Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Avaliação pré-operatória em Anestesiologia Pediátrica
Rodrigo Pereira Diaz Andre TSA/SBA

2
Ansiedade Pré-operatória
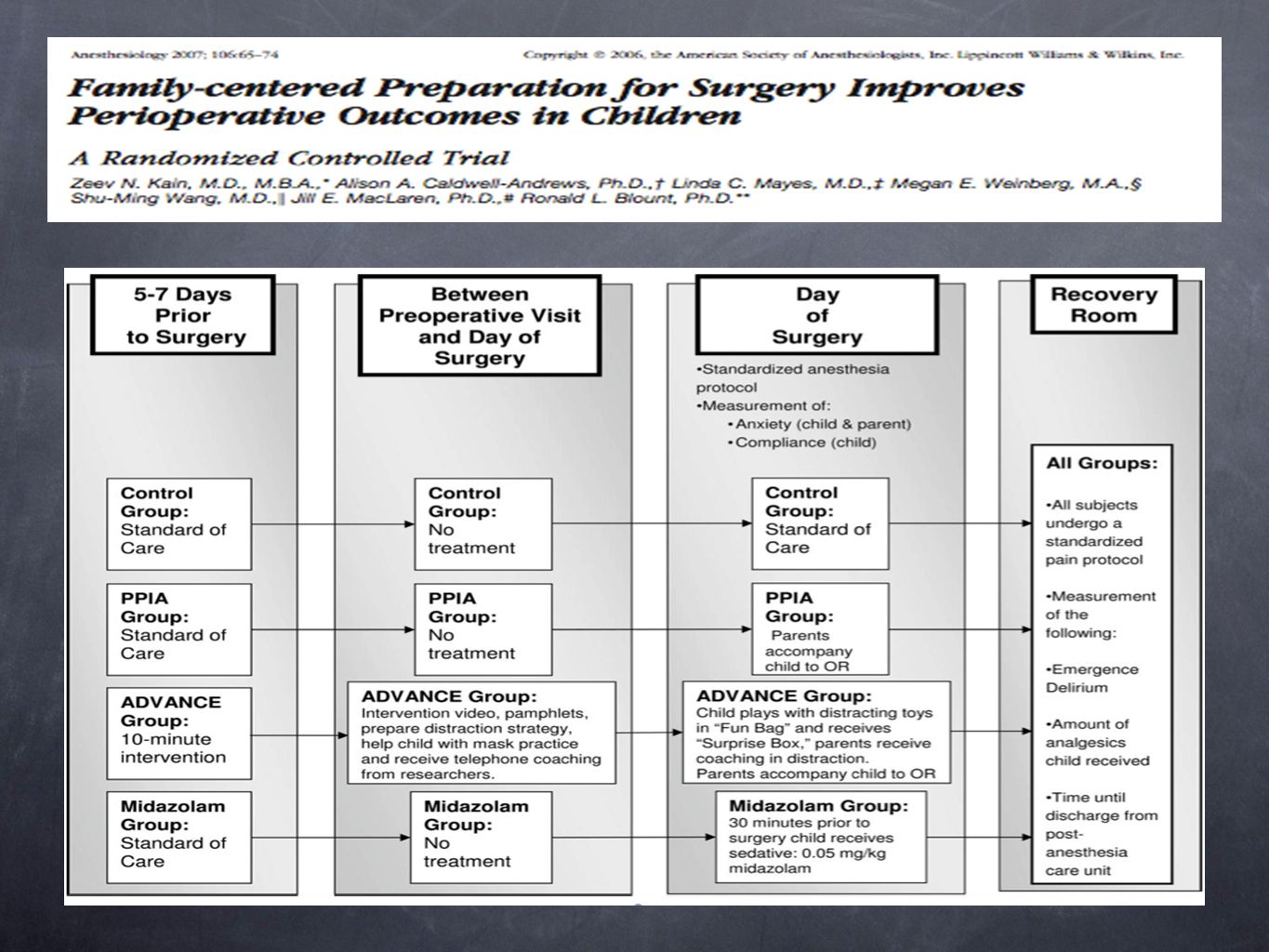
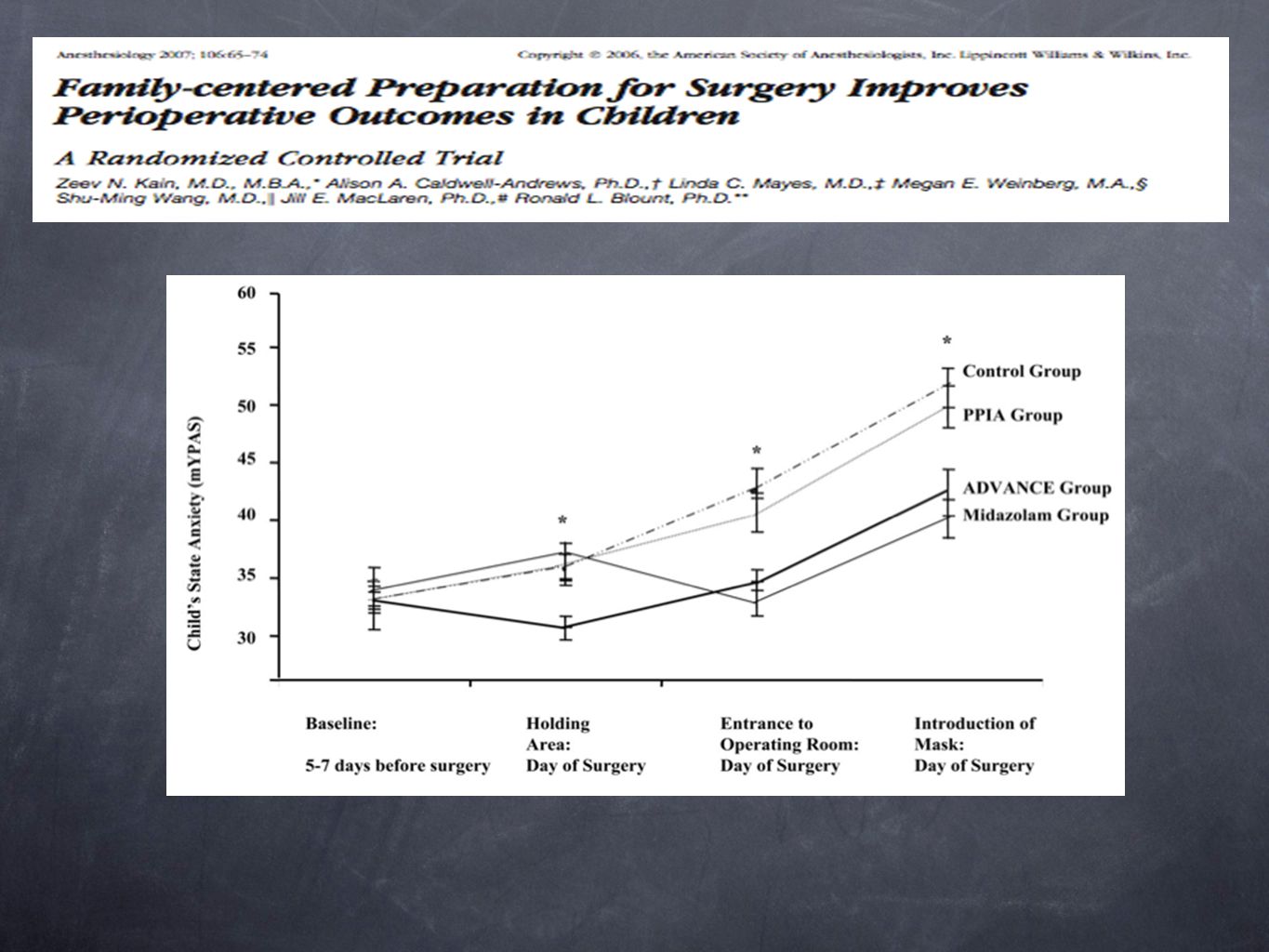
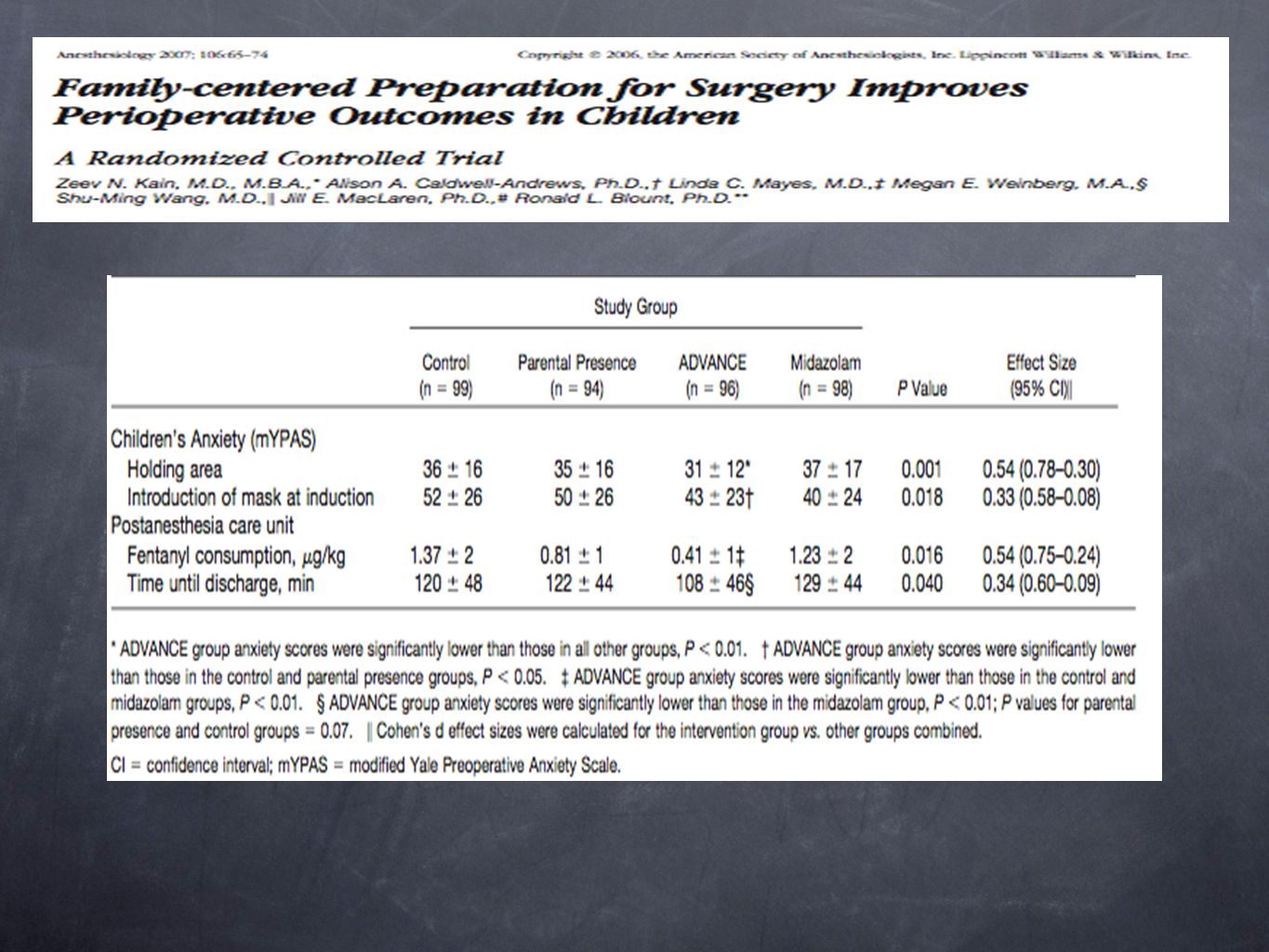
Questões do Desenvolvimento Ansiedade Pré-operatória Desenvolvimento Cognitivo/Compreensão da Doença Ligação Familiar: ➸ Ligação Segura Ligação Insegura Ligação Ansiosa Temperamento: Emotividade Atividade Sociabilidade Fatores de Risco: Idade e Maturidade Experiência Prévia Ansiedade Basal Características Familiares Intervenções Comportamentais: Programas de Preparação Pré-operatória: Revistas/Livros Vídeos Fantoches Musica ?? Presença dos Pais: Deve ser aplicada em todos os casos? Reduz ansiedade das crianças? Provoca ansiedade nos pais! Existe grande variabilidade de sua aplicação. $ Pode haver implicações legais! The perioperative period is stressful for many individuals undergoing surgery, and this is especially true for children. Children's stress during the perioperative period results from multiple sources, one of which is a limited understanding of their illness and the need for surgery. Early developmental theories (e.g., those of Piaget[1,][2]) suggest that a child's understanding of illness changes qualitatively as he or she matures cognitively. Although dated, Bibace and Walsh[3] described a model of the child's progressive understanding of illness that evolves from prelogical explanations such as phenomenism (e.g., magical thinking), to concrete-logical explanations such as contamination (e.g., eating bad food), to formal-logical explanations (e.g., physiologic causes). This is still currently the most widely cited model for the child's perspective of illness. Although less theoretically developed, children's understanding of the treatments for illnesses is thought to follow a similar developmental pattern. In terms of understanding of surgery, a child's concepts are particularly underdeveloped. Young children have difficulty defining “an operation” suggesting that it is the same as being sick, going for a doctor's checkup, or taking a napGiven these developmental considerations, it is not surprising that young children are more likely to have misconceptions about hospitalization and surgery than older children and adults[5] and are at unique and disparate risk for perioperative stress when compared with adults. Another child-specific consideration during the perioperative period is his or her attachment style to the parent/caregiver and how the parent-child relationship influences the child's response to the separation associated with surgery/anesthesia. Although adults also undergo separation from family, the separation of children from their parents is particularly stressful. Coping with separation is a lifelong challenge that is inevitable and necessary for a child's normal healthy development.[6] Separation experiences such as saying good-bye at the door of school or sleeping overnight at a friend's house facilitate normal childhood psychological growth and personality organization by mobilizing opportunities for learning and adaptation. Other separation experiences, especially those occurring in the context of loss, illness, or other stressors, can precipitate states of confusion, anger, and anxiety. Brief separations such as those associated with surgery are most stressful for infants, toddlers, and preschool-aged children. Indeed, for school-aged children, responses to separation may reflect, in part, response patterns established early in the preschool years. For children with biologically based vulnerabilities, such as a sensitivity to novelty and transitions, even expected separations, may impose a greater degree of stress than for less sensitive children.[6] Similarly, for children with developmental delay, separations may be experienced with a degree of anxiety and developmental stress more like that experienced by a younger child. Children may be “securely attached,” “insecurely attached,” or “anxiously attached” to their parents. Infants who are more “securely attached” to their parents deal more adaptively with the stress of brief separation and with the novelty of the hospital experience. These infants are more willing to explore their world and respond positively to their mother's return, using her as a secure, stable base from which to approach strangers and new situations.[8,][9] In contrast, toddlers classified as “anxiously attached” to their mother tend to be distressed in unfamiliar situations, like those found in the perioperative environment, even when their mother is present. When their mother returns after brief separations, these infants tend to be angry and distressed and avoid physical contact. Another form of “insecure attachment” is avoidance. Avoidant children do not explore their surroundings as much as securely attached infants do and tend to ignore their mother. They rarely show distress on separation and avoid interactions with their mother when she returns. Conversely, “insecurely attached” infants are more easily distressed by even brief separations and spend more time trying to stay close to their parents. More anxious about novelty and separation, they are less likely to explore and less likely to adapt positively to new situations. Responses to the stress of the perioperative period in infancy and preschool years reflects in part the child's relationships with the parents as well as the child's temperament. Temperament refers to emotional responses that are characteristic of individual infants and young children. Clusters of related characteristics may constitute a temperament type. While conceptually related to personality, temperament characteristics in children are presumed to have primarily a genetic basis.[10] Later personality characteristics, such as adulthood characteristics, presumably reflect the interaction between temperament traits arising in early childhood and environmental influences. Some authors find that it is useful to classify infants with respect to three main dimensions: emotionality, activity, and sociability.[11] Emotionality refers to the ease with which an infant becomes aroused or anxious, especially in situations that might lead to fear, such as perioperative settings. Activity refers to the infant's customary level of energy and intensity of behavior. Sociability reflects the infant's tendency to approach or avoid others. These behavioral dimensions of temperament are also reflected in physiologic responses related to anxiety.[12] For example, measures of heart rate variability are closely related to infants' reactivity and lability in the first year of life.[13] Infants with less variability in heart rate (presumably reflecting increased sympathetic relative to parasympathetic influence on heart rate) are more labile and reactive to novelty. Infants who have a tendency to avoid novelty cry more easily and are less active in contrast to those who readily approach the unfamiliar. In long-term studies, infants who are inhibited in the face of novelty continue to be so through early school age.[14] Thus, temperament as a behavioral descriptor appears to characterize an enduring cluster of traits reflecting reactivity and anxiety regulation in the face of novelty. It is estimated that between 40% and 60% of children develop significant fear and anxiety before their surgery.[16] Furthermore, separation from parents and induction of anesthesia have been found to be the most stressful times during the surgical/anesthesia experience. Age and developmental maturity • Previous experience with medical procedures and illness • Individual capacity for affect regulation and trait anxiety (baseline anxiety) • Parental state (situational) and trait (baseline) anxiety Children between the ages of 1 and 5 years are at greatest risk for developing extreme anxiety and distress. This is not surprising, because separation anxiety often does not peak until 1 year of age, and children older than the age of 5 years can more easily cope with new and unpredictable situations. A history of prior stressful medical encounters, such as in the pediatrician's office, the dentist's office, with previous surgery, or with previous hospitalization, affects how a child reacts to new medical encounters. Children who are shy and inhibited, as identified by temperament tests, are also at increased risk for developing anxiety and distress before surgery. In addition, children who lack good social adaptive abilities are likewise at risk.[26] Parental characteristics also have a strong influence on a child's behavior during the perioperative experience. Children of parents who are more anxious, children of parents who use avoidance coping mechanisms, and children of separated or divorced parents all appear to be at high risk for developing preoperative anxiety. The gender of the parent (mothers are more anxious than fathers[28]), the child younger than 1 year of age, children with repeated hospital admissions, and baseline temperament of the child are predictors of increased parental preoperative anxiety. Once one identifies those children and parents who are at the greatest risk for developing preoperative anxiety and distress, one can then take steps to better treat this “at-risk” population. Kain ZN, Mayes LC, Weisman SJ, Hofstadter MB: Social adaptability, cognitive abilities, and other predictors for children's reactions to surgery. J Clin Anesth 2000; 12: Kain ZN, Mayes LC, Caramico LA: Preoperative preparation in children: a cross-sectional study. J Clin Anesthesia 1996; 8: Messeri A, Caprilli S, Busoni P: Anaesthesia induction in children: a psychological evaluation of the efficiency of parents' presence. Paediatr Anaesth 2004; 14:
