimen, but those attributable to the addition of the protease inhibitor itself, are in fact even more common in persons on triple therapy compared to those on double therapy, and that’s illustrated in this slide. In particular, when one considers rash, there was a higher discontinuation rate because of the telaprevir-specific rash that did produce grade 3 or higher rash in 7% of patients in the triple therapy arm compared to 1% in the peg/ribavirin control arm. Furthermore, anemia was a major problem in both the ADVANCE and SPRINT-2 trials insofar as there was an excess frequency of anemia and even more severe anemia seen in the triple-therapy arms compared to the double-therapy arms. And moreover, when one considers the SPRINT-2 trial and the boceprevir registrational trial, where the use of erythropoiesis-stimulating agents was permitted, there was a very high frequency of use of EPO among those patients receiving triple therapy. So adverse effects are in fact common, and even more common, in the triple-therapy context. 50
 eventos adversos sérios: 29% - 51% anemia < 10 g/d: 37% - 46% transfusão: 6% - 18% INTERAÇÕES MEDICAMENTOSAS. com drogas de uso frequente na prática clínica. BOC, boceprevir; EPO, epoetin alfa; N/A, not applicable; PI, protease inhibitor; PR, peginterferon/ribavirin; RGT, response-guided therapy; T12, telaprevir for 12 weeks. The addition of a protease inhibitor unfortunately relies on a preexisting backbone of peginterferon and ribavirin. So it’s not surprising, therefore, that adverse events not only related to the inclusion of a peginterferon/ribavirin regimen, but those attributable to the addition of the protease inhibitor itself, are in fact even more common in persons on triple therapy compared to those on double therapy, and that’s illustrated in this slide. In particular, when one considers rash, there was a higher discontinuation rate because of the telaprevir-specific rash that did produce grade 3 or higher rash in 7% of patients in the triple therapy arm compared to 1% in the peg/ribavirin control arm. Furthermore, anemia was a major problem in both the ADVANCE and SPRINT-2 trials insofar as there was an excess frequency of anemia and even more severe anemia seen in the triple-therapy arms compared to the double-therapy arms. And moreover, when one considers the SPRINT-2 trial and the boceprevir registrational trial, where the use of erythropoiesis-stimulating agents was permitted, there was a very high frequency of use of EPO among those patients receiving triple therapy. So adverse effects are in fact common, and even more common, in the triple-therapy context. 50.")
51
TRATAMENTO DA HEPATITE C
NOVAS DROGAS - NOVAS ESTRATÉGIAS 2013 O TRATAMENTO IDEAL Quando o vírus necessita substitução de ≥3 aa para desenvolver resistência Potência elevada Posologia fácil tudo via oral, uma tomada diária, poucos comprimidos Alta barreira genética à resistência viral IFN, interferon; pegIFN, peginterferon; RBV, ribavirin. So what are the key elements of an ideal HCV regimen? First it should be of course highly effective, with high efficacy in traditionally challenging populations, including those patients with limited interferon sensitivity and those patients with advanced liver disease, such as cirrhotics. It should be easily administered: Once daily, with a low pill burden, would be ideal. An all-oral regimen, in which peginterferon/ribavirin have been replaced by an oral backbone with a minimal development of resistance. Pan-genotypic regimens, one that can be used not across not just genotype 1, 2 and 3, but even other genotypes such as 4, 5, and 6. It should be simple: short duration, with simple and straightforward stopping rules. And it should be of course safe and tolerable, with few or easily manageable adverse events. Regimes simples Curta duração, s/ regras de parada Pan-Genotípica Segurança Tolerabilidade poucos EA fáceis de manejar 51

