Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Laboratório de Imunologia Aplicada Dept
Laboratório de Imunologia Aplicada Dept. de Microbiologia e Parasitologia Centro de Ciências Biológicas Vacinas contra HIV Prof. Aguinaldo R. Pinto

2
20 anos após a descoberta do HIV...............

3
40 milhões de soropositivos

4
A pandemia somente será interrompida por uma vacina que seja:
Segura Eficaz Barata Estável Simples de ser administrada

5
Questões a serem resolvidas de ordem:
Política Prática Econômica Social Ética Biologia básica do HIV

6
Porque ainda não temos uma vacina contra HIV?
HIV não resulta em imunidade protetora Caxumba, rubéola, sarampo Infecção é persistente, longa, letalidade de 98% dos infectados SI não é capaz de eliminar o vírus Mecanismos imunes que impeçam re-infecções não são conhecidos

7
Porque ainda não temos uma vacina contra HIV?
Difícil neutralização por Anticorpos Progressiva destruição dos linfócitos T CD4 “Evolução” viral, levando ao escape Diversidade viral Down-regulation de MHC I Integração pró-vírus em células CD4 Reservatórios

8
Challenges in the development of an HIV vaccine
Scientific challenges: HIV variability Lack of Immune correlates of protection Limitation of animal models Logistical challenges: Multiple clinical trials required Research in developing countries Ethical considerations Financial challenges Low investment (compared with drugs) Future “markets”
 Future markets")
9
HIV vaccine approaches
recombinant protein gp120 synthetic peptides (V3) naked DNA live-recombinant vectors (viral, bacterial) whole-inactivated virus live-attenuated virus
 naked DNA. live-recombinant vectors. (viral, bacterial) whole-inactivated virus. live-attenuated virus.")
10
How vaccines are developed?
Basic research Preclinical development Clinical trials Phase I/II Phase III Safety, Immunogenicity Discovery Human research in vitro & animal studies Laboratory Exploration Efficacy Vaccine concept Experiments in primates Human trials 1 2 3 4 5 6 Safety, immunogenicity Likelihood of protection in humans 1: Recombinant Protein – 2: Synthetic Peptides – 3: Naked DNA 4. Live-recombinant vectors- 5: Whole inactivated virus – 6: Live attenuated virus

11
What are the steps in Vaccine development?
Phase I: volunteers, 8-12 months Phase II: volunteers,18-24 months Phase III: Thousands of volunteers, 3 or more years Before talking about recent progress in vaccine development and trials that are ongoing, let’s review the steps in vaccine development. Clinical trials for a candidate vaccine are divided into three distinct phases. Phase I trials are the first human tests of a candidate vaccine, generally conducted on small numbers (10-30) of healthy adult volunteers who are not at risk for the disease in question. The main goal is evaluation of safety, and to a lesser extent, analysis of the immune responses evoked by the vaccine and of different vaccine doses and immunization schedules. A Phase I trial usually takes 8-12 months to complete. Phase II testing involves a larger number of volunteers (50-500), usually a mixture of low-risk people and higher-risk individuals from the population where Phase III (vaccine efficacy) trials will eventually be conducted. Phase II trials generate additional safety data as well as information for refining the dosage and immunization schedule. Although not set up to determine whether the vaccine actually works, Phase II trials are sometimes large enough to yield preliminary indications of efficacy. These trials generally take months, with the increase over Phase I due primarily to the additional time required for screening and enrolling larger numbers of trial participants. Phase III trials are the definitive test of whether a vaccine is effective in preventing disease. Using thousands of volunteers from high-risk populations in geographic regions where HIV is circulating, the incidence of HIV in vaccinated people is compared to that in people who receive a placebo. Successful demonstration of efficacy in a Phase III trial can then lead to an application for licensure of the vaccine. Phase III trials of AIDS vaccines are generally expected to require a minimum of three years for enrollment, immunizations, and assessments of efficacy.
 of healthy adult volunteers who are not at risk for the disease in question. The main goal is evaluation of safety, and to a lesser extent, analysis of the immune responses evoked by the vaccine and of different vaccine doses and immunization schedules. A Phase I trial usually takes 8-12 months to complete. Phase II testing involves a larger number of volunteers (50-500), usually a mixture of low-risk people and higher-risk individuals from the population where Phase III (vaccine efficacy) trials will eventually be conducted. Phase II trials generate additional safety data as well as information for refining the dosage and immunization schedule. Although not set up to determine whether the vaccine actually works, Phase II trials are sometimes large enough to yield preliminary indications of efficacy. These trials generally take months, with the increase over Phase I due primarily to the additional time required for screening and enrolling larger numbers of trial participants. Phase III trials are the definitive test of whether a vaccine is effective in preventing disease. Using thousands of volunteers from high-risk populations in geographic regions where HIV is circulating, the incidence of HIV in vaccinated people is compared to that in people who receive a placebo. Successful demonstration of efficacy in a Phase III trial can then lead to an application for licensure of the vaccine. Phase III trials of AIDS vaccines are generally expected to require a minimum of three years for enrollment, immunizations, and assessments of efficacy.")
12
HIV Vaccines: Current Pipeline Situation
Vaccine Constructs in Concept Stage 66 # GMP lots made 25 # Entered Phase I 25 # Entered Phase II 5 # Entered Phase III 2

