Carregar apresentação
A apresentação está carregando. Por favor, espere

1
O Estado da Arte da “Broncoscopia” na Pneumologia Atual
Mauro Zamboni, MD, FCCP, MSc Pneumologista, Coordenador do Grupo de Oncologia Torácica do INCA/MS Professor Associado – Curso de Especialização em Pneumologia – PUC-RJ

2
História da Broncoscopia
. Gustav Killian (1897) . Broncoscopia rígida . Chevalier Jackson (1904) . Fonte de luz/aspiração . Shigeto Ikeda (1966) . Broncofibroscópio
 . Broncoscopia rígida. . Chevalier Jackson (1904) . Fonte de luz/aspiração. . Shigeto Ikeda (1966) . Broncofibroscópio.")
3
Além da Broncoscopia

4
Pneumologia Intervencionista
Pleura e espaço pleural e vasos US Torácico em terapia intensiva: vasos e transtorácico Pleuroscopia – toracoscópio rígido ou pleuroscópio semi-flexível Cateter pleural Broncoscopia (diagnóstica e terapêutica) Ecobroncoscopia (EBUS) TBNA - Wang Autofluorescência Eletronavegação Eletrocirurgia endobrônquica e Plasma de Argônio Crioterapia Laser Termoplastia Vias Aéreas Traqueostomia Percutânea Órteses Balão e cateteres pleurais Estenoses laringo-traqueais Traqueomalacia e colapso dinâmico das vias aéreas Válvulas Endobrônquicas
 Ecobroncoscopia (EBUS) TBNA - Wang. Autofluorescência. Eletronavegação. Eletrocirurgia endobrônquica e Plasma de Argônio. Crioterapia. Laser. Termoplastia. Vias Aéreas. Traqueostomia Percutânea. Órteses. Balão e cateteres pleurais. Estenoses laringo-traqueais. Traqueomalacia e colapso dinâmico das vias aéreas. Válvulas Endobrônquicas.")
5
Pneumologia Intervencionista
Diagnóstico broncoscópico avançado Lesões pulmonares periféricas Adenopatia hilar e mediastinal Detecção precoce do câncer do pulmão Obstrução da Via Aérea Central Broncoscopia rígida, balão, órteses, laser, crioterapia, eletrocautério Outras Termoplastia brônquica Válvulas Endobrônquicas

6
Ultrassonografia da Pleura e do Espaço Pleural

7
Ultrassom Torácico em Terapia Intensiva
Transtorácico Curvilíneo Vaso linear

8
Derrame Pleural . Linha pleural superficialmente, pleura visceral + profundamente . O limite inferior se move sinusoidalmente de baixo para cima, em sincronismo com a respiração - específico do derrame pleural

9
. Consolidação Alveolar :
Opacidades hiperecóicas puntiformes – broncogramas aéreos

10
Vascular Trombo na VJID Agulha, fio guia e cateter

11
Por que US? Revisão de 342 toracenteses 18% PTx sem US 3% PTx com US
(Raplopoulos, AJR 156: 917) 18% PTx sem US 3% PTx com US UTI/pats ventilados (Kohan ARRD 1986) Modifica o tratamento em 41%
 18% PTx sem US. 3% PTx com US. UTI/pats ventilados. (Kohan ARRD 1986) Modifica o tratamento em 41%")
12
Vasos VCI (distensibilidade – avalia hidratação) Ecocardiografia
Guia para punção venosa central . Posição e trombo

