Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Hepatite A: Diagnóstico Epidemiologia e Prevenção
Dra. Vanessa de Paula Fundação Oswaldo Cruz Lab. Desenvolvimento Tecnológico em Virologia FIOCRUZ de Paula, VS. 2011

2
Transmissão parenteral
Os vírus das hepatites Vírus da hepatite A (HAV) Fam. Picornaviridae Transmissão entérica Vírus da hepatite E (HEV) Fam. Hepeviridae Vírus da hepatite B (HBV) Fam. Hepadnaviridae Transmissão parenteral Vírus da hepatite C (HCV) Fam. Flaviviridae Vírus da hepatite D (HDV) “viróide” FIOCRUZ de Paula, VS. 2011
 Fam. Picornaviridae. Transmissão entérica. Vírus da hepatite E (HEV) Fam. Hepeviridae. Vírus da hepatite B (HBV) Fam. Hepadnaviridae. Transmissão parenteral. Vírus da hepatite C (HCV) Fam. Flaviviridae. Vírus da hepatite D (HDV) viróide FIOCRUZ de Paula, VS")
3
Hepatite A FIOCRUZ de Paula, VS. 2011
4
A infecção pelo HAV no mundo
Distribuição mundial Causa mais comum de hepatite viral aguda (1,5 milhão casos/ano) Prevalência de Anti-HAV Maior prevalência em países em desenvolvimento Alta Intermediária Baixa Muito baixa FIOCRUZ de Paula, VS. 2011 16
 Prevalência de Anti-HAV. Maior prevalência em países em desenvolvimento. Alta. Intermediária. Baixa. Muito baixa. FIOCRUZ de Paula, VS")
5
Breve histórico da hepatite A
1973, identificação do HAV (Feinstone et al.) 1979, propagação do HAV em cultura celular (Provost e Hilleman) 1991, licenciada a primeira vacina inativada para hepatite A FIOCRUZ de Paula, VS. 2011
 1979, propagação do HAV em cultura celular (Provost e Hilleman) 1991, licenciada a primeira vacina inativada para hepatite A. FIOCRUZ de Paula, VS")
6
O vírus da hepatite A (HAV)
Classificação: Família Picornaviridae Gênero Hepatovirus Partículas de 27 a 32 nm Não envelopado Simetria icosaédrica FIOCRUZ de Paula, VS. 2011

7
Organização do genoma do HAV
FIOCRUZ de Paula, VS. 2011

8
Ciclo de multiplicação intracelular do HAV
FIOCRUZ de Paula, VS. 2011

9
Propagação do HAV in vitro
Replicação em diversos tipos de cultivos de células de mamíferos Ciclo de multiplicação: lento, baixa produção viral, sem causar CPE Aumento da eficiência de replicação resultante da aquisição de uma série de mutações adaptativas FIOCRUZ de Paula, VS. 2011

10
Fezes contaminadas pelo HAV
Transmissão do HAV Fezes contaminadas pelo HAV mãos esgoto Suprimento de água Ambientes hídricos Frutos do mar homem FIOCRUZ de Paula, VS. 2011

11
Ingestão de material infectado
Patogênese do HAV Ingestão de material infectado Estômago e intestino delgado Circulação portal Replicação hepatócitos bile Circ. sistêmica Intestino Viremia Excreção nas fezes ciclo entero- hepático fonte: Cuthbert, 2001 FIOCRUZ de Paula, VS. 2011 FIOCRUZ-IOC Amado LA, 2010