 suggest that a child s understanding of illness changes qualitatively as he or she matures cognitively. Although dated, Bibace and Walsh[3] described a model of the child s progressive understanding of illness that evolves from prelogical explanations such as phenomenism (e.g., magical thinking), to concrete-logical explanations such as contamination (e.g., eating bad food), to formal-logical explanations (e.g., physiologic causes). This is still currently the most widely cited model for the child s perspective of illness. Although less theoretically developed, children s understanding of the treatments for illnesses is thought to follow a similar developmental pattern. In terms of understanding of surgery, a child s concepts are particularly underdeveloped. Young children have difficulty defining an operation suggesting that it is the same as being sick, going for a doctor s checkup, or taking a napGiven these developmental considerations, it is not surprising that young children are more likely to have misconceptions about hospitalization and surgery than older children and adults[5] and are at unique and disparate risk for perioperative stress when compared with adults. Another child-specific consideration during the perioperative period is his or her attachment style to the parent/caregiver and how the parent-child relationship influences the child s response to the separation associated with surgery/anesthesia. Although adults also undergo separation from family, the separation of children from their parents is particularly stressful. Coping with separation is a lifelong challenge that is inevitable and necessary for a child s normal healthy development.[6] Separation experiences such as saying good-bye at the door of school or sleeping overnight at a friend s house facilitate normal childhood psychological growth and personality organization by mobilizing opportunities for learning and adaptation. Other separation experiences, especially those occurring in the context of loss, illness, or other stressors, can precipitate states of confusion, anger, and anxiety. Brief separations such as those associated with surgery are most stressful for infants, toddlers, and preschool-aged children. Indeed, for school-aged children, responses to separation may reflect, in part, response patterns established early in the preschool years. For children with biologically based vulnerabilities, such as a sensitivity to novelty and transitions, even expected separations, may impose a greater degree of stress than for less sensitive children.[6] Similarly, for children with developmental delay, separations may be experienced with a degree of anxiety and developmental stress more like that experienced by a younger child. Children may be securely attached, insecurely attached, or anxiously attached to their parents. Infants who are more securely attached to their parents deal more adaptively with the stress of brief separation and with the novelty of the hospital experience. These infants are more willing to explore their world and respond positively to their mother s return, using her as a secure, stable base from which to approach strangers and new situations.[8,][9] In contrast, toddlers classified as anxiously attached to their mother tend to be distressed in unfamiliar situations, like those found in the perioperative environment, even when their mother is present. When their mother returns after brief separations, these infants tend to be angry and distressed and avoid physical contact. Another form of insecure attachment is avoidance. Avoidant children do not explore their surroundings as much as securely attached infants do and tend to ignore their mother. They rarely show distress on separation and avoid interactions with their mother when she returns. Conversely, insecurely attached infants are more easily distressed by even brief separations and spend more time trying to stay close to their parents. More anxious about novelty and separation, they are less likely to explore and less likely to adapt positively to new situations. Responses to the stress of the perioperative period in infancy and preschool years reflects in part the child s relationships with the parents as well as the child s temperament. Temperament refers to emotional responses that are characteristic of individual infants and young children. Clusters of related characteristics may constitute a temperament type. While conceptually related to personality, temperament characteristics in children are presumed to have primarily a genetic basis.[10] Later personality characteristics, such as adulthood characteristics, presumably reflect the interaction between temperament traits arising in early childhood and environmental influences. Some authors find that it is useful to classify infants with respect to three main dimensions: emotionality, activity, and sociability.[11] Emotionality refers to the ease with which an infant becomes aroused or anxious, especially in situations that might lead to fear, such as perioperative settings. Activity refers to the infant s customary level of energy and intensity of behavior. Sociability reflects the infant s tendency to approach or avoid others. These behavioral dimensions of temperament are also reflected in physiologic responses related to anxiety.[12] For example, measures of heart rate variability are closely related to infants reactivity and lability in the first year of life.[13] Infants with less variability in heart rate (presumably reflecting increased sympathetic relative to parasympathetic influence on heart rate) are more labile and reactive to novelty. Infants who have a tendency to avoid novelty cry more easily and are less active in contrast to those who readily approach the unfamiliar. In long-term studies, infants who are inhibited in the face of novelty continue to be so through early school age.[14] Thus, temperament as a behavioral descriptor appears to characterize an enduring cluster of traits reflecting reactivity and anxiety regulation in the face of novelty. It is estimated that between 40% and 60% of children develop significant fear and anxiety before their surgery.[16] Furthermore, separation from parents and induction of anesthesia have been found to be the most stressful times during the surgical/anesthesia experience. Age and developmental maturity. • Previous experience with medical procedures and illness. • Individual capacity for affect regulation and trait anxiety (baseline anxiety) • Parental state (situational) and trait (baseline) anxiety. Children between the ages of 1 and 5 years are at greatest risk for developing extreme anxiety and distress. This is not surprising, because separation anxiety often does not peak until 1 year of age, and children older than the age of 5 years can more easily cope with new and unpredictable situations. A history of prior stressful medical encounters, such as in the pediatrician s office, the dentist s office, with previous surgery, or with previous hospitalization, affects how a child reacts to new medical encounters. Children who are shy and inhibited, as identified by temperament tests, are also at increased risk for developing anxiety and distress before surgery. In addition, children who lack good social adaptive abilities are likewise at risk.[26] Parental characteristics also have a strong influence on a child s behavior during the perioperative experience. Children of parents who are more anxious, children of parents who use avoidance coping mechanisms, and children of separated or divorced parents all appear to be at high risk for developing preoperative anxiety. The gender of the parent (mothers are more anxious than fathers[28]), the child younger than 1 year of age, children with repeated hospital admissions, and baseline temperament of the child are predictors of increased parental preoperative anxiety. Once one identifies those children and parents who are at the greatest risk for developing preoperative anxiety and distress, one can then take steps to better treat this at-risk population. Kain ZN, Mayes LC, Weisman SJ, Hofstadter MB: Social adaptability, cognitive abilities, and other predictors for children s reactions to surgery. J Clin Anesth 2000; 12: Kain ZN, Mayes LC, Caramico LA: Preoperative preparation in children: a cross-sectional study. J Clin Anesthesia 1996; 8: Messeri A, Caprilli S, Busoni P: Anaesthesia induction in children: a psychological evaluation of the efficiency of parents presence. Paediatr Anaesth 2004; 14:")
3
Presença dos Pais Quais são os Fatos?
A maioria dos parentes e crianças preferem ficar juntos durante procedimentos. A maioria dos pais preferem presenciar a indução da anestesia. Incidência maior em pais cujos filhos são submetidos a procedimentos repetidos. A presença dos pais durante a indução não necessariamente equaciona os problemas. As mães que se mostram mais motivadas a presenciarem são também mais ansiosas, e seus filhos mais estressados no momento da indução. Mais de 90% dos pais referem algum grau de ansiedade. Henderson MA, Baines DB, Overton JH: Parental attitudes to presence at induction of paediatric anaesthesia. Anaesth Intensive Care 1993; 21: Ryder I, Spargo P: Parents in the anesthetic room: a questionnaire survey of parents' reactions. Anaesthesia 1991; 46: Kain ZN, Caldwell-Andrews AA, Wang SM, et al: Parental intervention choices for children undergoing repeated surgeries. Anesth Analg 2003; 96: Caldwell-Andrews AA, Kain ZN, Mayes LC, et al: Motivation and maternal presence during induction of anesthesia. Anesthesiology 2005; 103: Vessey JA, Bogetz MS, Caserza CL, et al: Parental upset associated with participation in induction of anaesthesia in children. Can J Anaesth 1994; 41: Kain ZN, Caldwell-Andrews AA, Mayes LC, et al: Parental presence during induction of anesthesia: physiological effects on parents. Anesthesiology 2003; 98:58-64

