Carregar apresentação
A apresentação está carregando. Por favor, espere

1
TROMBECTOMIA POR ASPIRAÇÃO MANUAL NO IAM
Julho / 2010 TROMBECTOMIA POR ASPIRAÇÃO MANUAL NO IAM Estratégia seletiva ou para todos? Jamil Abdalla Saad Hospital Felicio Rocho/ SOCOR Belo Horizonte MG

2
Hospital Felicio Rocho/ SOCOR
Julho / 2010 Estratégia seletiva ou para todos? ATC primária no IAM ? Stent em angioplastia ? Stent farmacológico ? PAMI DEBATE I / II ???? Jamil Abdalla Saad Hospital Felicio Rocho/ SOCOR Belo Horizonte MG

3
Ruptura de placa com trombo oclusivo
IAM: Fisiopatologia Ruptura de placa com trombo oclusivo Fonte: G Stone - TCTMD 3 3

10
Qual o tamanho do trombo?
Fonte: C Grines - TCTMD

11
Impacto da Embolização distal
Falha de enchimento no sítio primário da ATC Tromboembolia distal 27 de 178 (15%) pts após ATC primaria ↓ res ST ↑área Infarto ↑ Mortalidade Henriques JPS et al. EHJ 2002;23:1112-7 Fonte: G Stone - TCTMD
 pts após ATC primaria ↓ res ST. ↑área Infarto. ↑ Mortalidade. Henriques JPS et al. EHJ 2002;23: Fonte: G Stone - TCTMD.")
12
Momento da embolização distal
64 (de 400) pacientes com ED Napodano M. TCT 2005
 pacientes com ED. Napodano M. TCT")
13
Abordagem mecânica do trombo
Aspiração (Rinspirator, Pronto, Export, Rescue, Diver CE, etc.) Thrombectomia (AngioJet, X-Sizer) GuardWire, FilterWire, AngioGuard, EmboShield, etc. Proteção distal (GuardWire, FilterWire, AngioGuard, etc.) Fonte: G Stone - TCTMD
 Thrombectomia. (AngioJet, X-Sizer) GuardWire, FilterWire, AngioGuard, EmboShield, etc. Proteção distal (GuardWire, FilterWire, AngioGuard, etc.) Fonte: G Stone - TCTMD.")
14
Trombectomia e proteção distal no IAM
Partículas embólicas retiradas em mais de 75% dos casos De Luca G, et al. Am Heart J. 2007;153:343–353. Fonte: G Stone - TCTMD De Luca G, et al. Am Heart J. 2007;153:343–353. 14 14

16
Devices adicionais no IAM
Metanálise de 21 trials com 3721 pacientes Device Controle OR p TIMI-3 pós 89.4% 87.1% 1.34 0.03 TMPG 3 pós 48.8% 36.5% 2.21 <0.001 Mortalidade 2.5% 2.6% 0.97 NS De Luca G. Am Heart J 2007;153:343-53 Fonte: C Grines - TCTMD