12
Aspectos clínicos da hepatite A
Período de incubação: Icterícia por grupo etário: < 6 anos 6 – 14 anos > 14 anos Complicações (raras): Cronicidade: média 30 dias (15-50 dias) <10% 40%-50% 70%-80% hepatite fulminante hepatite recorrente hepatite arrastada Não FIOCRUZ de Paula, VS. 2011 7
: Cronicidade: média 30 dias. (15-50 dias) <10% 40%-50% 70%-80% hepatite fulminante hepatite recorrente hepatite arrastada. Não. FIOCRUZ de Paula, VS")
13
Manifestações clínicas
Sintomática Assintomática Anictérica 1 a 2 anos: 85% 3 a 4 anos: 50% Ictérica > 5 anos: 20% Colestática Adolescentes e adultos jovens: 3% a 20% Fulminante 0,5-1% (dos Santos et al., 2009) Fatalidade 12,5% ≥ 60 anos (Canuel et al., 2007) FIOCRUZ de Paula, VS. 2011 FIOCRUZ-IOC Amado LA, 2010
 Fatalidade. 12,5% ≥ 60 anos. (Canuel et al., 2007) FIOCRUZ de Paula, VS FIOCRUZ-IOC Amado LA,")
14
Diagnóstico das hepatites virais
Diagnóstico clínico Pródromo: síndrome gripal, astenia, febre, cefaléia Fase aguda: icterícia, colúria, acolia fecal, náuseas, vômitos, hepatomegalia, dor abdominal 2. Diagnóstico bioquímico Hepatograma (ALT, AST, FA, gama GT) 3. Diagnóstico sorológico Pesquisa de anticorpos e antígenos (EIA) 4. Diagnóstico molecular Pesquisa do genoma viral (hibridização,PCR) 5. Diagnóstico histológico (biópsia hepática) Histopatologia e imunohistoquímica FIOCRUZ de Paula, VS. 2011
 3. Diagnóstico sorológico. Pesquisa de anticorpos e antígenos (EIA) 4. Diagnóstico molecular. Pesquisa do genoma viral (hibridização,PCR) 5. Diagnóstico histológico (biópsia hepática) Histopatologia e imunohistoquímica. FIOCRUZ de Paula, VS")
15
MANIFESTAÇÃO CLÍNICA DO HAV POR FAIXA ETÁRIA
20 40 60 80 100 < 6 6 - 14 > 14 Idade (anos) % Assintomática Sintomática FIOCRUZ-IOC de Paula, VS; 2004 FIOCRUZ de Paula, VS. 2011
 % Assintomática. Sintomática. FIOCRUZ-IOC de Paula, VS; FIOCRUZ de Paula, VS")
16
Hepatite A aguda Cura EVOLUÇÃO CLÍNICA DA INFECÇÃO PELO HAV
Hepatite Colestática Hepatite Fulminante Reincidência Cura 99% Caso Fatal Clinical Outcome of HАV Infection FIOCRUZ de Paula, VS. 2011