52
DROGAS

53
Ciclo do VHC e Alvos dos DAA
Receptor binding and endocytosis Transport and release Fusion and uncoating Agentes anti-alvos do hospedeiro Inibidores cyclophilina ER lumen (+) RNA Virion assembly LD LD NS3/4 protease inhibitors Translation and polyprotein processing DAAs, direct-acting antivirals; ER, endoplasmic reticulum; HCV, hepatitis C virus; LD, luminal domain. The elucidation of the life cycle of the hepatitis C virus (HCV) allowed for the identification of potential targets of antivirals that directly interrupt HCV replication. From the binding of the virus to the plasma membrane and its endocytosis through the membrane, all the way through uncoating and generating the membranous web to translation and replication, viral assembly, and transport and release again into the extracellular space, one may envision a variety of potential targets. The most obvious targets are the NS3/4 serine protease and the NS5B HCV polymerase. Therefore, our first DAAs have been protease inhibitors and nucleoside or nonnucleoside polymerase inhibitors. Also interesting was the recent discovery of NS5A inhibitors that are inhibitors of the NS5A protein. However, the function of this protein in the hepatitis C life cycle is not yet well understood. Therefore, the inhibitory drugs may help to elucidate the involvement of this protein in the HCV life cycle rather than vice versa. LD Membranous web NS5B polymerase inhibitors Nucleoside/nucleotide Nonnucleoside RNA replication ER lumen *Role in HCV life cycle not well defined NS5A* inhibitors Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6: 53
 RNA. Virion assembly. LD. LD. NS3/4 protease inhibitors. Translation and polyprotein processing. DAAs, direct-acting antivirals; ER, endoplasmic reticulum; HCV, hepatitis C virus; LD, luminal domain. The elucidation of the life cycle of the hepatitis C virus (HCV) allowed for the identification of potential targets of antivirals that directly interrupt HCV replication. From the binding of the virus to the plasma membrane and its endocytosis through the membrane, all the way through uncoating and generating the membranous web to translation and replication, viral assembly, and transport and release again into the extracellular space, one may envision a variety of potential targets. The most obvious targets are the NS3/4 serine protease and the NS5B HCV polymerase. Therefore, our first DAAs have been protease inhibitors and nucleoside or nonnucleoside polymerase inhibitors. Also interesting was the recent discovery of NS5A inhibitors that are inhibitors of the NS5A protein. However, the function of this protein in the hepatitis C life cycle is not yet well understood. Therefore, the inhibitory drugs may help to elucidate the involvement of this protein in the HCV life cycle rather than vice versa. LD. Membranous web. NS5B polymerase inhibitors. Nucleoside/nucleotide. Nonnucleoside. RNA replication. ER lumen. *Role in HCV life cycle not well defined. NS5A* inhibitors. Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6:")
54
(Simeprevir) Aprovada (Faldaprevir) Em aprovação Em aprovação (Sofosbuvir) Aprovada Em aprovação (Ledipasvir) Pawlotsky JM, F1000 Biology Reports 2012, 4:5, pg 1-7
 Pawlotsky JM, F1000 Biology Reports 2012, 4:5, pg 1-7.")
55
TRATAMENTO DA HEPATITE C
NOVAS DROGAS - NOVAS ESTRATÉGIAS 2014 Inibidores Protease 1.a Inibidores Protease 2.a Inibidores NS5A a Inibidores NS5A a Inibidores Polimerase N Nucleosíd Inibidores Polimerase Nucleosíd Potência Barreira Genética Atividade Pangenotípica Efeitos Adversos Interação com drogas Fried, EASL 2014 Perfil bom Perfil médio Perfil desfavorável

56
NOVAS DROGAS DAA APROVADAS
Sofosbuvir Análogo Nucleotídeo 400 mg qd Todos Genótipos Alta barreira Simeprevir Inibidor De Protease 150 mg qd Genótipos 1 e 4 Baixa barreira