4
Presença dos Pais t is well established that most parents and children prefer to remain together during procedures such as immunization, bone marrow aspiration, and dental treatment.[49,][50] Several survey studies have also indicated that most parents prefer to be present during induction of anesthesia regardless of the child's age or previous surgical experience. It is important to note, however, that parental presence during induction of anesthesia (PPIA) does not necessarily equate with appropriate choice of interventions. One study found that mothers who were most highly motivated to be present at induction of anesthesia also reported high levels of anxiety and their children were more distressed at induction. That is, mothers who most want to be present during induction of anesthesia are the most anxious during induction and thus the anesthesiologist should consider carefully the option of permitting the very anxious mother to accompany her child to the operating room. Indeed, more than 90% of parents report some degree of anxiety during the anesthesia induction process. The most upsetting factors are seeing the child go limp during induction and then having to leave their child. This observation was confirmed by a study that examined heart rate, blood pressure, and skin conductance levels in mothers as they observed their child's induction of anesthesia.[56] The study found a moderate increase in heart rate and blood pressure among the mothers who were present during induction of anesthesia (Fig. 3-2). However, no cardiac arrhythmias or ischemic episodes were noted.
 does not necessarily equate with appropriate choice of interventions. One study found that mothers who were most highly motivated to be present at induction of anesthesia also reported high levels of anxiety and their children were more distressed at induction. That is, mothers who most want to be present during induction of anesthesia are the most anxious during induction and thus the anesthesiologist should consider carefully the option of permitting the very anxious mother to accompany her child to the operating room. Indeed, more than 90% of parents report some degree of anxiety during the anesthesia induction process. The most upsetting factors are seeing the child go limp during induction and then having to leave their child. This observation was confirmed by a study that examined heart rate, blood pressure, and skin conductance levels in mothers as they observed their child s induction of anesthesia.[56] The study found a moderate increase in heart rate and blood pressure among the mothers who were present during induction of anesthesia (Fig. 3-2). However, no cardiac arrhythmias or ischemic episodes were noted.")
5
Presença dos Pais Pais mais calmos podem ser benéficos?
Devemos individualizar? Existe beneficio real? Qual a aplicabilidade? Kain ZN, Ferris CA, Mayes LC, Rimar S: Parental presence during induction of anaesthesia: practice differences between the United States and Great Britain. Paediatr Anaesth 1996; 6:

6
Presença dos Pais

7
Presença dos Pais Desvantagens: Vantagens:
Minimizar necessidade de medicação pré-anestésica. Melhora estética na separação dos pais. Melhora da ansiedade durante a indução anestésica? Redução dos efeitos comportamentais de longo prazo? Estudos iniciais demonstravam redução na ansiedade e melhora na cooperação. Estudos futuros indicaram que a presença rotineira dos pais não era benéfica! Quebra da rotina da equipe. Comprometimento com o ambiente estéril. Salas de cirurgias cheias. Possível reação adversa dos parentes. Aumento na ansiedade da criança. Indução prolongada. Estresse adicional ao anestesiologista. Algumas crianças ficam mais ansiosas com a presença dos pais. Alguns parentes podem apresentar comportamento bizarro! Levar em consideração idade e nível de ansiedade das crianças e familiares. Atentar para repercussões legais! Hannallah RS, Rosales JK:Experience with parents' presence during anaesthesia induction in children. Can Anaesth Soc J 1983; 30: Schulman JL, Foley JM, Vernon DT, Allan D A study of the effect of the mother's presence during anesthesia induction. Pediatrics 1967; 39: Bevan JC, Johnston C, Haig MJ, et al:Preoperative parental anxiety predicts behavioral and emotional responses to induction of anesthesia in children. effective?. Anesthesiology 1998; 89: Kain ZN, Mayes LC, Wang SM, et al: Parental presence during induction of anesthesia versus sedative premedication: which intervention is more effective?. Anesthesiology 1998; 89: Shaw EG, Routh DK: Effect of mother presence on children's reaction to aversive procedures. J Pediatr Psychol 1982; 7:33-42 Bowie JR: Parents in the operating room. Anesthesiology 1993; 78: Schofield NM, White JB: Interrelations among children, parents, premedication, and anaesthetists in paediatric day stay surgery. BMJ 1989; 299: Gauderer MW, Lorig JL, Eastwood DW: Is there a place for parents in the operating room?. J Pediatr Surg 1989; 24:

8
Presença dos Pais Quando Indicar? Atenção!
Crianças maiores que 4 anos. Crianças com temperamento calmo. Pais calmos. Crianças calmas com pais ansiosos se comportam pior do que se estivessem sem os pais! Presença dos pais sem o preparo adequado pode ser contra produtivo! Repercussões Legais!! Kain ZN, Mayes LC, Caramico LA, et al: Parental presence during induction of anesthesia: a randomized controlled trial. Anesthesiology 1996; 84: Kain Z, Caldwell-Andrews A, Maranets I, et al: Predicting which child-parent pair will benefit from parental presence during induction of anesthesia: a decision-making approach. Anesth Analg 2006; 102:81-84 Dahlquist LM, Gil KM, Armstrong FD, et al: Preparing children for medical examinations: the importance of previous medical experience. Health Psychol 1986; 5: Lewyn MJ: Should parents be present while their children receive anesthesia?. Anesth Malpract Protect 1993; May:56-57