13
Progress toward AIDS vaccine since 2000
30 AIDS vaccines in small-clinical trials Developing countries taking a lead Demonstration that large scale AIDS vaccine trials can be conducted Much progress has been made since 2000. The number of AIDS vaccine candidates in small-scale human trials has doubled since The number of countries and agencies involved has also grown. Currently, more than 30 candidate AIDS vaccines are being tested in small-scale human clinical trials, the majority of which began in the past five years. These trials span 19 countries on six continents. The number of agencies working toward a vaccine has increased as well. Four pharmaceutical companies have vaccine candidates in trials, up from two in 2000. Developing countries, which in 2000 participated in vaccine research and development only marginally, are now helping lead the field. In 2000, one African country, Uganda, was conducting an AIDS vaccine trial. Today, four African countries have small-scale trials underway, and five others are preparing for trials. The first-ever AIDS vaccine trials in India are expected to begin later this year. As the number of small-scale trials in developing countries grows, so too does capacity to conduct these trials. Throughout Africa, Asia and Latin America, state-of-the-art clinics and laboratories, staffed by local physicians and technicians, exist where four years ago there were none. It is critical that developing countries conduct AIDS vaccine trials because the incidence of new HIV infections is among the highest in these areas. In addition, the subtypes of HIV circulating in developing countries are different from the subtype common in industrialized countries. Scientists do not yet know if or how subtype will impact a vaccineユs effectiveness. The first-ever large-scale AIDS vaccine trials were completed in A third large-scale trial began last fall, and a fourth is expected to begin later this year. To be fully evaluated for safety and effectiveness, a vaccine candidate must first be tested in small-scale trials, then tested in large-scale trials. Until last year, no AIDS vaccine candidate had ever completed a large-scale trial. In early 2003, a large-scale trial of VaxGenユs AIDSVAX candidate was completed in North America. Later in 2003, a second trial of AIDSVAX was completed in Thailand. Although both trials found the candidates to be ineffective, the trials themselves were major milestones. Before these trials were completed there were many that doubted that you could even logistically carry out this sort of research. The VaxGen trials demonstrated that it is possible to recruit thousands of volunteers for an AIDS vaccine trial and retain them over a three-year observation period.