57
ESTRATÉGIAS

58
NOVOS REGIMES TRIPLOS / QUÁDRUPLOS
FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS Faldaprevir Asunaprevir (IP) MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) GS8558 (NS5A) Daclatasvir + Asunaprevir GS G59451 PR + Boceprevir ou Telaprevir Genótipo 1 PR + Simeprevir(IP) Genótipo 1 REGIMES COM PEGIFN PR + Sofosbuvir(NUC) Genótipos 1,4,5,6 2013 2014 2015 2016 2017 FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV Faldaprevir (IP) + BI (NNuc) + RBV Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV GS5885(NS5A) + Sofosbuvir(Nuc) + RBV GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV Asunaprevir (IP) + Daclatasvir (NS5A) + BMS791325 RBV + Sofosbuvir(NUC) Genótipo 2 e 3 REGIMES SEM PEGIFN Thomas Berg, EASL 2013
 MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) GS8558 (NS5A) Daclatasvir + Asunaprevir. GS G PR. + Boceprevir. ou. Telaprevir. Genótipo 1. PR + Simeprevir(IP) Genótipo 1. REGIMES COM PEGIFN. PR + Sofosbuvir(NUC) Genótipos 1,4,5, FASE III. NOVOS REGIMES TRIPLOS / QUÁDRUPLOS. ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV. Faldaprevir (IP) + BI (NNuc) + RBV. Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV. GS5885(NS5A) + Sofosbuvir(Nuc) + RBV. GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV. Asunaprevir (IP) + Daclatasvir (NS5A) + BMS RBV + Sofosbuvir(NUC) Genótipo 2 e 3. REGIMES SEM PEGIFN. Thomas Berg, EASL")
59
NOVAS DROGAS : SOFOSBUVIR & SIMEPREVIR

60
NOVAS DROGAS : SOFOSBUVIR & SIMEPREVIR
gen 1,2,3,4,5,6

61
NOVAS DROGAS : SOFOSBUVIR & SIMEPREVIR
genótipo 1

62
Sofosbuvir + Simeprevir c/s RBV
em HCV G1 Estudo COSMOS Fase II RVS % 26/27 13/14 16/16 25/27 13/14 28/30 14/15 19/24 12 sem 24 sem 12 sem 24 sem SS+R SS SS+R SS SS+R SS SS+R SS Jacobson et al, AASLD 2013; Lawitz et al, EASL 2014 62