13
Uso do cateter pleural The Pleurx® catheter: tratamento do derrame pleural maligno crônico em regime ambulatorial

14
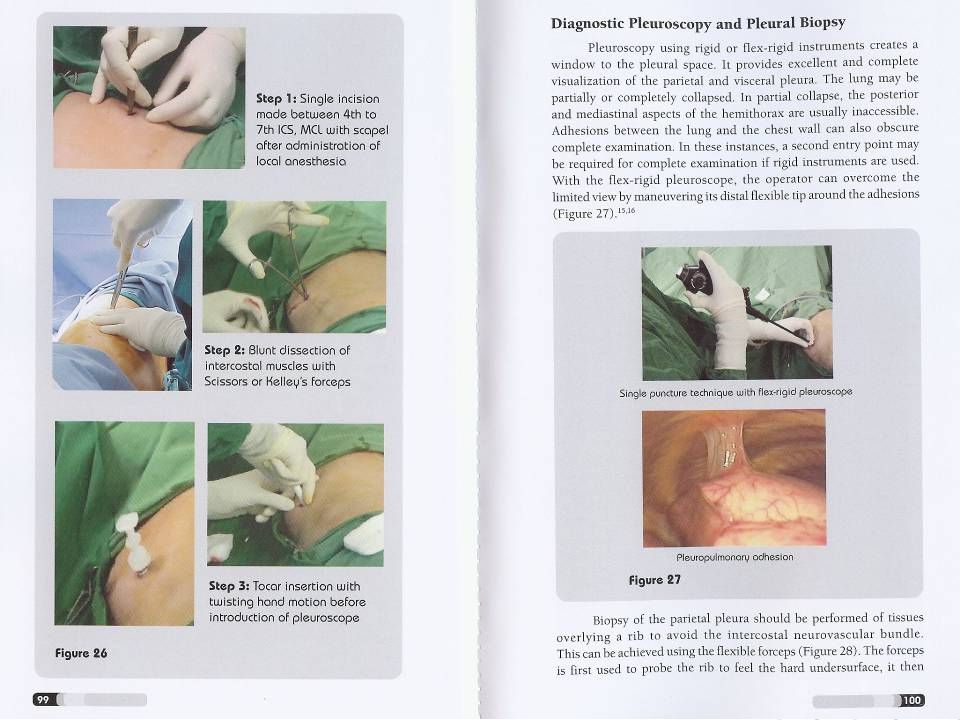
Pleuroscopia – toracoscopia rígida ou pleuroscópio semi-flexível
Toracoscópio Rígido – sala cirurgia Pleuroscópio Semi-Flexível: pode ser realizado na sala de broncoscopia sob sedação cosnciente

20
Wahidi, M. M. et al. Chest 2007;131:261-274
Nódulo em pleura diafragmática em paciente com derrame pleural Wahidi, M. M. et al. Chest 2007;131:

21
Diagnóstica e terapêutica
Broncoscopia Diagnóstica e terapêutica

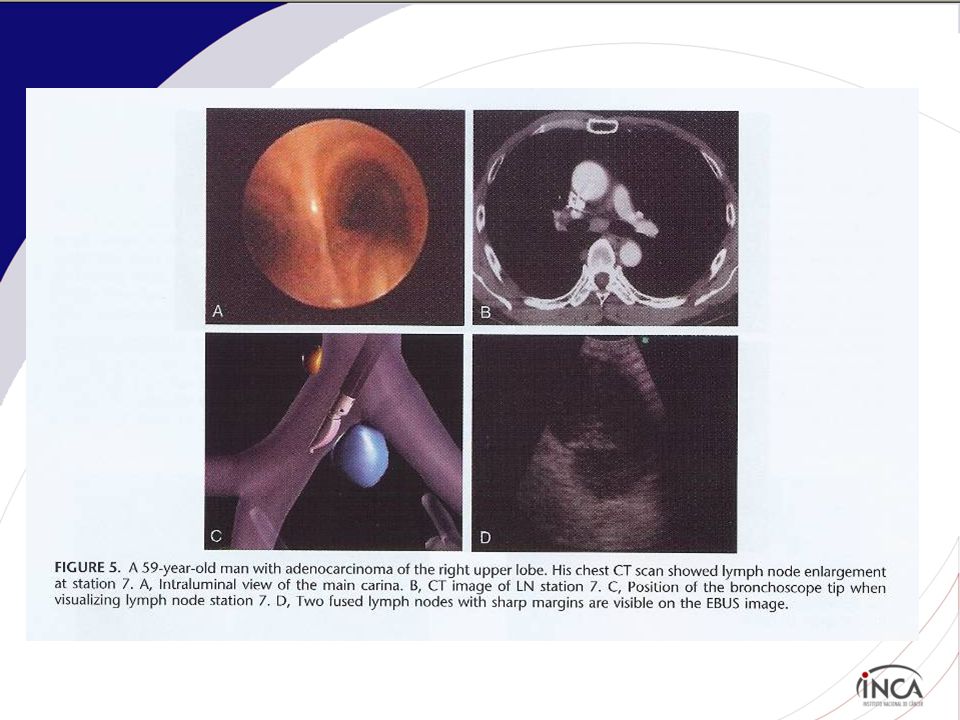
22
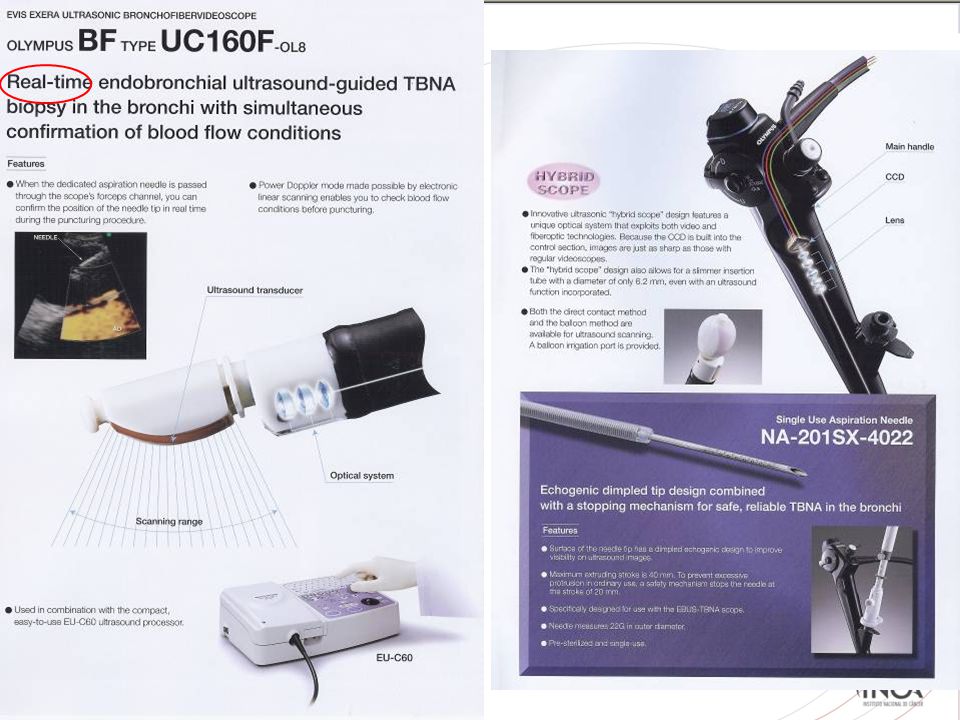
Ultrasom endobrônquico (EBUS)
")
24
Probe convexo Sheath Scope Saline filled balloon Convex US Probe
Needle (21or 22 Gauge) Sheath Saline filled balloon Convex US Probe Scope
 Sheath. Saline filled balloon. Convex US Probe. Scope.")
26
Needle Lymph node Vessel

27
Radial probe

30
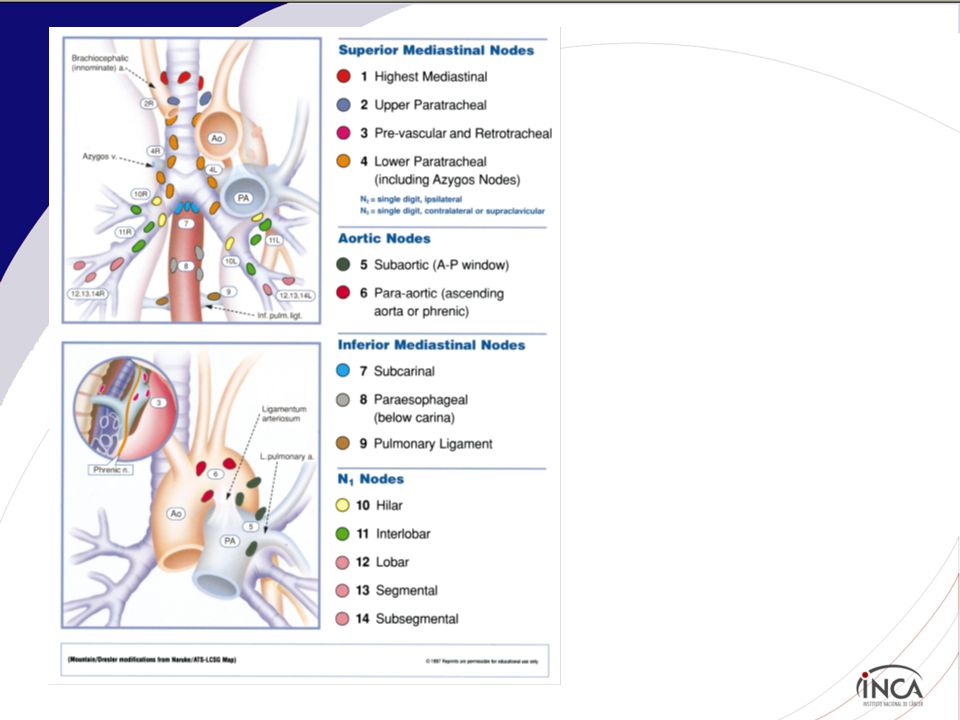
Áreas acessíveis pela técnica
2 3 4 5 6 7 8 9 TBNA ● EUS/FNA Mediastinoscopy Thoracoscopy