17
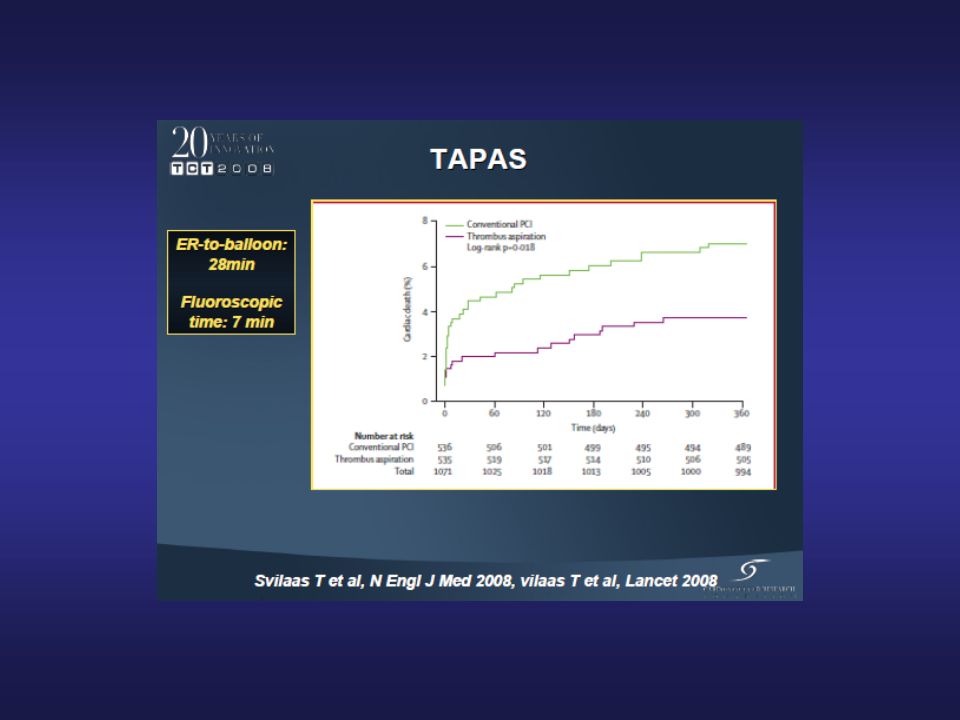
TAPAS: 1071 pacientes IAMSST = ICP primária
Randomizados ( CONVENCIONAL X ASPIRAÇÃO) - Único centro; desfechos substitutos Randomização antes da angiografia Critérios de inclusão amplos Exclusão (expectativa < 06 meses; salvamento) Análise histopatológica do material Svilaas T et al. NEJM 2008;358;
 - Único centro; desfechos substitutos. Randomização antes da angiografia. Critérios de inclusão amplos. Exclusão (expectativa < 06 meses; salvamento) Análise histopatológica do material. Svilaas T et al. NEJM 2008;358;")
18
TAPAS: 1071 pacientes IAMSST = ICP primária
Randomizados ( CONVENCIONAL X ASPIRAÇÃO) Myocardial Blush (1 EP) ST-segment Resolution P<0.001 P<0.001 Thrombus aspiration Conventional PCI Thrombus aspiration Conventional PCI Svilaas T et al. NEJM 2008;358; Fonte: G Stone - TCTMD
 Myocardial Blush (1 EP) ST-segment Resolution. P< P< Thrombus. aspiration. Conventional. PCI. Thrombus. aspiration. Conventional. PCI. Svilaas T et al. NEJM 2008;358; Fonte: G Stone - TCTMD.")
19
TAPAS: 1071 pacientes IAMSST = ICP primária
Randomizados ( CONVENCIONAL X ASPIRAÇÃO) Vlaar et al. Lancet 2008;371: Fonte: G Stone - TCTMD
 Vlaar et al. Lancet 2008;371: Fonte: G Stone - TCTMD.")
20
TAPAS: 1071 pacientes IAMSST = ICP primária
Randomizados ( CONVENCIONAL X ASPIRAÇÃO) 10% INSUCESSO PRIMÁRIO Svilaas T et al. NEJM 2008;358;
 10% INSUCESSO. PRIMÁRIO. Svilaas T et al. NEJM 2008;358;")
22
Thrombectomy Plus PCI (n = 88)
EXPIRA – resultados pós procedimento e 9 meses Standard PCI (n = 87) Thrombectomy Plus PCI (n = 88) P Value Post-Stent Myocardial Blush Grade ≥ 2a 59.8% 88.6% < 90-Minute ST-Segment Resolutiona 39.1% 63.6% 0.001 9-Month Cardiac Death 4.6% 0% 0.02 Sardella et al. JACC 2009;53:309-31 AHA Nov. 14 : 2009
 Thrombectomy Plus PCI (n = 88) P Value. Post-Stent Myocardial Blush Grade ≥ 2a. 59.8% 88.6% < Minute ST-Segment Resolutiona. 39.1% 63.6% Month Cardiac Death. 4.6% 0% Sardella et al. JACC 2009;53: AHA Nov. 14 :")
23
Thrombectomy Plus PCI (n = 88)