63
Sofosbuvir + Daclatasvir c/s RBV em HCV G1
Sulkowski et al, NEJM 2014

64
NOVOS REGIMES TRIPLOS / QUÁDRUPLOS
FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS REGIMES COM PEGIFN Asunaprevir (IP) MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) Ledipasvir (NS5A) Daclatasvir + Asunaprevir GS G59451 Tripla - 2ª ger. IP Faldaprevir Simeprevir Tripla - NUC Sofosbuvir Genótipos 1,4,5,6 2013 2014 2015 2016 2017 REGIMES SEM PEGIFN FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV Faldaprevir (IP) + BI (NNuc) + RBV Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV Ledipasvir(NS5A) + Sofosbuvir(Nuc) +/- RBV GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV Asunaprevir (IP) + Daclatasvir (NS5A) + BMS791325 Simeprevir + Sofosbuvir c/s RBV NUC+ RBV Sofosbuvir Genótipo 2 e 3 Thomas Berg, EASL 2013
 MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) Ledipasvir (NS5A) Daclatasvir + Asunaprevir. GS G Tripla - 2ª ger. IP. Faldaprevir. Simeprevir. Tripla - NUC. Sofosbuvir. Genótipos 1,4,5, REGIMES SEM. PEGIFN. FASE III. NOVOS REGIMES TRIPLOS / QUÁDRUPLOS. ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV. Faldaprevir (IP) + BI (NNuc) + RBV. Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV. Ledipasvir(NS5A) + Sofosbuvir(Nuc) +/- RBV. GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV. Asunaprevir (IP) + Daclatasvir (NS5A) + BMS Simeprevir + Sofosbuvir c/s RBV. NUC+ RBV. Sofosbuvir. Genótipo 2 e 3. Thomas Berg, EASL")
65
REGIMES SEM PegIFN sem/com RBV Gen 1 Naives
FASE II/III REGIMES SEM PegIFN sem/com RBV Gen 1 Naives Fried M, EASL 2014 Regime DAA N Duração Tratamento RVS Asunaprevir (IP) Daclatasvir C/S RBV 419 12 W 99-100% Daclatasvir (NS5A) BMS (NNuc/75 ou 150 mg) 166 12 w 92% ABT-450/r (IP;100/200 mg) ABT-267 (NS5A) ABT-333 (NNuc) RBV 96% Ledispavir (NS5A) Sofosbuvir (Nuc) 431 647 12-24 w 8-12 W 97-99% 93-95% MK-5172 (IP) MK-8742 (NS5A) C/Rib 52 S/Rib 13(G1b) 89-96% 100% PEARL-3 SAPHIRE-1 473 TURQUOISE-2 (CIRRÓTICOS) 208 ION-1 ION-3 C-WORTHY
 Daclatasvir. C/S RBV W % Daclatasvir (NS5A) BMS (NNuc/75 ou 150 mg) w. 92% ABT-450/r (IP;100/200 mg) ABT-267 (NS5A) ABT-333 (NNuc) RBV. 96% Ledispavir (NS5A) Sofosbuvir (Nuc) w W % 93-95% MK-5172 (IP) MK-8742 (NS5A) C/Rib 52. S/Rib 13(G1b) 89-96% 100% PEARL-3. SAPHIRE TURQUOISE-2. (CIRRÓTICOS) 208. ION-1. ION-3. C-WORTHY.")
66
REGIMES SEM PegIFN sem/com RBV Gen 1 Retratamento
FASE II/III Regime DAA N Duração Tratamento RVS ABT-450/r (IP;100/200 mg) ABT-267 (NS5A) ABT-333 (NNuc) RBV 208 172 12 w 24 W 96% Ledispavir (NS5A) Sofosbuvir (Nuc) C/S RBV 220 94-96% 99% Asunaprevir (IP) Daclatasvir (NNuc) 222 24 w 81-88% SAPHIRE-2 TURQUOISE-2 (CIRRÓTICOS) ION-2 1.Everson et al; p 1423 EASL 2013; 2.Kewdley KV et al.J Hepatol 2013(Suppl)S2 #3 EASL 2013; 3.Gane E et al. J Hepatol2013 (Suppl) S7#14 EASL2013
 ABT-267 (NS5A) ABT-333 (NNuc) RBV w. 24 W. 96% Ledispavir (NS5A) Sofosbuvir (Nuc) C/S RBV % 99% Asunaprevir (IP) Daclatasvir (NNuc) w % SAPHIRE-2. TURQUOISE-2. (CIRRÓTICOS) ION-2. 1.Everson et al; p 1423 EASL 2013; 2.Kewdley KV et al.J Hepatol 2013(Suppl)S2 #3 EASL 2013; 3.Gane E et al. J Hepatol2013 (Suppl) S7#14 EASL2013.")
67
DIRETRIZES INTERNACIONAIS
DIRETRIZES ADAPTADAS ÀS DIVERSIDADES REGIONAIS