31
EBUS versus mediastinoscopia
. Pts. CNPCP que necessitavam de mediastinoscopia . Todos pts foram submetidos ao EBUS seguido pela mediastinoscopia . N= 190 patients . Resultados: . 91% concordância . Especificidade e VPP 100% . Sensibilidade, VPN e acurácia EBUS 81%, 91%, 93% respectivamente Mediastinoscopia 79%, 90%, 93% respectivamente Yasufuku K, et al. J. Thorac Cadiovasc Surg;142:

32
Autofluorescência

33
Broncoscopia com autofluorescência

37
Paciente com pequeno carcinoma in situ endobrônquico
Wahidi, M. M. et al. Chest 2007;131:

38
Local indications for autofluorescence bronchoscopy examination (QMH)
Sputum cytology atypia but normal white light bronchoscopy and non-localizing radiological examination i.e. normal CXR/CT Operable lung cancer patients but synchronous lung cancer suspected. Preoperative assessment of lung cancer to delineate endobronchial extension.

39
Follow up plan for patients who had autofluorescence bronchoscopy performed (QMH)
For patients confirmed to have invasive lung cancer, they will be staged and managed according to the current recommendations. For patients with intraepithelial neoplasm, i.e. severe dysplasia or carcinoma in situ, local treatment will be offered (e.g. cryotherapy) unless refused by patients. For patients with moderate dysplasia, they would be followed up with autofluorescence bronchoscopy at 6 monthly interval till histology reported as mild dysplasia or less For remaining patients who had non-diagnostic autofluorescence bronchoscopy, they should have CT thorax if not done yet to look for peripheral lesions. If still non-diagnostic, these patients should be followed up regularly at referring unit and repeat sputum cytology at 6 monthly intervals. They should be referred for repeating autofluorescence bronchoscopy examination if sputum atypia persisted.
 unless refused by patients. For patients with moderate dysplasia, they would be followed up with autofluorescence bronchoscopy at 6 monthly interval till histology reported as mild dysplasia or less. For remaining patients who had non-diagnostic autofluorescence bronchoscopy, they should have CT thorax if not done yet to look for peripheral lesions. If still non-diagnostic, these patients should be followed up regularly at referring unit and repeat sputum cytology at 6 monthly intervals. They should be referred for repeating autofluorescence bronchoscopy examination if sputum atypia persisted.")
40
Navegação Eletromagnética