EXPIRA – eventos adversos aos 2 anos Standard PCI (n = 87) Thrombectomy Plus PCI (n = 88) P Value Cardiac Death 6.8% 0% 0.0001 Reinfarction 1.1% 0.999 TVR 5.7% 4.5% 0.651 MACE 13.6% 0.050 Sardella et al. JACC 2009;53:309-31 AHA Nov. 14 : 2009
 Thrombectomy Plus PCI (n = 88) P Value. Cardiac Death. 6.8% 0% Reinfarction. 1.1% TVR. 5.7% 4.5% MACE. 13.6% Sardella et al. JACC 2009;53: AHA Nov. 14 :")
24
REDUZINDO A EMBOLIZAÇÃO DISTAL
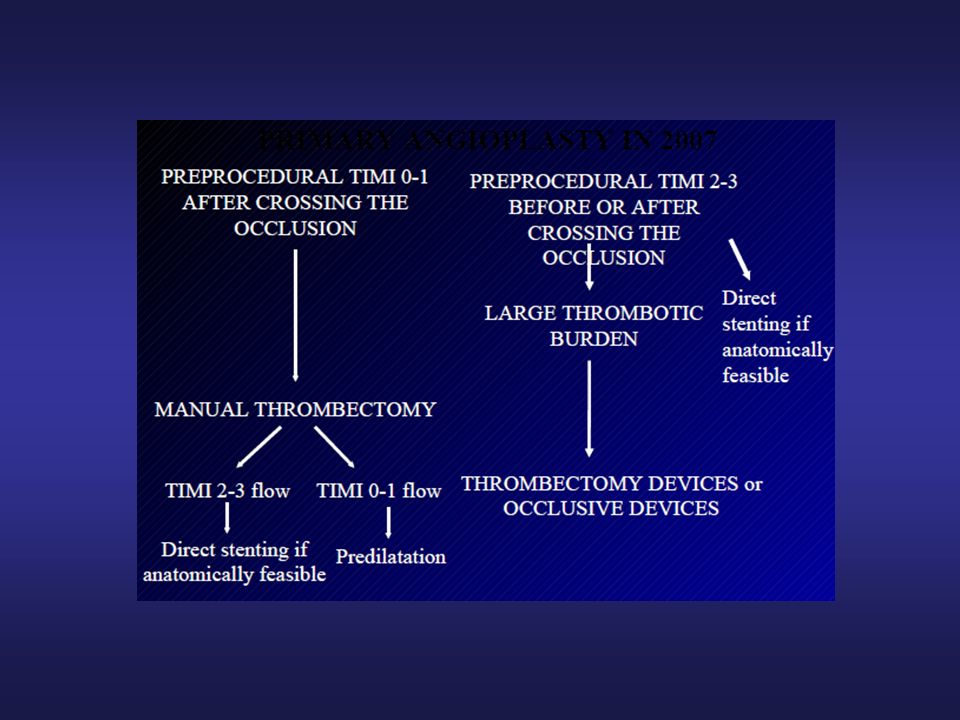
TIMI 0-1 após Guia .014” TIMI 2-3 antes/após Guia .014” Stent direto (se viável) Trombectomia manual TTS elevado(>3) TIMI 2-3 TIMI 0-1 Trombectomia manual / Proteção distal Stent direto (se viável) Pré-dilatação
 Trombectomia manual. TTS elevado(>3) TIMI 2-3. TIMI 0-1. Trombectomia manual. / Proteção distal. Stent direto. (se viável) Pré-dilatação.")
25
Estratégia seletiva ou para todos?
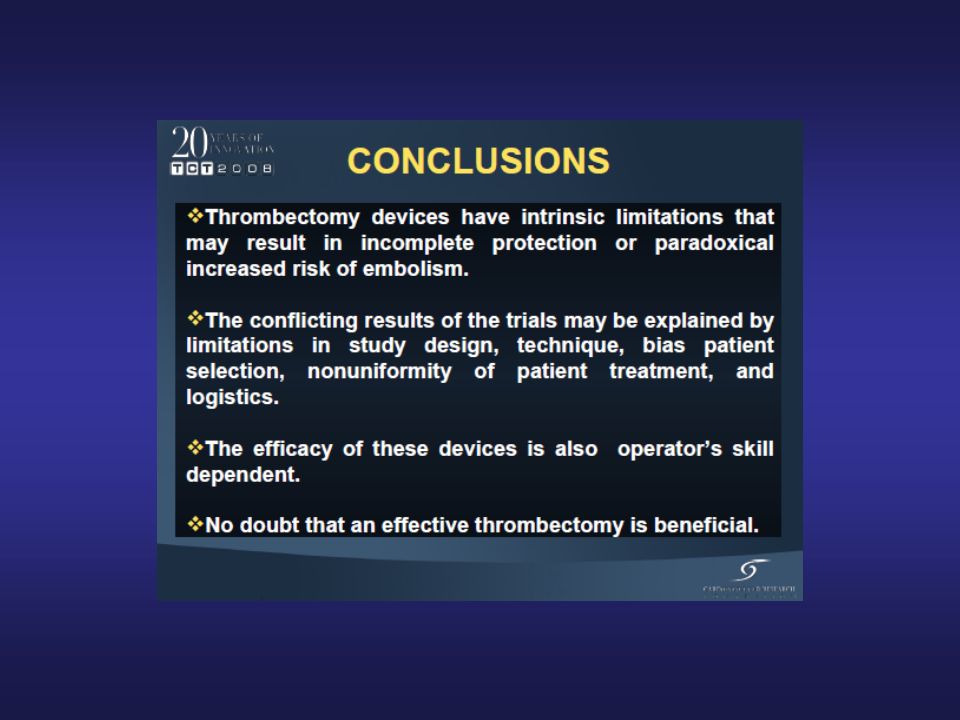
Conclusões : Atualmente classificada como IIa / B – Diretrizes ESC Ausência de estudo comparativo com poder suficiente para avaliar desfecho clínico duro Nos estudos mais representativos a randomização foi feita antes da angiografia Como orientação clínica deve ser fortemente considerada em casos com TTS elevado (3 a 5)
")
39
A patient was considered to have AET if TIMI thrombus grades 2
to 5 were present. In brief, in TIMI thrombus grade 0, no cineangiographic characteristics of thrombus are present; in TIMI thrombus grade 1, possible thrombus is present, with such angiography characteristics as reduced contrast density, haziness, irregular lesion contour, or a smooth convex “meniscus” at the site of total occlusion suggestive but not diagnostic of thrombus; in TIMI thrombus grade 2, there is definite thrombus, with greatest dimensions < ou=1/2 the vessel diameter; in TIMI thrombus grade 3, there is definite thrombus but with greatest linear dimension >1/2 but <2 vessel diameters; in TIMI thrombus grade 4, there is definite thrombus, with the largest dimension >2 vessel diameters; and in TIMI thrombus grade 5, there is total occlusion.

Apresentações semelhantes







:679-84. Long-term Outcomes of Patients with Acute Myocardial Infarction Presenting to Hospitals.>")
>")