69
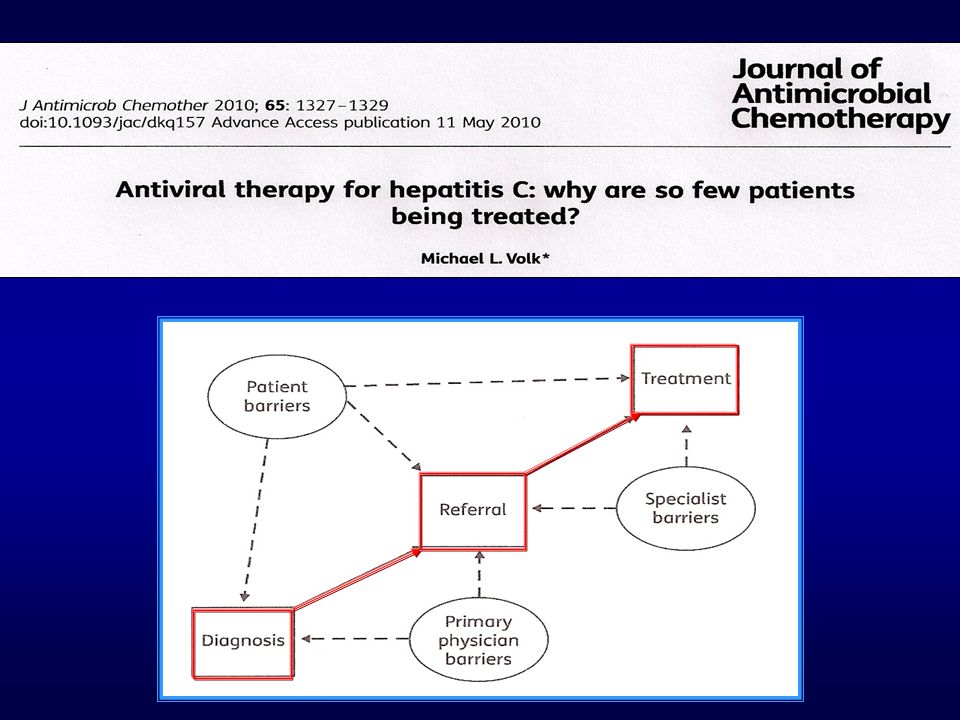
WHO hepatitis C treatment guidelines
EASL, Londres abril/2014 Topics for WHO hepatitis C screening, care and treatment guidelines Screening Care Treatment When to start treatment ? What medicines to use ? Who should be tested ? When to confirm(PCR) ? Awareness Diagnosis Referral Disease-stage assessment Treatment Monitoring How to assess degree of fibrosis ? What intervention to slow progression ? How monitor response ? and drug reactions ?
 Awareness. Diagnosis. Referral. Disease-stage. assessment. Treatment. Monitoring. How to assess degree of fibrosis What intervention to slow progression How monitor response and drug reactions")
70
WHO hepatitis C treatment guidelines
EASL, Londres abril/2014 Teste anti-HCV para pessoas: populações alta prevalência exposição a riscos: Transfusão antes 1992 UDIV/N, tatuagem, piercing HIV + Nascidos entre Filhos mães hcv Presidiários/ex-pres Captação RR 2.9 Detecção RR 1.7 PCR imediato nos anti-HCV+ Topics for WHO hepatitis C screening, care and treatment guidelines Screening Care Treatment When to start treatment ? What medicines to use ? Who should be tested ? When to confirm(PCR) ? Awareness Diagnosis Referral Disease-stage assessment Treatment Monitoring How to assess degree of fibrosis ? What intervention to slow progression ? How monitor response ? and drug reactions ?
 Awareness. Diagnosis. Referral. Disease-stage. assessment. Treatment. Monitoring. How to assess degree of fibrosis What intervention to slow progression How monitor response and drug reactions")
71
são nascidos no período
Nos EUA, existem milhões de portadores do VHC Estima-se que 45% - 85% não foram sequer diagnosticados 75% dos infectados são nascidos no período Center for Disease Control and Prevention Morbity and Mortality Weekly Report/ Vol 61/ No. 4/ August 2012