41
Wahidi, M. M. et al. Chest 2007;131:261-274

42
Navegação Eletromagnética

43
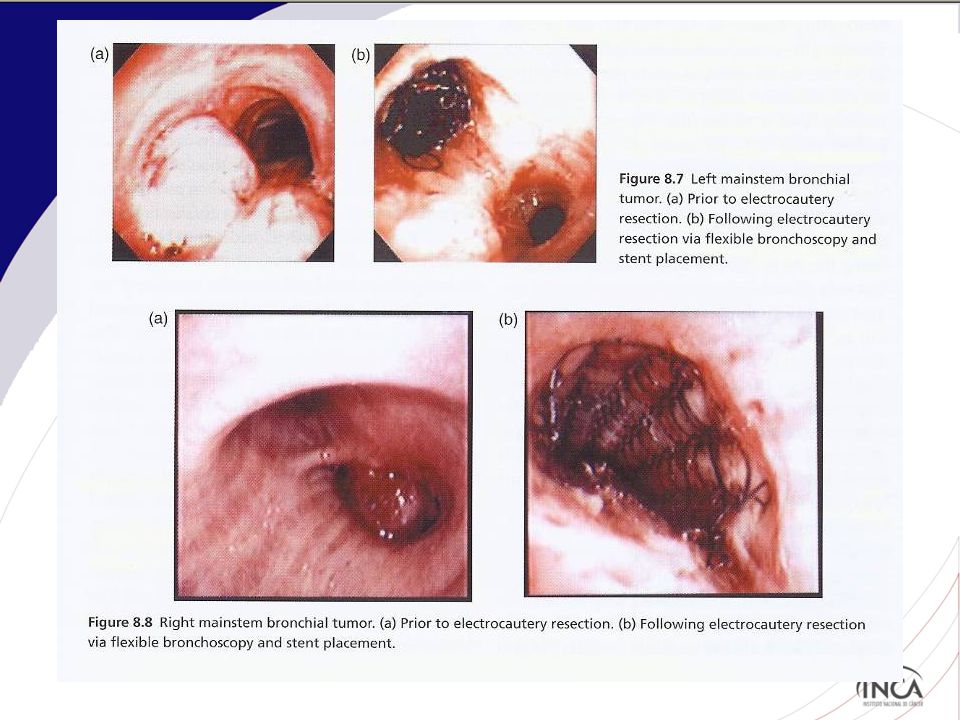
. Coagulação com Plasma de Argônio
Eletrocirurgia Eletrocautério com: . Coagulação com Plasma de Argônio . Nd:YAG Laser . Crioterapia

44
Eletrocautério

46
Coagulação com Plasma de Argônio
A high voltage spark is delivered at the tip of the probe, which ionizes the argon gas as it is sprayed from the probe tip in the direction of the target tissue. via the flexible or rigid bronchoscope Non-contact

47
Tecido de granulação visível na extremidade distal de stent traqueal
Wahidi, M. M. et al. Chest 2007;131:

48
Nd:YAG laser via bronco flexível ou rígido Sem contato com tecido
Baixa absorção Alta coagulação Pequeno efeito de corte Perfuração, fogo em via aérea e embolismo gasoso

49
An example of Nd-YAG laser treatment of a benign tumor (fibrolipoma) in the right lower lobe bronchus. An example of Nd-YAG laser treatment of a benign tumor (fibrolipoma) in the right lower lobe bronchus. Left, A, tumor occluding the right lower bronchus; right middle lobe bronchus (RML) is open. Right, B, the star indicates laser burns where the stalk of the tumor was located. The lower lobe bronchi (RB 6–10) are now visible. Prakash U B S Chest 1999;116: ©1999 by American College of Chest Physicians
 in the right lower lobe bronchus. Left, A, tumor occluding the right lower bronchus; right middle lobe bronchus (RML) is open. Right, B, the star indicates laser burns where the stalk of the tumor was located. The lower lobe bronchi (RB 6–10) are now visible. Prakash U B S Chest 1999;116: ©1999 by American College of Chest Physicians.")
50
Crioterapia contato tecidual via broncoscópio rígido ou flexível
Seguro – sem risco para perfuração da parede brônquica Resultados mais demorados e necessita de várias broncoscopias para tratamento e remoção de debris. (A) Cryotherapy can be applied to tissue using either the probe tip or side. (B) Reapplication to the same area after thawing allows a deeper freeze and tissue destruction.
 Cryotherapy can be applied to tissue using either the probe tip or side. (B) Reapplication to the same area after thawing allows a deeper freeze and tissue destruction.")
51
Chest. 2007;131:

52
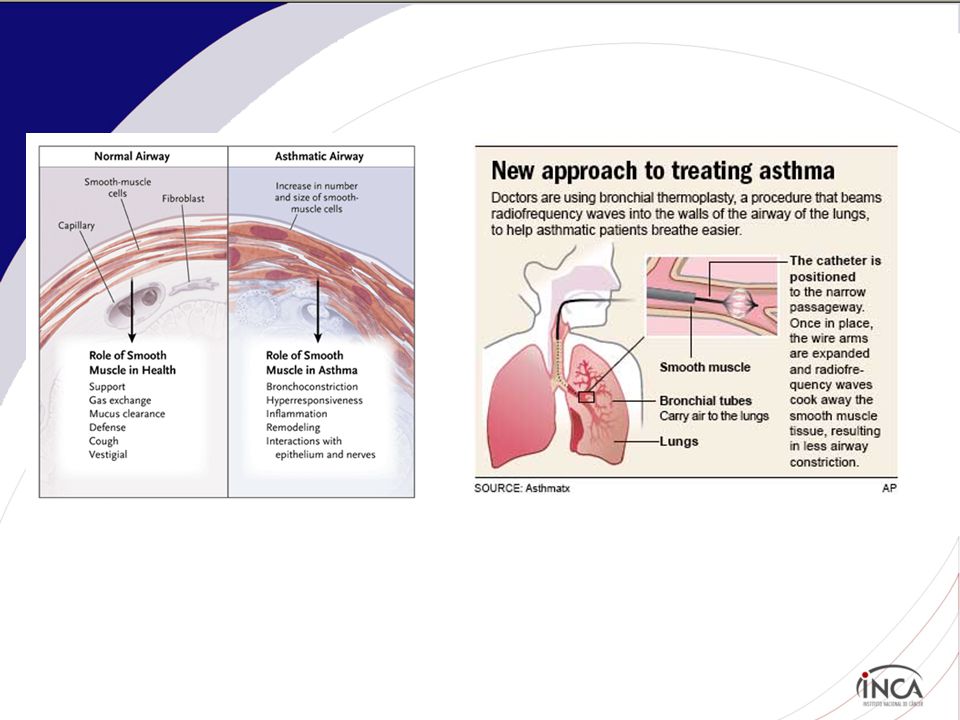
Termoplastia Brônquica

53
Termoplastia brônquica para Asma severa
Bronchial thermoplasty is a procedure in which controlled thermal energy is applied to the airway wall to decrease smooth muscle. Requires a series of procedures (3)
")
55
The Asthma Intervention Research (AIR) Trial
Cox G et al. NEJM 2007; 356:

56
AIR2 Trial Pts com asma severa 280 pts até 31 Março 2007

57
Resumo Bronchial thermoplasty to moderate to severe asthma
55 BT vs 54 control The mean rate of mild exacerbations, as compared with baseline, was reduced in the bronchial-thermoplasty group but was unchanged in the control group (change in frequency per subject per week, –0.16±0.37 vs. 0.04±0.29; P=0.005). At 12 months, there were significantly greater improvements in the bronchial-thermoplasty group than in the control group in the morning peak expiratory flow (39.3±48.7 vs. 8.5±44.2 liters per minute) scores on the AQLQ (1.3±1.0 vs. 0.6±1.1) ACQ (reduction, 1.2±1.0 vs. 0.5±1.0) the percentage of symptom-free days (40.6±39.7 vs. 17.0±37.9), and symptom scores (reduction, 1.9±2.1 vs. 0.7±2.5) while fewer puffs of rescue medication were required. Adverse events immediately after treatment were more common in the bronchial-thermoplasty group than in the control group but were similar during the period from 6 weeks to 12 months after treatment.
. At 12 months, there were significantly greater improvements in the bronchial-thermoplasty group than in the control group in the. morning peak expiratory flow (39.3±48.7 vs. 8.5±44.2 liters per minute) scores on the AQLQ (1.3±1.0 vs. 0.6±1.1) ACQ (reduction, 1.2±1.0 vs. 0.5±1.0) the percentage of symptom-free days (40.6±39.7 vs. 17.0±37.9), and. symptom scores (reduction, 1.9±2.1 vs. 0.7±2.5) while fewer puffs of rescue medication were required. Adverse events immediately after treatment were more common in the bronchial-thermoplasty group than in the control group but were similar during the period from 6 weeks to 12 months after treatment.")
58
Vias Aéreas

59
Órteses Silicone Metálicos Mais barato Facilmente removidos
Alto índice de migração Necessita broncoscopia rígida Metálicos Podem ser colocados através da broncofibroscopia ou da broncoscopia rígida com ou sem o auxílio da fluoroscopia Ultraflex® stent