9
Medicação Pré-anestésica
Vantagens: Desvantagens: Promover uma separação sem ansiedade. Facilitar a indução anestésica. Bloquear reflexos autonômicos. Reduzir Secreções. Profilaxia da broncoaspiração pulmonar. Prover analgesia. Amnésia .Ansiólise. ‽Prevenção do estresse fisiológico ➜Evitar taquicardia em pacientes especias. Elevação de Custos. ☛ Retardo no despertar. ☛ Retardo na saida da SO e RPA. ☛ Retardo na alta hospitalar. ☛ Agitação pré-operatória. ☛ Comportamento adverso no pós-operatório. ☛ Soluços ! Interações Medicamentosas. ☠ Depressão Ventilatória ! Interacoes medicamentosas:varias drogas podem interferir no sistema de oxidacao do citocroma, afetando o metabolismo de primeira passagem do midazolan. Por exemplo: suco de uva, eritromicina,antiretrovirais,bloqueadores de canal de calcio,deprimem a atividade do CYP3A4., resultado em concentracoes inesperadamente maiores de midazolam e prolongando a sedacao.De maneira inversa, anticonvulsivantes(fenitoina e carbamazepina), rifanpicina,,erva de Sao Joao,glicocorticoides e barbituricos induzem a enzinma 3A4, reduzindo a concentracao de midazolam e asua duracao tb. Viitanen H, Annila P, Viitanen M, Tarkkila P: Premedication with midazolam delays recovery after ambulatory sevoflurane anesthesia in children. Anesth Analg 1999; 89:75-79 Martlew RA, Meakin G, Wadsworth R, et al: Dose of propofol for laryngeal mask airway insertion in children: effect of premedication with midazolam. Br J Anaesth 1996; 76: Brosius KK, Bannister CF: Effect of oral midazolam premedication on the awakening concentration of sevoflurane, recovery times and bispectral index in children. Paediatr Anaesth 2001; 11: Massanari M, Novitsky J, Reinstein LJ: Paradoxical reactions in children associated with midazolam use during endoscopy. Clin Pediatr (Phila)1997;36: McGraw T: Oral midazolam and post-operative behaviour in children. Can J Anaesth 1993; 40: Palkama VJ, Ahonen J, Neuvonen PJ, Olkkola KT: Effect of saquinavir on the pharmacokinetics and pharmacodynamics of oral and intravenous midazolam. Clin Pharmacol Ther 1999; 66:33-39 Bailey DG, Malcolm J, Arnold O, Spence JD: Grapefruit juice-drug interactions. Br J Clin Pharmacol 1998; 46: Ameer B, Weintraub RA: Drug interactions with grapefruit juice. Clin Pharmacokinet 1997; 33: Olkkola KT, Aranko K, Luurila H, et al: A potentially hazardous interaction between erythromycin and midazolam. Clin Pharmacol Ther 1993; 53: Hiller A, Olkkola KT, Isohanni P, Saarnivaara L: Unconsciousness associated with midazolam and erythromycin. Br J Anaesth 1990; 65:
, rifanpicina,,erva de Sao Joao,glicocorticoides e barbituricos induzem a enzinma 3A4, reduzindo a concentracao de midazolam e asua duracao tb. Viitanen H, Annila P, Viitanen M, Tarkkila P: Premedication with midazolam delays recovery after ambulatory sevoflurane anesthesia in children. Anesth Analg 1999; 89: Martlew RA, Meakin G, Wadsworth R, et al: Dose of propofol for laryngeal mask airway insertion in children: effect of premedication with midazolam. Br J Anaesth 1996; 76: Brosius KK, Bannister CF: Effect of oral midazolam premedication on the awakening concentration of sevoflurane, recovery times and bispectral index in children. Paediatr Anaesth 2001; 11: Massanari M, Novitsky J, Reinstein LJ: Paradoxical reactions in children associated with midazolam use during endoscopy. Clin Pediatr (Phila)1997;36: McGraw T: Oral midazolam and post-operative behaviour in children. Can J Anaesth 1993; 40: Palkama VJ, Ahonen J, Neuvonen PJ, Olkkola KT: Effect of saquinavir on the pharmacokinetics and pharmacodynamics of oral and intravenous midazolam. Clin Pharmacol Ther 1999; 66: Bailey DG, Malcolm J, Arnold O, Spence JD: Grapefruit juice-drug interactions. Br J Clin Pharmacol 1998; 46: Ameer B, Weintraub RA: Drug interactions with grapefruit juice. Clin Pharmacokinet 1997; 33: Olkkola KT, Aranko K, Luurila H, et al: A potentially hazardous interaction between erythromycin and midazolam. Clin Pharmacol Ther 1993; 53: Hiller A, Olkkola KT, Isohanni P, Saarnivaara L: Unconsciousness associated with midazolam and erythromycin. Br J Anaesth 1990; 65:")
10
Drogas, Doses e Vias Drogas Via Dose(mg/kg) Tiopental Retal
(solução 10%) 20-40 Diazepam Oral 0,1-0,5 Midazolam 0,25-0,75 Nasal 0,2 0,5-1,0 IM 0,1-0,15 Ketamina + Atropina 3-6 3 6-10 2-10 Clonidina 0,004 Morfina 0,1-0,2 Meperidina 1,0-2,0 Fentanil 0,010-0,015(10-15 mcg/kg) Sufentanil 0,001-0,003(1-3 mcg/kg) Saint-Maurice C, Meistelman C, Rey E, et al: The pharma-cokinetics of rectal midazolam for premedication in children. Anesthesiology 1986; 65: Lindahl SG: The use of midazolam in premedication. Acta Anaesthesiol Scand Suppl 1990; 92:79-83.discussion 107
 Diazepam. Oral. 0,1-0,5. Midazolam. 0,25-0,75. Nasal. 0,2. 0,5-1,0. IM. 0,1-0,15. Ketamina. + Atropina Clonidina. 0,004. Morfina. 0,1-0,2. Meperidina. 1,0-2,0. Fentanil. 0,010-0,015(10-15 mcg/kg) Sufentanil. 0,001-0,003(1-3 mcg/kg) Saint-Maurice C, Meistelman C, Rey E, et al: The pharma-cokinetics of rectal midazolam for premedication in children. Anesthesiology 1986; 65: Lindahl SG: The use of midazolam in premedication. Acta Anaesthesiol Scand Suppl 1990; 92:79-83.discussion 107.")
11
Via Nasal? Greenblatt DJ, Abernethy DR, Locniskar A, et al: Effect of age, gender, and obesity on midazolam kinetics. Anesthesiology 1984; 61:27-35. Feld LH, Negus JB, White PF: Oral midazolam preanesthetic medication in pediatric outpatients. Anesthesiology 1990; 73:

12
Medicação Pré-anestésica

13
Medicação Pré-anestésica
Kain ZN, Caldwell-Andrews AA, Maranets I, et al: Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg 2004; 99:

14
Existem Alternativas?

15
Existem Alternativas?

16
Existem Alternativas?

17
Estresse Pré-operatório Multifatorial

21
Avaliação Pré-anestésica!

22
Qual o Nosso Objetivo ? Sedação Superficial Sedação Profunda

23
Jejum Pré-operatório ✍ 1948: Digby Leigh 1 hr ✔ 1980-1990
Histórico: ✍ 1948: Digby Leigh 1 hr ☞Mendelson 8 hr C. L. Mendelson.The aspiration of stomach contents into the lungs during obstetric anesthesia. American Journal of Obstetrics and Gynecology,St. Louis 1946, 52: ✔ Fatores de risco: Splinter WM, Stewart JA, Muir JG: The effect of preoperative apple juice on gastric contents, thirst, and hunger in children. Can J Anaesth 1989; 36:55-58 Splinter WM, Schaefer JD: Ingestion of clear fluids is safe for adolescents up to 3 h before anaesthesia. Br J Anaesth 1991; 66:48-52 Schreiner MS, Triebwasser A, Keon TP: Ingestion of liquids compared with preoperative fasting in pediatric outpatients. Anesthesiology 1990; 72: Sandhar BK, Goresky GV, Maltby JR, Shaffer EA: Effect of oral liquids and ranitidine on gastric fluid volume and pH in children undergoing outpatient surgery. Anesthesiology 1989; 71: Meakin G, Dingwall AE, Addison GM: Effects of fasting and oral premedication on the pH and volume of gastric aspirate in children. Br J Anaesth 1987; 59: Crawford M, Lerman J, Christensen S, Farrow-Gillespie A: Effects of duration of fasting on gastric fluid pH and volume in healthy children. Anesth Analg 1990; 71: Brady M, Kinn S, O'Rourke K, et al: Preoperative fasting for preventing perioperative complications in children. Cochrane Database Syst Rev 2005.CD005285 Splinter WM, Stewart JA, Muir JG: Large volumes of apple juice preoperatively do not affect gastric pH and volume in children. Can J Anaesth 1990; 37:36-39 Warner MA, Caplan RA, Epstein B: Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: A report by the American Society of Anesthesiologists Task Force on Preoperative Fasting. Anesthesiology 1999; 90: ✎ Incidência em Criancas? Borland LM, Sereika SM, Woelfel SK, et al: Pulmonary aspiration in pediatric patients during general anesthesia: incidence and outcome. J Clin Anesth 1998; 10: Olsson GL, Hallen B, Hambraeus-Jonzon K: Aspiration during anaesthesia: a computer-aided study of 185,358 anaesthetics. Acta Anaesthesiol Scand 1986; 30:84-92. Tiret L, Nivoche Y, Hatton F, et al: Complications related to anaesthesia in infants and children: a prospective survey of anaesthetics. Br J Anaesth 1988; 61: Aspiration occurred in 52 (0.10% or 10.2 per 10,000) of the 50,880 general anesthesia cases. Aspirate was food or gastric contents in 25 cases (0.049% or 4.9 per 10,000), blood in 13 (0.026% or 2.6 per 10,000), and unknown material in 14 (0.0275% or 2.76 per 10,000).
 of the 50,880 general anesthesia cases. Aspirate was food or gastric contents in 25 cases (0.049% or 4.9 per 10,000), blood in 13 (0.026% or 2.6 per 10,000), and unknown material in 14 (0.0275% or 2.76 per 10,000).")
24
Reduzir o Jejum !

25
Qual alimento escolher?
Reduzir o Jejum Qual alimento escolher? Vantagens! Líquidos Claros: → Água → Sucos de frutas coados → Chás claros → Bebidas carbonatadas ➤ Reduzir risco de hipoglicemia: ➵ Debilitados ➵ Desnutridas ➵ Prematuros ➵ Alteracoes Metabólicas ➤ Reduzir sede ➤ Reduzir ansiedade ➤ Melhora na cooperação da criança ➤ Reduzir risco de “roubo” alimentar ➤ Reduzir hipotensão na indução Não se Aplica ao Leite Materno! ➠ Não se Aplica a fórmula. Aun CS, Panesar NS: Paediatric glucose homeostasis during anaesthesia. Br J Anaesth 1990; 64: Jensen BH, Wernberg M, Andersen M: Preoperative starvation and blood glucose concentrations in children undergoing inpatient and outpatient anaesthesia. Br J Anaesth 1982; 54: van der Walt JH, Carter JA: The effect of different pre-operative feeding regimens on plasma glucose and gastric volume and pH in infancy. Anaesth Intensive Care 1986; 14: Welborn LG, McGill WA, Hannallah RS, et al: Perioperative blood glucose concentrations in pediatric outpatients. Anesthesiology 1986; 65: Cote CJ: NPO after midnight for children–a reappraisal. Anesthesiology 1990; 72:

26
Reduzir o Jejum ? Cavell B: Gastric emptying in preterm infants. Acta Paediatr Scand 1979; 68: ; Cavell B: Gastric emptying in infants fed human milk or infant formula. Acta Paediatr Scand 1981; 70:

27
Recomendações a Seguir
< 6 meses 6-36 meses > 36 meses Líquidos Claros 2 hrs 3 hrs 3hrs Leite Materno 4 hrs 6 hrs 8 hrs Formulas Sólidos Devemos Sempre desconfiar das crianças! Schoenfelder RC, Ponnamma CM, Freyle D, et al: Residual gastric fluid volume and chewing gum before surgery. Anesth Analg 2006; 102:

28
Jejum em Situações de Emergência
Borland LM, Sereika SM, Woelfel SK, et al: Pulmonary aspiration in pediatric patients during general anesthesia: incidence and outcome. J Clin Anesth 1998; 10: Olsson GL, Hallen B, Hambraeus-Jonzon K: Aspiration during anaesthesia: a computer-aided study of 185,358 anaesthetics. Acta Anaesthesiol Scand 1986; 30:84-92. Tiret L, Nivoche Y, Hatton F, et al: Complications related to anaesthesia in infants and children: a prospective survey of anaesthetics. Br J Anaesth 1988; 61: Mean gastric residual volume is plotted against hours of fasting before anesthetic induction in emergency pediatric cases. These data suggest that a 4-hour fast, if it does not compromise patient safety, may reduce gastric residual volume and therefore reduce (but not eliminate) risk for aspiration. (Data abstracted from Schurizek BA, Rybro L, Boggild-Madsen NB, Juhl B: Gastric volume and pH in children for emergency surgery. Acta Anaesthesiol Scand 1986; 30: ) Warner MA, Warner ME, Warner DO, et al: Perioperative pulmonary aspiration in infants and children. Anesthesiology 1999; 90:66-71.
 risk for aspiration. (Data abstracted from Schurizek BA, Rybro L, Boggild-Madsen NB, Juhl B: Gastric volume and pH in children for emergency surgery. Acta Anaesthesiol Scand 1986; 30: ) Warner MA, Warner ME, Warner DO, et al: Perioperative pulmonary aspiration in infants and children. Anesthesiology 1999; 90:")
29
Jejum em Situações de Emergência
Mean gastric residual volume is plotted against time from last food ingestion to time of injury. These data suggest that the longer the time from ingestion to injury, the lower the risk for pulmonary aspiration of gastric contents. Also, if more than 4 hours has elapsed between the time of last food ingestion and time of injury, the risk is similar to that for patients with routine fasting. However, even with a 4-hour fasting time period, these patients must still be treated as though they have a full stomach. (Data abstracted from Bricker SRW, McLuckie A, Nightingale DA: Gastric aspirates after trauma in children. Anesthesia 1989; 44: )
")
30
Jejum em Situações de Emergência
Fatores de Risco: Crianças menores de 3 anos: ↓Competência do esfíncter esofagiano inferior Deglutição de ar durante o choro Respiração diafragmatica Esôfago curto ↓ Gradiente de pressão entre estomago e laringe. Tosse ou esgasgos durante manipulação da VA. A maioria da aspirações acontece na indução! Warner MA, Warner ME, Warner DO, et al: Perioperative pulmonary aspiration in infants and children. Anesthesiology 1999; 90:66-71

31
Exames Laboratoriais Todos os exames obtidos no pré-operatório de crianças devem ser guiados pela história, patologias e procedimento cirúrgico. Hemograma e exames de urina não estão indicados como rotina. Patel RI, DeWitt L, Hannallah RS: Preoperative laboratory testing in children undergoing elective surgery: analysis of current practice.J Clin Anesth 1997; 9: Indicações: Procedimentos de grande porte Hemoglobinopatias Prematuros Menores de 6 meses Provas de Coagulação: HPP Cirurgias Reconstrutivas? Adenoamigdalectomia????