14
What types of HIV vaccines are being tested?
Peptide epitopes (protein fragments) Status: In phase I trials Live attenuated HIV Status: Non-human primates Whole, killed HIV Status: Not under study in primates eptides The "peptide" vaccine concept is based on the identification and chemical synthesis of B cell and T cell epitopes, particularly those that may be immunodominant and induce specific immune functions (neutralization, killing, help). In their simplest form, peptides used as vaccine candidates are linear polymers of ~ 8 -24 amino acids. These vaccines are simple and cheap to make, but they only represent a limited amount of HIV material, and there are issues with the peptides remaining stable, which could be a challenge in trying to disseminate the vaccine in resource poor settings. Live, attenuated virus vaccines mimic natural exposure while avoiding disease, in the expectation that immunologic memory and lifelong immunity will be induced, just as in youngsters who recover from the usual childhood infections. These vaccines effectively induce both humoral and cell-mediated immunity, and generally require only one or two immunizations, since the immune responses they induce are very durable. While most licensed vaccines in use today for other diseases are based on this concept, formidable safety concerns have limited research on live, attenuated HIV vaccines in humans. A whole-killed AIDS vaccine uses HIV that has been rendered incapable of replication, usually through chemical treatment. Such vaccines have proven useful in other viral diseases, and are potentially safer than live-attenuated virus vaccines, provided that complete inactivation is achieved in the manufactured product. The primary advantage of this approach is that all of the viral antigens are presented in a completely "native" form. Its primary disadvantage is the difficulty in maintaining this "native" configuration during the chemical inactivation required to render the product safe for humans. It is also difficult to make large quantities of this type of vaccine. Naked DNA Vaccines DNA immunization uses the genes for viral antigens, rather than the antigens themselves, as the source of immunogen. In DNA immunization, the host is immunized by direct administration of viral genes; the genes are composed of DNA that encode for the antigen that would normally be produced by the cell infected with the virus. The vaccinee's cells take up the DNA and produce viral antigen by normal cellular mechanisms. The newly-formed antigen is then presented on the cell surface with host MHC class I and class II molecules where contact with immunocompetent cells evokes an immune response. Naked DNA Status: Phase I trials
 Status: In phase I trials. Live attenuated HIV. Status: Non-human primates. Whole, killed HIV. Status: Not under study in primates. eptides The peptide vaccine concept is based on the identification and chemical synthesis of B cell and T cell epitopes, particularly those that may be immunodominant and induce specific immune functions (neutralization, killing, help). In their simplest form, peptides used as vaccine candidates are linear polymers of ~ amino acids. These vaccines are simple and cheap to make, but they only represent a limited amount of HIV material, and there are issues with the peptides remaining stable, which could be a challenge in trying to disseminate the vaccine in resource poor settings. Live, attenuated virus vaccines mimic natural exposure while avoiding disease, in the expectation that immunologic memory and lifelong immunity will be induced, just as in youngsters who recover from the usual childhood infections. These vaccines effectively induce both humoral and cell-mediated immunity, and generally require only one or two immunizations, since the immune responses they induce are very durable. While most licensed vaccines in use today for other diseases are based on this concept, formidable safety concerns have limited research on live, attenuated HIV vaccines in humans. A whole-killed AIDS vaccine uses HIV that has been rendered incapable of replication, usually through chemical treatment. Such vaccines have proven useful in other viral diseases, and are potentially safer than live-attenuated virus vaccines, provided that complete inactivation is achieved in the manufactured product. The primary advantage of this approach is that all of the viral antigens are presented in a completely native form. Its primary disadvantage is the difficulty in maintaining this native configuration during the chemical inactivation required to render the product safe for humans. It is also difficult to make large quantities of this type of vaccine. Naked DNA Vaccines DNA immunization uses the genes for viral antigens, rather than the antigens themselves, as the source of immunogen. In DNA immunization, the host is immunized by direct administration of viral genes; the genes are composed of DNA that encode for the antigen that would normally be produced by the cell infected with the virus. The vaccinee s cells take up the DNA and produce viral antigen by normal cellular mechanisms. The newly-formed antigen is then presented on the cell surface with host MHC class I and class II molecules where contact with immunocompetent cells evokes an immune response. Naked DNA. Status: Phase I trials.")
15
What types of HIV vaccines are being tested?