17
Curso sorológico Sintomas HAV fecal HAV Log10 semanas HAV fecal
81 dias (>3 meses) PCR tempo real (Tjon et al., 2006) Saliva (Pinto et al.,2002) FIOCRUZ de Paula, VS. 2011 FIOCRUZ-IOC Amado LA, 2010
 PCR tempo real. (Tjon et al., 2006) Saliva. (Pinto et al.,2002) FIOCRUZ de Paula, VS FIOCRUZ-IOC Amado LA,")
18
FIOCRUZ de Paula, VS. 2011
19
Infecção pelo HAV na fase pré-soroconversão
Período de janela virêmico SORONEGATIVO População: 46 Pacientes com hepatite aguda não A-C (CRNHV, 2001) Testes sorológicos (2a amostra soro): anti-HAV IgM e total (Organon) Pesquisa de HAV RNA: RT-PCR FIOCRUZ de Paula, VS. 2011
 Testes sorológicos (2a amostra soro): anti-HAV IgM e total (Organon) Pesquisa de HAV RNA: RT-PCR. FIOCRUZ de Paula, VS")
20
Dados bioquímicos, clínicos e sorológicos dos casos de hepatite A aguda inicialmente categorizada como HNABC (12/46: 26%) 1a coleta 2 a c oleta No. idade ALT (IU/L) HAV RNA Time (dias ) IgM anti - Total 24 12 106 + 21 180 33 13 14 NA 150 11 22 192 193 