72
WHO hepatitis C treatment guidelines
EASL, Londres abril/2014 APRI AST/lsn X 100/no plaquetas FIB-4 idade x AST / plaq x √ALT Avaliação do grau de fibrose: BH em larga escala = impraticável Elastografia ou Fibroteste = caros cenários carentes = APRI ou FIB4 Lentificar progressão: avaliação ingesta álcool tratamento redução da ingesta APRI Cut off 0.5 = 82% sens excl F2-4 Cut off 1.0 = 76%sens conf F4 Cut off 2.0 = 94% espec conf F4 ELASTOGRAFIA Cut off 7kPA = 79% sens exc F2-4 Cutt off 14 kPA = 91%espec com F4 Topics for WHO hepatitis C screening, care and treatment guidelines Screening Care Treatment When to start treatment ? What medicines to use ? Who should be tested ? When to confirm(PCR) ? Awareness Diagnosis Referral Disease-stage assessment Treatment Monitoring How to assess degree of fibrosis ? What intervention to slow progression ? How monitor response ? and drug reactions ?
 Awareness. Diagnosis. Referral. Disease-stage. assessment. Treatment. Monitoring. How to assess degree of fibrosis What intervention to slow progression How monitor response and drug reactions")
73
WHO hepatitis C treatment guidelines
EASL, Londres abril/2014 Topics for WHO hepatitis C screening, care and treatment guidelines Screening Care Treatment Quem tratar? Quando? TODOS adultos e crianças, naives e experimentados, mono ou coinfectados, incl UDIV ativo PRIORIDADE para F3 e F4 Como tratar ? PegIFN e não IFN convencional PR + TELA/BOCE gen 1 e não PR SOF + RBV c/s PEG gen 1,2,3 e 4 SIME + PR gen 1b e 1a s/Q80K When to start treatment ? What medicines to use ? Who should be tested ? When to confirm(PCR) ? Awareness Diagnosis Referral Disease-stage assessment Treatment Monitoring How to assess degree of fibrosis ? What intervention to slow progression ? How monitor response ? and drug reactions ?
 Awareness. Diagnosis. Referral. Disease-stage. assessment. Treatment. Monitoring. How to assess degree of fibrosis What intervention to slow progression How monitor response and drug reactions")
75
Tratamento é JUSTIFICADO em pacientes com fibrose moderada (F2)
TODOS os pacientes naives ou experimentados devem ser considerados para tratamento Tratamento deve ser PRIORIZADO para os pacientes com fibrose avançada (F3 e F4) Tratamento é JUSTIFICADO em pacientes com fibrose moderada (F2) Em pacientes com fibrose leve ou ausente (F0 e F1) a indicação e o momento de tratamento É DISCUTÍVEL
 Tratamento é JUSTIFICADO em pacientes com fibrose moderada (F2) Em pacientes com fibrose leve ou ausente (F0 e F1) a indicação e o momento de tratamento É DISCUTÍVEL.")
76
Em contextos onde nenhuma das novas opções estiver disponível, a terapia tríplice com PR + Boceprevir/Telaprevir permanece aceitável (genótipo 1) Em contextos onde nenhuma das novas opções estiver disponível, a combinação de PegIFN + Ribavirina permanece aceitável (genótipo 2-6)
")
77
NOVAS DROGAS DAA APROVADAS
Sofosbuvir Análogo Nucleotídeo 400 mg qd Todos Genótipos Alta barreira Simeprevir Inibidor De Protease 150 mg qd Genótipos 1 e 4 Baixa barreira Daclatasvir Inibidor NS5A 60 mg qd Todos Genótipos Baixa barreira

78
Guideline europeu - EASL 2014
PEG+RBV+SOF s PEG+RBV+SMV s (G1b e G1a s/Q80K) PEG+RBV+DCV s (apenas G1b) SOF+RBV s SOF+SMV (~c/RBV) s SOF+DCV (~c/RBV) s SOF+RBV s SOF+RBV+PEG 12s PEG+RBV+SOF s SOF+RBV s SOF+DCV(~c/RBV) s EASL 2014 78
 PEG+RBV+DCV 24s. (apenas G1b) SOF+RBV 24s. SOF+SMV (~c/RBV) 12s. SOF+DCV (~c/RBV) 12-24s. SOF+RBV 12s. SOF+RBV+PEG 12s. PEG+RBV+SOF 12s. SOF+RBV 24s. SOF+DCV(~c/RBV) 12-24s. EASL")
79
No Brasil onde estamos? Do que dispomos?