Recombinant Viral Proteins Status: Phase II and III trials Live bacterial vectors Status: Phase I trials Live Viral Vectors Status: Phase II trials Naked DNA Vaccines DNA immunization uses the genes for viral antigens, rather than the antigens themselves, as the source of immunogen. In DNA immunization, the host is immunized by direct administration of viral genes; the genes are composed of DNA that encode for the antigen that would normally be produced by the cell infected with the virus. The vaccinee's cells take up the DNA and produce viral antigen by normal cellular mechanisms. The newly-formed antigen is then presented on the cell surface with host MHC class I and class II molecules where contact with immunocompetent cells evokes an immune response. RECOMBINANT VIRAL SURFACE PROTEIN VACCINES HIV subunit vaccines use viral surface antigens, particularly gp120 and gp160, to evoke an immune response. Subunit vaccines consist of small protein or peptide portions of pathogenic virus. They can be made by genetically engineering bacteria, yeast, insect or mammalian cell cultures to produce protein subunit antigens.Envelope subunit and peptide approaches were among the earliest attempts to make an HIV vaccine, based on the premise that the envelope protein is a prominent, "visible", and important target which binds to cells and facilitates viral entry. LIVE VECTOR VACCINES Live recombinant vector vaccines are constructed by inserting HIV or SIV genes into live, infectious, but non-disease-causing viruses or bacteria such as vaccinia virus or Bacille Calmette-Guerin (BCG). These vaccines are produced by engineering viral or bacterial genomes to express the desired HIV antigen(s). Viral vectors can be constructed to contain one or more viral genes that cause infected cells to make the coded protein in native form. Recombinant viral vectors enter cells and allow the HIV or SIV proteins to be generated inside the cells; these proteins are then presented to the immune system in the same way that proteins from a virus-infected cell would be. As a result, vector-based vaccines induce both humoral and cellular immune responses. The antibody response to some live vector experimental vaccines can be substantially augmented by subsequent boost with recombinant subunit protein vaccines. In addition, some live vector vaccines may be capable of generating a mucosal immune response. PSEUDOVIRIONS Virus-like particles (VLP) take advantage of the fact that the immune system responds well to particulate antigens that are the size of viruses. The self-assembling core structures of many different viruses can be adapted by recombinant technology to contain or display one or more antigens of HIV (or SIV). Since these particles neither replicate nor contain the HIV genome, they cannot produce progeny virus and so avoid the formidable safety concerns associated with whole-inactivated and live-attenuated virus vaccines. "Pseudovirions" or genetically inactivated HIV, are a special kind of VLP. They are self-assembling, non- replicating, virus-sized structures that closely resemble the intact HIV virion. Pseudovirions Status: Pre-clinical trials
. These vaccines are produced by engineering viral or bacterial genomes to express the desired HIV antigen(s). Viral vectors can be constructed to contain one or more viral genes that cause infected cells to make the coded protein in native form. Recombinant viral vectors enter cells and allow the HIV or SIV proteins to be generated inside the cells; these proteins are then presented to the immune system in the same way that proteins from a virus-infected cell would be. As a result, vector-based vaccines induce both humoral and cellular immune responses. The antibody response to some live vector experimental vaccines can be substantially augmented by subsequent boost with recombinant subunit protein vaccines. In addition, some live vector vaccines may be capable of generating a mucosal immune response. PSEUDOVIRIONS Virus-like particles (VLP) take advantage of the fact that the immune system responds well to particulate antigens that are the size of viruses. The self-assembling core structures of many different viruses can be adapted by recombinant technology to contain or display one or more antigens of HIV (or SIV). Since these particles neither replicate nor contain the HIV genome, they cannot produce progeny virus and so avoid the formidable safety concerns associated with whole-inactivated and live-attenuated virus vaccines. Pseudovirions or genetically inactivated HIV, are a special kind of VLP. They are self-assembling, non- replicating, virus-sized structures that closely resemble the intact HIV virion. Pseudovirions. Status: Pre-clinical trials.")
16
Immune correlates Different vaccine concepts are explored
What type of immune response can protect against HIV infection or progression to AIDS? Humoral immunity (neutralizing Ab) Cell-mediated immunity (CTLs, T helper cells) Mucosal immunity Combination of all ? Different vaccine concepts are explored targeting different types of immune response(s)
 Cell-mediated immunity (CTLs, T helper cells) Mucosal immunity. Combination of all Different vaccine concepts are explored. targeting different types of immune. response(s)")
17
Three “waves” of HIV vaccine paradigms and clinical trials
First “wave” ( mid 1990s): Induction of neutralizing antibodies Envelope antigens Second “wave” (mid 1990s - early 2000s) Induction of cell-mediated immunity (CD 8 CTL) Live vectors, DNA vaccines Prime-boost combinations (pox-vectors + gp120) Third “wave” (now) Better/broader immune responses Novel immunogens and combinations
: Induction of neutralizing antibodies. Envelope antigens. Second wave (mid 1990s - early 2000s) Induction of cell-mediated immunity (CD 8 CTL) Live vectors, DNA vaccines. Prime-boost combinations (pox-vectors + gp120) Third wave (now) Better/broader immune responses. Novel immunogens and combinations.")
18
Vacinas contra HIV Anticorpos neutralizantes
Linfócitos T CD8+ específicos Diversidade genética