33
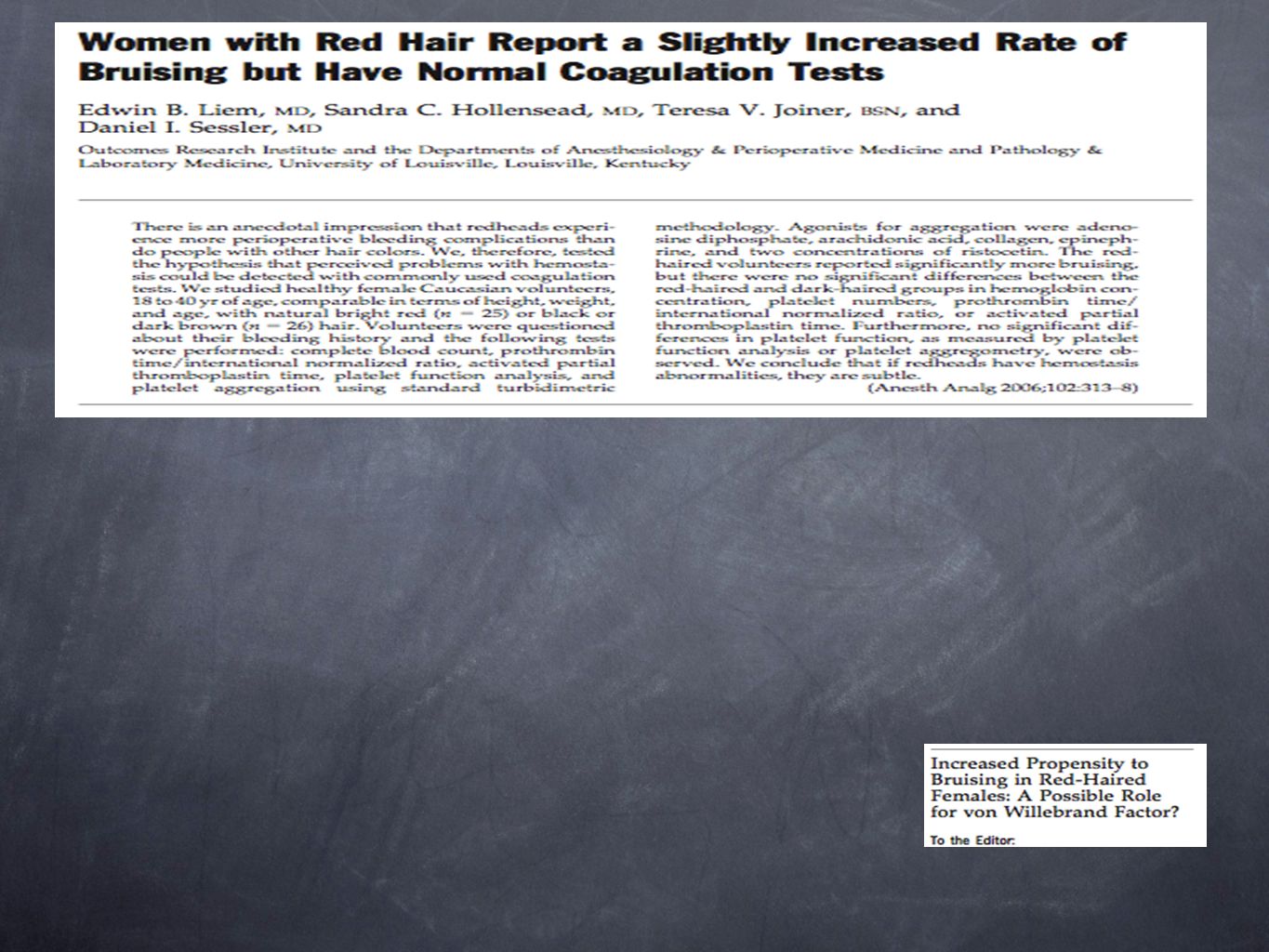
Monitorização da Coagulação

34
Radiografia de Tórax Alario AJ, McCarthy PL, Markowitz R, et al: Usefulness of chest radiographs in children with acute lower respiratory tract disease.J Pediatr 1987; 111: Wood RA, Hoekelman RA: Value of the chest X-ray as a screening test for elective surgery in children Pediatrics 1981; 67:

35
Saturação Basal de O2

36
Outros Exames Glicose Eletrólitos Função Renal Gasometrias
Dosagem de Medicações ECG Ecocardiograma Função Hepática TC RMN Espirometria Conforme HDA, Exame Físico e HPP

37
Causas Não Infecciosas:
Infecção de VAS 20-30% apresentam rinorréia durante períodos significativos! Devemos fazer diagnostico diferencial. Causas Não Infecciosas: Rinite Alérgica Rinite Vasomotora Causas Infecciosas: Infecções Virais Exantemas Infecções Bacterianas Agudas