17 18 168 266 35 20 289 423 447 10 37 23 926 546 19 97 631 3 15 34 - 956 4 31 + - NA NA NA NA 1067 10 NA + 24 888 + + + 1400 15 NA + 20 923 + + + FIOCRUZ de Paula, VS. 2011
 HAV. RNA. Time. (dias. ) IgM. anti. - Total NA NA. NA. NA. NA NA NA FIOCRUZ de Paula, VS")
21
Detecção do HAV-RNA nas Hepatites Agudas NABC
Detecção de HAV RNA em 26% (12/42) dos pacientes com quadro agudo de hepatite NANBNC Importância na pesquisa do HAV RNA no esclarecimento de casos de hepatite aguda de etiologia desconhecida Importância da solicitação de uma segunda amostra nestes casos FIOCRUZ de Paula, VS. 2011
 dos pacientes com quadro agudo de hepatite NANBNC. Importância na pesquisa do HAV RNA no esclarecimento de casos de hepatite aguda de etiologia desconhecida. Importância da solicitação de uma segunda amostra nestes casos. FIOCRUZ de Paula, VS")
22
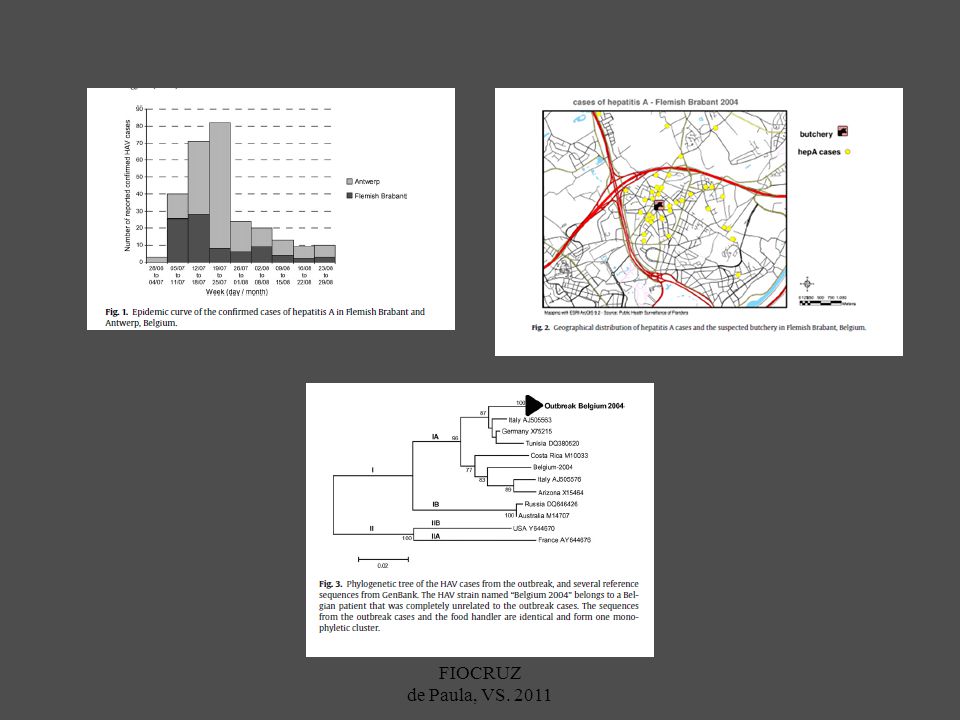
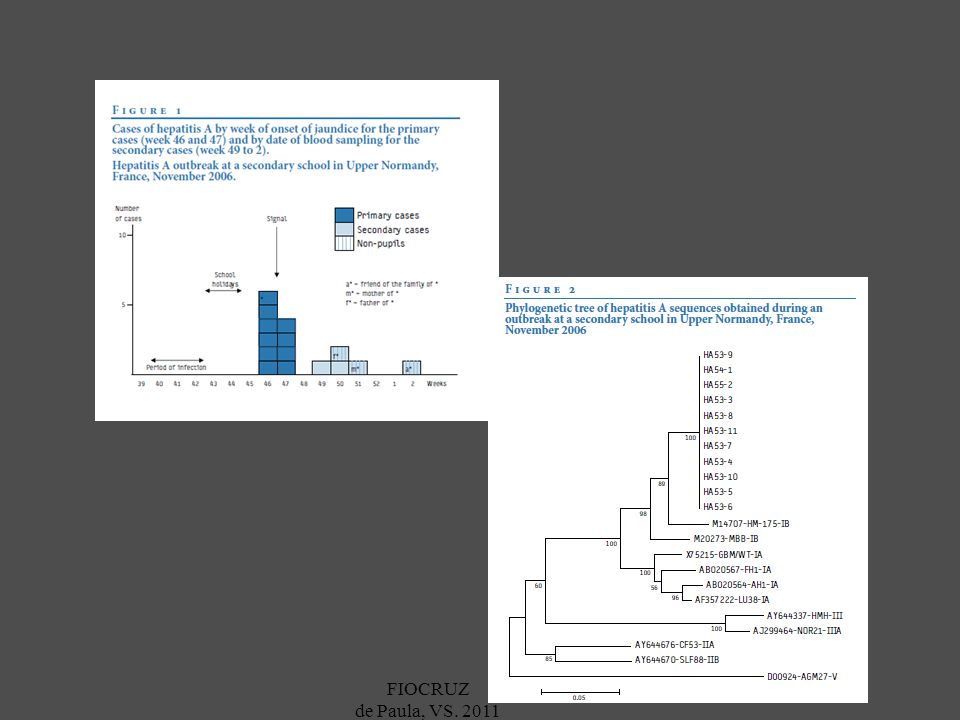
Artigo 8 FIOCRUZ de Paula, VS. 2011
23
FIOCRUZ de Paula, VS. 2011