19
What Does an HIV Vaccine Need to Do?
Bind up free virions in infected secretions Binding Antibodies Neutralization

20
Anticorpos neutralizantes - AcN
Glicoproteínas de superfície do HIV são resistentes à ligação de Ac neutralizantes: Extensa glicosilação impede ligação de anticorpos; Quando aparecem AcN eficazes, ocorre uma rápida seleção de vírus resistentes a essa neutralização; alças hipervariáveis mascaram os epítopos importantes do envelope viral. Ex: CCR5

21
Anticorpos neutralizantes - AcN

22
Anticorpos monoclonais neutralizantes
2 clones principais: b12 e 2G12 Uso profilático (SHIV) Administração tópica em cremes vaginais Dificuldades Grande quantidades Várias doses Muito caro
 Administração tópica em cremes vaginais. Dificuldades. Grande quantidades. Várias doses. Muito caro.")
23
Anticorpos neutralizantes - AcN
AIDSVAX B/B e B/E gp 120 recombinante Tailândia e EUA – voluntários Não induziu anticorpos neutralizantes

24
Vacinas contra HIV Anticorpos neutralizantes
Linfócitos T CD8+ específicos Diversidade genética

25
What Does an HIV Vaccine Need to Do?
Produce T cell memory to eliminate HIV infected cells HIV Infected Cell CTL CTL Apoptotic Death Kill

26
Linfócitos T CD8+ específicos
Induzir linfócitos T CD8 específicos que controlem a replicação viral: Destruição de células infectadas Secrecção de citocinas (INF-, TNF-α) Secrecção de quimiocinas (RANTES, MIP 1-α, MIP 1β) – bloqueio dos co-receptores
 Secrecção de quimiocinas (RANTES, MIP 1-α, MIP 1β) – bloqueio dos co-receptores.")
27
Linfócitos T CD8+ específicos
Good points: Indivíduos HIV-positivos progressores lentos apresentam altos níveis de células T CD8+ Estudos em primatas com SIV, mostram que a depleção de CD8+ faz com eles evoluam rapidamente para AIDS Grupo de prostitutas em Nairóbi recorrentemente expostas e HIV negativas

28
Linfócitos T CD8+ específicos
Bad points: Células T CD8+ reconhecem células infectadas apenas após infecção. Vacinas que estimulam principalmente células T não devem induzir imunidade esterilizante.

29
Controle da replicação viral após infecção
Viral load set point Controle da replicação viral após infecção Diminuir disseminação viral

30
Mathematical Model of Impact of a Vaccine That Reduced Viral Load Over Time (Ira Longini, Emory University) Prevalence of HIV in Population Years

31
Porque indivíduos com células T CD8 específicas evoluem para AIDS?
HIV desenvolve mecanismos de escape NEF diminui a expressão de moléculas de MHC Depleção de células CD4 impede o auxílio que estas células fornecem às células T CD8

32
Porque uma vacinas baseada em Linfócitos T CD8+ funcionaria?
Os linfócitos T CD8 específicos estarão presentes desde o início da infecção e portanto serão mais eficazes do que aqueles estimulados pela infecção natural, uma vez que terão todo o suporte das células T CD4.