38
Infecção de VAS Riscos anestesia x IVAS?
Anestesia Geral em crianças com IVAS tem risco pouco conhecido... Koka BV, Jeon IS, Andre JM, et al: Postintubation croup in children. Anesth Analg 1977; 56: Complicações intra-operatórias ( atelectasias, e cianose) mais freqüentes em crianças com IVAS recentes? McGill WA, Coveler LA, Epstein BS: Subacute upper respiratory infection in small children. Anesth Analg 1979; 58: Tait AR, Knight PR: Intraoperative respiratory complications in patients with upper respiratory tract infections. Can J Anaesth 1987; 34: Tait AR, Knight PR: The effects of general anesthesia on upper respiratory tract infections in children. Anesthesiology 1987; 67: Broncoespasmo e laringoespasmo mais freqüentes em crianças com IVAS que foram entubadas. Olsson GL: Bronchospasm during anesthesia: a computer-aided incidence study of 136,929 patients. Acta Anaesthesiol Scand 1987; 31: Olsson GL, Hallen B: Laryngospasm during anesthesia: a computer-aided incidence study in 136,929 patients. Acta Anaesthesiol Scand 1984; 28: Incidência de dessaturação maior em crianças com IVAS. Rolf N, Coté CJ: Frequency and severity of desaturation events during general anesthesia in children with and without upper respiratory infections. J Clin Anesth 1992; 4: Eventos respiratórios adversos mais freqüentes em crianças com IVAS principalmente quando entubadas. Cohen MM, Cameron CB: Should you cancel the operation when a child has an upper respiratory tract infection?. Anesth Analg 1991; 72: Quando comparados TOT e mascara laríngea em crianças com IVAS a incidência de complicações e menor com mascara laríngea. Tait AR, Pandit UA, Voepel-Lewis T, et al: Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal intubation. Anesth Analg 1998; 86: Tartari S, Fratantonio R, Bomben R, et al: [Laryngeal mask vs tracheal tube in pediatric anesthesia in the presence of upper respiratory tract infection]. Minerva Anestesiol 2000; 66:
 mais freqüentes em crianças com IVAS recentes McGill WA, Coveler LA, Epstein BS: Subacute upper respiratory infection in small children. Anesth Analg 1979; 58: Tait AR, Knight PR: Intraoperative respiratory complications in patients with upper respiratory tract infections. Can J Anaesth 1987; 34: Tait AR, Knight PR: The effects of general anesthesia on upper respiratory tract infections in children. Anesthesiology 1987; 67: Broncoespasmo e laringoespasmo mais freqüentes em crianças com IVAS que foram entubadas. Olsson GL: Bronchospasm during anesthesia: a computer-aided incidence study of 136,929 patients. Acta Anaesthesiol Scand 1987; 31: Olsson GL, Hallen B: Laryngospasm during anesthesia: a computer-aided incidence study in 136,929 patients. Acta Anaesthesiol Scand 1984; 28: Incidência de dessaturação maior em crianças com IVAS. Rolf N, Coté CJ: Frequency and severity of desaturation events during general anesthesia in children with and without upper respiratory infections. J Clin Anesth 1992; 4: Eventos respiratórios adversos mais freqüentes em crianças com IVAS principalmente quando entubadas. Cohen MM, Cameron CB: Should you cancel the operation when a child has an upper respiratory tract infection . Anesth Analg 1991; 72: Quando comparados TOT e mascara laríngea em crianças com IVAS a incidência de complicações e menor com mascara laríngea. Tait AR, Pandit UA, Voepel-Lewis T, et al: Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal intubation. Anesth Analg 1998; 86: Tartari S, Fratantonio R, Bomben R, et al: [Laryngeal mask vs tracheal tube in pediatric anesthesia in the presence of upper respiratory tract infection]. Minerva Anestesiol 2000; 66:")
39
Infecção de VAS Não Preditores: Preditores de Eventos adversos:
Idade ? ASA Duração da Anestesia Plano na Extubação Preditores de Eventos adversos: Manuseio de VA (TOT>ML). Relato de “resfriado”. Congestão Nasal. Tabagismo passivo. Característica da Secreção. Uso do Prostigmine. Tipo de Indutor(Tiopental>Hal>Sevo≅Propofol). Ex-prematuros. Cirurgias de VAS. Historia de Hiperrreatividade de VA. Parnis SJ, Barker DS, Van Der Walt JH:Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth 2001;11:29-40. Ouedraogo N, Roux E, Forestier F, et al: Effects of intravenous anesthetics on normal and passively sensitized human isolated airway smooth muscle. Anesthesiology 1998; 88: Cheng EY, Mazzeo AJ, Bosnjak ZJ, et al: Direct relaxant effects of intravenous anesthetics on airway smooth muscle. Anesth Analg 1996; 83: Tait AR, Malviya S, Voepel-Lewis T, et al: Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001; 95:
. Relato de resfriado . Congestão Nasal. Tabagismo passivo. Característica da Secreção. Uso do Prostigmine. Tipo de Indutor(Tiopental>Hal>Sevo≅Propofol). Ex-prematuros. Cirurgias de VAS. Historia de Hiperrreatividade de VA. Parnis SJ, Barker DS, Van Der Walt JH:Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth 2001;11: Ouedraogo N, Roux E, Forestier F, et al: Effects of intravenous anesthetics on normal and passively sensitized human isolated airway smooth muscle. Anesthesiology 1998; 88: Cheng EY, Mazzeo AJ, Bosnjak ZJ, et al: Direct relaxant effects of intravenous anesthetics on airway smooth muscle. Anesth Analg 1996; 83: Tait AR, Malviya S, Voepel-Lewis T, et al: Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001; 95:")
40
Infecção de VAS Outros Preditores: Em Cirurgias Cardíacas:
Pré-medicação com Midazolam. Extubação traqueal em plano profundo. Pico dos sintomas dentro de 4 semanas. Em Cirurgias Cardíacas: Maior incidência de eventos respiratórios. Maior incidência complicações pós-operatórias. Maior incidência de infecções bacterianas. Maior tempo de internação em UTI. Em cirurgia cardiaca:eventos respiratorios(29,2X17,3),complicacoes(25X10,3),infec bacterianas(5,2X1,0),todas com P<0.01, (infecP=0,01).Internacao em UTI 80X60 hrs(P<0,01) Rachel Homer J, Elwood T, Peterson D, Rampersad S: Risk factors for adverse events in children with colds emerging from anesthesia: a logistic regression. Paediatr Anaesth 2007; 17: Malviya S, Voepel-Lewis T, Siewert M, et al: Risk factors for adverse postoperative outcomes in children presenting for cardiac surgery with upper respiratory tract infections. Anesthesiology 2003; 98:
,complicacoes(25X10,3),infec bacterianas(5,2X1,0),todas com P<0.01, (infecP=0,01).Internacao em UTI 80X60 hrs(P<0,01) Rachel Homer J, Elwood T, Peterson D, Rampersad S: Risk factors for adverse events in children with colds emerging from anesthesia: a logistic regression. Paediatr Anaesth 2007; 17: Malviya S, Voepel-Lewis T, Siewert M, et al: Risk factors for adverse postoperative outcomes in children presenting for cardiac surgery with upper respiratory tract infections. Anesthesiology 2003; 98:")
41
Infecção de VAS Resumindo...
Anestesiologistas mais experientes suspendem menos! Crianças com IVAS leves, que não sejam de início agudo, podem ser seguramente anestesiadas para procedimentos de pequeno porte! Caso haja necessidade de EOT, caso deve ser reavaliado. Pré-medicação com broncodilatadores não se provou eficaz! Humidificação, hidratação venosa, e anticolinérgicos podem evitar complicações. Tait AR, Reynolds PI, Gutstein HB: Factors that influence an anesthesiologist's decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995; 7: Cote CJ: The upper respiratory tract infection (URI) dilemma: fear of a complication or litigation?. Anesthesiology 2001; 95: Tait AR, Voepel-Lewis T, Munro HM, et al: Cancellation of pediatric outpatient surgery: economic and emotional implications for patients and their families. J Clin Anesth 1997; 9: DeSoto H, Patel RI, Soliman IE, Hannallah RS: Changes in oxygen saturation following general anesthesia in children with upper respiratory infection signs and symptoms undergoing otolaryngological procedures. Anesthesiology 1988; 68: Elwood T, Morris W, Martin LD, et al: Bronchodilator premedication does not decrease respiratory adverse events in pediatric general anesthesia. Can J Anaesth 2003; 50: Tait AR, Reynolds PI, Gutstein HB: Factors that influence an anesthesiologist's decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995; 7: Tait AR, Burke C, Voepel-Lewis T, et al: Glycopyrrolate does not reduce the incidence of perioperative adverse events in children with upper respiratory tract infections. Anesth Analg 2007; 104:
 dilemma: fear of a complication or litigation . Anesthesiology 2001; 95: Tait AR, Voepel-Lewis T, Munro HM, et al: Cancellation of pediatric outpatient surgery: economic and emotional implications for patients and their families. J Clin Anesth 1997; 9: DeSoto H, Patel RI, Soliman IE, Hannallah RS: Changes in oxygen saturation following general anesthesia in children with upper respiratory infection signs and symptoms undergoing otolaryngological procedures. Anesthesiology 1988; 68: Elwood T, Morris W, Martin LD, et al: Bronchodilator premedication does not decrease respiratory adverse events in pediatric general anesthesia. Can J Anaesth 2003; 50: Tait AR, Reynolds PI, Gutstein HB: Factors that influence an anesthesiologist s decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995; 7: Tait AR, Burke C, Voepel-Lewis T, et al: Glycopyrrolate does not reduce the incidence of perioperative adverse events in children with upper respiratory tract infections. Anesth Analg 2007; 104:")
42
Infecção de VAS Quando Suspender? Contras Prós Relato Familiar
“Ela esta sempre assim” “Já melhorou muito” Pais preocupados:”Piorou noite passada”,sintomas de inicio recente,febre,mal-estar,tosse,perda do apetite Atividade Criança ativa e feliz Letárgica, com aspecto de doente Qualidade da Secreção Rinorréia clara Secreção nasal pururlenta Ausculta Pulmonar Normal Sibilos, estertores, roncos Idade Crianças maiores de 1 ano Menores de 1 ano, ex-prematuros Questões Sociais & Outros fatores Difícil para os pais se ausentarem do trabalho, família vai perder o plano Historia de hiperrreatividade de VAS`s, cirurgias de grande porte, Necessidade de TOT

43
Infecção de VAS Adiar por Quanto Tempo?
Hiperrreatividade de VA`s perdura por até 7 semanas. Adiar por 2 semanas é comum porem sem benefício comprovado. Maioria dos anestesiologistas opta por adiar por 3-4 semanas. O risco começa a cair apos 4-6 semanas. Podemos direcionar nossa técnica anestésica para reduzir os riscos. Empey DW, Laitinen LA, Jacobs L, et al: Mechanisms of bronchial hyperreactivity in normal subjects after upper respiratory tract infection. Am Rev Respir Dis 1976; 113: Collier AM, Pimmel RL, Hasselblad V, et al: Spirometric changes in normal children with upper respiratory infections. Am Rev Respir Dis 1978; 117:47-53. Levy L, Pandit UA, Randel GI, et al: Upper respiratory tract infections and general anaesthesia in children: peri-operative complications and oxygen saturation. Anaesthesia 1992; 47: Tait AR, Reynolds PI, Gutstein HB: Factors that influence an anesthesiologist's decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995; 7: Tait AR, Malviya S, Voepel-Lewis T, et al: Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001; 95:

44
Medicina Baseada em Evidências?
Obrigado

Apresentações semelhantes
 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")





. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")