60
Stent de silicone no BPD Wahidi, M. M. et al. Chest 2007;131:261-274

61
Wahidi, M. M. et al. Chest 2007;131:261-274

62
Stent Type Manufacturer Construction Dumon Novatech Molded silicon rubber Hood Hood Corp. Wallstent Boston Scientific Woven cobalt/chrome alloy monofilament coated with silicone Polyflex Rush Inc. Polyester mesh covered with silicone Ultraflex Single strand woven nitilol With/without silicone coating Dynamic Silicone with anterolateal steel struts

63
Stent de nitinol no BPD A nitinol stent in place in the right mainstem bronchus. Left, A, view through the stent. Right, B, a view of the distal end of the stent and distal bronchus. Prakash U B S Chest 1999;116: ©1999 by American College of Chest Physicians

64
Metal Stent Silicone Stents

65
Madden B. P. et al.; Ann Thorac Surg 2002;73:938-944
Both covered and uncovered Ultraflex expandable metallic bronchial stents and a covered tracheal stent Madden B. P. et al.; Ann Thorac Surg 2002;73: Copyright ©2002 The Society of Thoracic Surgeons

66
Redução do Volume Pulmonar por Broncoscopia
Placement of one-way endobronchial valves in segmental and/or sub-segmental airways General inclusion and exclusion criteria (extrapolated from NETT) Inclusion: severe, UL emphysema Exclusion: diffuse emphysema, FEV1<20%, DLCO<20%
 Inclusion: severe, UL emphysema. Exclusion: diffuse emphysema, FEV1<20%, DLCO<20%")
67
Válvulas Endobrônquicas
Emphasys Med Inc: Emphasys Zephyr™ Endobronchial Valve* (EBV):válvula unidirecional de silicone em suporte de nitinol Endobronchial Valve for Emphysema PalliatioN Trial (VENT) Spiration Inc: IBV valve IBV Valve Trial An older model
:válvula unidirecional de silicone em suporte de nitinol. Endobronchial Valve for Emphysema PalliatioN Trial (VENT) Spiration Inc: IBV valve. IBV Valve Trial. An older model.")
68
Válvula Endobrônquica para o Tratamento do Enfisema (VENT)
. 31 centros . N= 321 .Critérios para inclusão . Idade 40 a 75 . Dx de enfisema heterogeneo FEV1 de 15 a 45% do previsto CPT > 100% do previsto VR > 150% do previsto Sciurba FC, et al. N Engl J Med 2010;363:

69
View of endobronchial one-way valves placed into the airways of a patient with heterogeneous emphysema. Wahidi M M et al. Chest 2007;131: ©2007 by American College of Chest Physicians

70
VENT Trial Primary and Secondary Efficacy Outcomes in the Intention-to-Treat Population (Change from Baseline at 6 Months) Table 2 Primary and Secondary Efficacy Outcomes in the Intention-to-Treat Population (Change from Baseline at 6 Months). Sciurba FC et al. N Engl J Med 2010;363:
. Sciurba FC et al. N Engl J Med 2010;363:")
71
Balão para broncoplastia
Pode ser utilizado através do broncoscópio rígido ou flexível Dilatação com ogiva somente com BR Mayse, M. L. et al. Chest 2004;126:

72
Microdebrider

73
EBUS com mini Probe Radial
Lung nodule Lung Nodule Lung Nodule Miniature US probe

74
EBUS com Probe Radial para Bx de lesões periféricas
. 24 pts com lesões periféricas pequenas Nenhuma com + de 30 mm de diâmetro Diâmetro mediano 18.4 mm . EBUS + fluoro utilizdos para localização das lesões . 19/24 visíveis pelo EBUS (79%) . BX TB e escovado . 14/19 com diagnóstico definido Eur Respir J 2004;24:533
 . BX TB e escovado. . 14/19 com diagnóstico definido. Eur Respir J 2004;24:533.")
Apresentações semelhantes








 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")











. Metallic bonding is essentially covalent bonding with delocalized electrons.>")

 SEGUNDO NOVOS ESTRATOS VITÓRIA, ES – OUTUBRO 2008 Kenneth Camargo – IMS/UERJ Cláudia Medina – IESC/UFRJ.>")