33
Vacinas contra HIV Anticorpos neutralizantes
Linfócitos T CD8+ específicos Diversidade genética

35
Diversidade genética Muitas dessas mutações são deletérias ao vírus
Transcriptase reversa não tem capacidade de corrigir erros 1 nucleotídeo errado a cada Muitas dessas mutações são deletérias ao vírus Diversidade em termos de amino-ácido 15 % gag e 30 % env Influenza > 2% requer nova vacina

36
High genetic diversity of HIV-1 is perceived as a major obstacle for the development of globally effective HIV vaccines The genetic diversity of HIV-1 strains can vary significantly. For example, in the env gene it can range : In a single individual: up to 8-10 % Between different individuals in the same population: up to 20% Between populations in diverse geographical locations: up to 35 %

37
Diversidade genética n= 23 n= 193

38
Ensaios clínicos Primeira Fase I – início em 1987
5 anos após isolamento do HIV Primeira Fase III (gp 120 recombinante) AIDSVAX B/B – EUA – 5009 indivíduos, a maioria homosexuais AIDSVAX B/E – Tailândia – 2546 indivíduos usuários de droga injetáveis NÃO INDUZIU PROTEÇÃO!!!!
 AIDSVAX B/B – EUA – 5009 indivíduos, a maioria homosexuais. AIDSVAX B/E – Tailândia – 2546 indivíduos usuários de droga injetáveis. NÃO INDUZIU PROTEÇÃO!!!!")
39
Examples of Products in Development
Adeno-associated virus (A,C) Adenovirus (B) Canarypox (A) DNA (A, B, C) Fowlpox (B) MVA (A, B) Salmonella-DNA (A, B) VEE replicon (C)
 Adenovirus (B) Canarypox (A) DNA (A, B, C) Fowlpox (B) MVA (A, B) Salmonella-DNA (A, B) VEE replicon (C)")
40
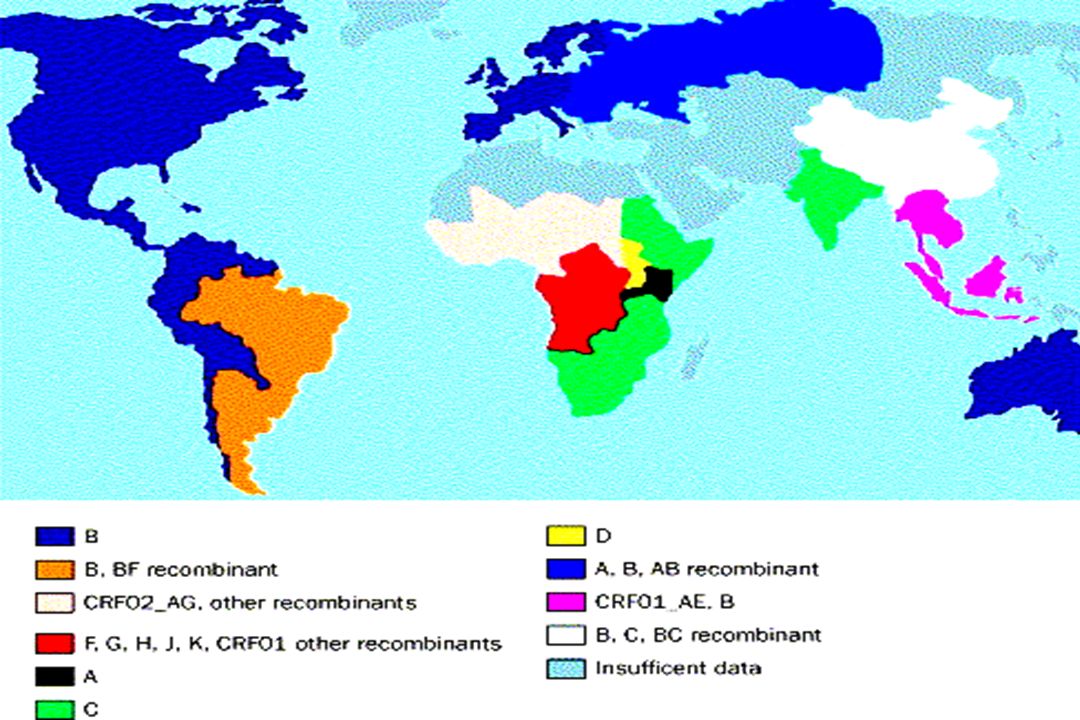
Where are these vaccines being tested?
This slide shows past, present and future sites for HIV vaccine trials. It is important to note that trials are being undertaken in the global north as well as the global south. It is important to test vaccines in multiple settings. There are two major HIV variants that are responsible for the global epidemic, HIV-1 and HIV-2. These two viruses are quite different, and a vaccine generated against one will not necessarily provide protection against the other. Therefore, when companies and researchers are designing vaccines, the strain that they use to derive the DNA and proteins is an important consideration. What offers protection from the dominant strain in the US may not offer protection in regions of Africa or in Asia.