24
Epidemiologia da Hepatite A
estabilidade da partícula viral eliminação nas fezes, em grandes quantidades, no período de incubação infecção assintomática em crianças Condições sanitárias precárias Ampla disseminação do HAV no ambiente FIOCRUZ de Paula, VS. 2011

25
Padrões globais da transmissão do HAV
Endemicidade Taxa da doença Idade da infecção Modo de transmissão infância alta variável Pessoa-a-pessoa; Surtos incomuns adolescentes/ adultos jovens intermediária Surtos (Água e alimentos) baixa muito baixa adultos Viajantes; surtos incomuns [SLIDE 17, SLIDE 18] Global Patterns of Hepatitis A Virus Transmission, Geographic Distribution of HAV Infection* Worldwide, four different patterns of HAV transmission can be defined on the basis of age-specific seroprevalence data. In general, these transmission patterns correlate with socioeconomic and hygienic conditions. In many developing countries where environmental sanitation generally is poor, nearly all children <9 years of age have evidence of prior HAV infection. In these areas, distinct outbreaks rarely occur and clinical disease related to HAV infection is uncommon. As hygienic conditions improve, transmission shifts to older age groups and the incidence of clinically evident disease increases. In most industrialized countries, low levels of endemic HAV transmission occur. The relatively high prevalence of prior HAV infection among older age groups in these areas is likely to be related to the presence of lower socioeconomic and hygienic conditions in the past. Because most of the population is susceptible to HAV infection, disease outbreaks are relatively common in most of these countries. However, in a few industrialized countries hepatitis A outbreaks are uncommon, and nearly all HAV transmission occurs among drug users and travelers to high endemic areas. *(Note: The map of anti-HAV prevalence generalizes available data and patterns may vary within countries.) FIOCRUZ de Paula, VS. 2011
 baixa. muito baixa. adultos. Viajantes; surtos. incomuns. [SLIDE 17, SLIDE 18] Global Patterns of Hepatitis A Virus Transmission, Geographic Distribution of HAV Infection* Worldwide, four different patterns of HAV transmission can be defined on the basis of age-specific seroprevalence data. In general, these transmission patterns correlate with socioeconomic and hygienic conditions. In many developing countries where environmental sanitation generally is poor, nearly all children <9 years of age have evidence of prior HAV infection. In these areas, distinct outbreaks rarely occur and clinical disease related to HAV infection is uncommon. As hygienic conditions improve, transmission shifts to older age groups and the incidence of clinically evident disease increases. In most industrialized countries, low levels of endemic HAV transmission occur. The relatively high prevalence of prior HAV infection among older age groups in these areas is likely to be related to the presence of lower socioeconomic and hygienic conditions in the past. Because most of the population is susceptible to HAV infection, disease outbreaks are relatively common in most of these countries. However, in a few industrialized countries hepatitis A outbreaks are uncommon, and nearly all HAV transmission occurs among drug users and travelers to high endemic areas. *(Note: The map of anti-HAV prevalence generalizes available data and patterns may vary within countries.) FIOCRUZ de Paula, VS")
26
Distribuição geográfica da infecção pelo HAV
Prevalência de Anti-HAV Alta Intermediária Baixa Muito baixa FIOCRUZ de Paula, VS. 2011 (CDC, 1999) 16
 16.")
27
O impacto das melhorias sócio-econômicas na prevalência da infecção pelo HAV
[SLIDE 17, SLIDE 18] Global Patterns of Hepatitis A Virus Transmission, Geographic Distribution of HAV Infection* Worldwide, four different patterns of HAV transmission can be defined on the basis of age-specific seroprevalence data. In general, these transmission patterns correlate with socioeconomic and hygienic conditions. In many developing countries where environmental sanitation generally is poor, nearly all children <9 years of age have evidence of prior HAV infection. In these areas, distinct outbreaks rarely occur and clinical disease related to HAV infection is uncommon. As hygienic conditions improve, transmission shifts to older age groups and the incidence of clinically evident disease increases. In most industrialized countries, low levels of endemic HAV transmission occur. The relatively high prevalence of prior HAV infection among older age groups in these areas is likely to be related to the presence of lower socioeconomic and hygienic conditions in the past. Because most of the population is susceptible to HAV infection, disease outbreaks are relatively common in most of these countries. However, in a few industrialized countries hepatitis A outbreaks are uncommon, and nearly all HAV transmission occurs among drug users and travelers to high endemic areas. *(Note: The map of anti-HAV prevalence generalizes available data and patterns may vary within countries.) FIOCRUZ de Paula, VS. 2011 (CDC, 2006)
 FIOCRUZ de Paula, VS (CDC, 2006)")
28
Genótipos do HAV I A e IB II A e IIB Humanas IIIA e IIIB
Costa-Matiolli et al., 2002: VP1 inteira (900 nts), sugere a classificação do HAV em 6 genótipos. Lu et al., 2004: seqüência completa das cepas CF53 (II) e SLF88 (VII): confirmaram a existência de 6 genótipos do HAV. Um único sorotipo I A e IB II A e IIB IIIA e IIIB IV, V, VI: Símias Humanas Fonte: Lu et al., 2004 FIOCRUZ de Paula, VS. 2011 FIOCRUZ-IOC Amado LA, 2010
, sugere a classificação do HAV em 6 genótipos. Lu et al., 2004: seqüência completa das cepas CF53 (II) e SLF88 (VII): confirmaram a existência de 6 genótipos do HAV. Um único sorotipo. I A e IB. II A e IIB. IIIA e IIIB. IV, V, VI: Símias. Humanas. Fonte: Lu et al., FIOCRUZ de Paula, VS FIOCRUZ-IOC Amado LA,")
29
Distribuição geográfica dos genótipos do HAV
IA IA III IB IA III IB IA IB * IA IA * IB IA * * II III IA IA IB IB IA Fonte: Nainan et al., 2006 Genótipos do HAV IA IB II III * Co-circulação de múltiplos genótipos do HAV: Brasil, França, África Sul, Israel, India FIOCRUZ de Paula, VS. 2011