80
NOVOS REGIMES TRIPLOS / QUÁDRUPLOS
FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS Faldaprevir Asunaprevir (IP) MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) GS8558 (NS5A) Daclatasvir + Asunaprevir GS G59451 PR + Boceprevir ou Telaprevir Genótipo 1 PR + Simeprevir(IP) Genótipo 1 REGIMES COM PEGIFN PR + Sofosbuvir(NUC) Genótipos 1,4,5,6 2013 2014 2015 2016 2017 FASE III NOVOS REGIMES TRIPLOS / QUÁDRUPLOS ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV Faldaprevir (IP) + BI (NNuc) + RBV Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV GS5885(NS5A) + Sofosbuvir(Nuc) + RBV GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV Asunaprevir (IP) + Daclatasvir (NS5A) + BMS791325 RBV + Sofosbuvir(NUC) Genótipo 2 e 3 REGIMES SEM PEGIFN Thomas Berg, EASL 2013
 MK5172 (IP) MK7009 (IP) Daclatasvir (NS5A) GS8558 (NS5A) Daclatasvir + Asunaprevir. GS G PR. + Boceprevir. ou. Telaprevir. Genótipo 1. PR + Simeprevir(IP) Genótipo 1. REGIMES COM PEGIFN. PR + Sofosbuvir(NUC) Genótipos 1,4,5, FASE III. NOVOS REGIMES TRIPLOS / QUÁDRUPLOS. ABT450/R(IP/r) + ABT267(NS5A) + ABT333(NNuc) + RBV. Faldaprevir (IP) + BI (NNuc) + RBV. Daclatasvir (NS5A) + Sofosbuvir(Nuc) + RBV. GS5885(NS5A) + Sofosbuvir(Nuc) + RBV. GS9669 (NNuc) + Sofosbuvir(Nuc) + RBV. Asunaprevir (IP) + Daclatasvir (NS5A) + BMS RBV + Sofosbuvir(NUC) Genótipo 2 e 3. REGIMES SEM PEGIFN. Thomas Berg, EASL")
81
NOVAS DROGAS - NOVAS ESTRATÉGIAS
HEPATITE CRÔNICA C NOVAS DROGAS - NOVAS ESTRATÉGIAS 2014 CONCLUSÕES Vários novos regimes terapêuticos estarão disponíveis nos próximos meses (?) ou anos (quantos ?) Taxas de RVS muito elevadas (90% - 100%) serão obtidas Melhor tolerados e de mais simples administração, alguns todo via oral A duração dos tratamentos será menor (12 a 24 semanas) Grande parte dos indivíduos portadores vivem em áreas onde o trinômio screening / acesso / financiamento ainda não está disponível de forma adequada IFN, interferon; pegIFN, peginterferon; RBV, ribavirin. So what are the key elements of an ideal HCV regimen? First it should be of course highly effective, with high efficacy in traditionally challenging populations, including those patients with limited interferon sensitivity and those patients with advanced liver disease, such as cirrhotics. It should be easily administered: Once daily, with a low pill burden, would be ideal. An all-oral regimen, in which peginterferon/ribavirin have been replaced by an oral backbone with a minimal development of resistance. Pan-genotypic regimens, one that can be used not across not just genotype 1, 2 and 3, but even other genotypes such as 4, 5, and 6. It should be simple: short duration, with simple and straightforward stopping rules. And it should be of course safe and tolerable, with few or easily manageable adverse events. Jean-Michel Pawlotsky, F1000 Biology Reports 2012,4:5 81
 ou anos (quantos ) Taxas de RVS muito elevadas (90% - 100%) serão obtidas. Melhor tolerados e de mais simples administração, alguns todo via oral. A duração dos tratamentos será menor (12 a 24 semanas) Grande parte dos indivíduos portadores vivem em áreas onde o trinômio screening / acesso / financiamento ainda não está disponível de forma adequada. IFN, interferon; pegIFN, peginterferon; RBV, ribavirin. So what are the key elements of an ideal HCV regimen First it should be of course highly effective, with high efficacy in traditionally challenging populations, including those patients with limited interferon sensitivity and those patients with advanced liver disease, such as cirrhotics. It should be easily administered: Once daily, with a low pill burden, would be ideal. An all-oral regimen, in which peginterferon/ribavirin have been replaced by an oral backbone with a minimal development of resistance. Pan-genotypic regimens, one that can be used not across not just genotype 1, 2 and 3, but even other genotypes such as 4, 5, and 6. It should be simple: short duration, with simple and straightforward stopping rules. And it should be of course safe and tolerable, with few or easily manageable adverse events. Jean-Michel Pawlotsky, F1000 Biology Reports 2012,4:")
Apresentações semelhantes
 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")








. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")