41
What are the animal models for HIV vaccines?
Macaques Chimpanzees Scientists are using macaque monkeys infected with simian immunodeficiency virus (SIV), a virus closely related to HIV. This model is useful because SIV in macaques follows a similar disease course to HIV, and adequate numbers of animals are available. A potential shortcoming is that SIV and HIV, though similar, are different viruses, so that advances made with SIV need to be verified using HIV. Macaques are being used to evaluate a variety of SIV vaccines of the same type as HIV vaccines being developed for humans. Since the monkeys can be challenged with SIV after immunization, the vaccines can be evaluated for their ability to protect from virus infection or disease in the monkeys. Chimeric viruses containing the HIV envelope gene in place of the SIV envelope gene in the SIV virus (called SHIVs), can be used to test HIV envelope vaccines for their ability to protect from infection with the SHIV viruses. Vaccine researchers are also using the chimpanzee for evaluation of HIV vaccines, since chimpanzees can be infected with HIV. Although this model is very valuable - since it uses the same virus that infects humans - chimpanzees are expensive and typically do not develop the same disease complications as humans. This makes it impossible to evaluate a vaccine's effect on the course if disease.
, a virus closely related to HIV. This model is useful because SIV in macaques follows a similar disease course to HIV, and adequate numbers of animals are available. A potential shortcoming is that SIV and HIV, though similar, are different viruses, so that advances made with SIV need to be verified using HIV. Macaques are being used to evaluate a variety of SIV vaccines of the same type as HIV vaccines being developed for humans. Since the monkeys can be challenged with SIV after immunization, the vaccines can be evaluated for their ability to protect from virus infection or disease in the monkeys. Chimeric viruses containing the HIV envelope gene in place of the SIV envelope gene in the SIV virus (called SHIVs), can be used to test HIV envelope vaccines for their ability to protect from infection with the SHIV viruses. Vaccine researchers are also using the chimpanzee for evaluation of HIV vaccines, since chimpanzees can be infected with HIV. Although this model is very valuable - since it uses the same virus that infects humans - chimpanzees are expensive and typically do not develop the same disease complications as humans. This makes it impossible to evaluate a vaccine s effect on the course if disease.")
42
Animal models Three major animal models: SIV in monkeys
SHIV in monkeys Different candidate vaccines induce different types of protection in different animals: gp120 protects chimps but not macaques protection in macaques is usually “incomplete” (no sterilizing immunity, only decreasing virus loads) No clear immunological correlate of protection Relevance of these animal models in terms of human protection is not clear and they need to be validated
 No clear immunological correlate of protection. Relevance of these animal models in terms of. human protection is not clear and they need. to be validated.")
43
Surrogate Challenge Model
VVgag Inject ip 5 days Homogenize, Freeze Thaw Gag-specific CD8+ T cells

44
Vacinas Problemas éticos Interesses Pesquisador Indústria farmacêutica
Governo Comunidade

45
extensão

46
Perguntas?

Apresentações semelhantes


















>")
 foi alertado para o aparecimento de uma nova doença. Em oito meses apareceram, na.>")