30
FIOCRUZ de Paula, VS. 2011
31
FIOCRUZ de Paula, VS. 2011
32
FIOCRUZ de Paula, VS. 2011
33
FIOCRUZ de Paula, VS. 2011
34
FIOCRUZ de Paula, VS. 2011
35
FIOCRUZ de Paula, VS. 2011
36
Prevenção e controle da hepatite A
Saneamento básico Higiene Imunoglobulina Vacina Altamente imunogênicas Eficácia pré- e pós-exposição Proteção contra todas as amostras de HAV (1 sorotipo) FIOCRUZ de Paula, VS. 2011
 FIOCRUZ de Paula, VS")
37
Controle da hepatite A em alguns países industrializados - EUA
Recomendações do Comitê de Práticas de Imunização/ACIP para prevenção da hepatite A pela vacinação (1999) Grupos de risco (a partir de 1996) Viajantes para áreas endêmicas Homosexuais masculinos IVDUs Pessoas com hepatopatias crônicas Imunização infantil universal em comunidades com altas taxas de hepatite A ( 20 casos/ habitantes, 1987/1997) FIOCRUZ de Paula, VS. 2011
 Grupos de risco (a partir de 1996) Viajantes para áreas endêmicas. Homosexuais masculinos. IVDUs. Pessoas com hepatopatias crônicas. Imunização infantil universal em comunidades com altas taxas de hepatite A ( 20 casos/ habitantes, 1987/1997) FIOCRUZ de Paula, VS")
38
Incidência da hepatite A nos EUA
> = 20 5 - 9 0 - 4 Taxa por 100,000 2002 [SLIDE 15] Hepatitis A Incidence, United States The decline of hepatitis A in these three regions may be summarized as follows. At baseline, prior to the ACIP recommendations of 1999, the high incidence states had an average rate of 25.9 cases per 100,000 and declined in 2001 to 4.5 cases per 100,000. In intermediate incidence states there was a decline from 16.1 to 3.8 cases per 100,000. In low incidence states there was a smaller decline from 5.6 to 3.4 cases per 100,000. The change in incidence from the baseline period to 2001 can be seen in this state and county map of the United States. From 1987 to 1997 there were many counties particularly in the West with rates averaging 10 or more cases per 100,000, shown in red and orange. By 2001 there were few counties with rates at this level. The decline in national rates is a reflection of declines in high and intermediate incidence states as shown in this slide. In summary, the incidence of hepatitis A declined to its lowest recorded level by Incidence declines have been greatest in the high and intermediate incidence states where the rate in children is approaching that of adults and where the majority of pediatric vaccine has been distributed. Cases from low incidence states now account for the majority of cases nationwide. A limitation of this analysis is that we relied on public sector vaccine doses purchased because currently we do not have vaccine coverage data. At this time, it is difficult to separate the impact of vaccination from temporal trends because of the cyclic variation in hepatitis A incidence. These findings suggest that implementation of the ACIP strategy is reducing the overall incidence of hepatitis A in the U.S.. The decline in rate observed among adults may in part be attributed to vaccination of children. FIOCRUZ de Paula, VS. 2011

39
Ministerio de Salud de la Nacion 2005-06-18 B.O. 17/06/05
SALUD PUBLICA Resolución 653/2005 – MSA Argentina - Incorpórase al Programa Nacional de Inmunizaciones la vacunación con una dosis contra la hepatitis A, con carácter de gratuito y obligatorio, e intégrase la misma al Calendario Nacional de Vacunación. FIOCRUZ de Paula, VS. 2011

40
Fuente: Elaboración UNAMOS en base a datos del SNVS
Tasas de notificación de hepatitis A y sin especificar por cada habitantes según grupos de edad. Argentina hasta la semana epidemiológica 41 de 2009. Fuente: Elaboración UNAMOS en base a datos del SNVS Morbilidad El principal grupo afectado es el de 5 a 9 años con 173 casos y una tasa de 0,52 casos por habitantes. FIOCRUZ de Paula, VS. 2011

41
ACIP - Recomendações provisórias (Outubro de 2005)
Todas as crianças devem ser vacinadas para hepatite A com 1 ano de idade (12 a 24 meses) [SLIDE 12] Hepatitis A Vaccination Strategy: Epidemiologic Considerations Epidemiologic features of HAV infection that need to be considered in developing hepatitis A vaccination strategies include the following: Most hepatitis A in the United States occur in the context of extended community-wide outbreaks in which a large proportion of cases have no identifiable risk factor. In these outbreaks, the highest rates of disease occur among children 5-14 years of age and person-to-person transmission, especially from children to adults, is the primary mode of transmission. 2. The primary groups with an increased risk of infection include the following: Travelers to developing countries. The risk among such travelers who do not receive IG is about 3-5/1000 per month of stay. These persons should be vaccinated before departure. Persons can be assumed to be protected by 4 weeks after receiving the initial vaccine dose, although the second dose 6 to 18 months later is necessary for long‑term protection. Individuals who will travel to high‑risk areas <4 weeks after the initial dose of vaccine should also be given IG, but at different injection sites. Travelers to high‑risk areas who are allergic to a vaccine component or otherwise elect not to receive vaccine or children less than 2 years old should receive IG. Men who have sex with men. Hepatitis A outbreaks among MSM have been reported frequently and serosurveys have demonstrated a prevalence of HAV infection among MSM several-fold higher than among control populations. Illegal drug users. Cross-sectional serologic surveys have demonstrated that IDUs have higher anti-HAV seropositivity that the general US population. Transmission among IDUs likely occurs through percutaneous and fecal-oral routes, e.g., sharing needles, sharing contaminated “works” and having household or other close personal contact with infected persons. Persons with chronic liver disease. Susceptible persons with chronic liver disease, including persons awaiting or having received liver transplants, may be at increased risk for complications of hepatitis A and should be vaccinated. FIOCRUZ de Paula, VS. 2011
 [SLIDE 12] Hepatitis A Vaccination Strategy: Epidemiologic Considerations. Epidemiologic features of HAV infection that need to be considered in developing hepatitis A vaccination strategies include the following: Most hepatitis A in the United States occur in the context of extended community-wide outbreaks in which a large proportion of cases have no identifiable risk factor. In these outbreaks, the highest rates of disease occur among children 5-14 years of age and person-to-person transmission, especially from children to adults, is the primary mode of transmission. 2. The primary groups with an increased risk of infection include the following: Travelers to developing countries. The risk among such travelers who do not receive IG is about 3-5/1000 per month of stay. These persons should be vaccinated before departure. Persons can be assumed to be protected by 4 weeks after receiving the initial vaccine dose, although the second dose 6 to 18 months later is necessary for long‑term protection. Individuals who will travel to high‑risk areas <4 weeks after the initial dose of vaccine should also be given IG, but at different injection sites. Travelers to high‑risk areas who are allergic to a vaccine component or otherwise elect not to receive vaccine or children less than 2 years old should receive IG. Men who have sex with men. Hepatitis A outbreaks among MSM have been reported frequently and serosurveys have demonstrated a prevalence of HAV infection among MSM several-fold higher than among control populations. Illegal drug users. Cross-sectional serologic surveys have demonstrated that IDUs have higher anti-HAV seropositivity that the general US population. Transmission among IDUs likely occurs through percutaneous and fecal-oral routes, e.g., sharing needles, sharing contaminated works and having household or other close personal contact with infected persons. Persons with chronic liver disease. Susceptible persons with chronic liver disease, including persons awaiting or having received liver transplants, may be at increased risk for complications of hepatitis A and should be vaccinated. FIOCRUZ de Paula, VS")
42
FIOCRUZ de Paula, VS. 2011
Apresentações semelhantes







 REDUZIR RISCO DE TRANSMISSÃO>")





>")





