Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Prevenção do câncer do T.G.I.
Dra. Marcia Fuzaro Terra Cardial Departamento de Ginecologia e Obstetrícia da FMABC Setor de PTGI e Colposcopia Diretora da SOGESP e ABG- SP

2
CARCINOMA DO COLO UTERINO
HISTÓRICO 1880 – Abordagem cirúrgica do câncer de colo -50% de mortalidade. Wertheim e Schauta desenvolvem técnica cirúrgica radical radioterapia substitui a cirurgia-persistem complicações

3
CARCINOMA DO COLO UTERINO
HISTÓRICO ESTUDANDO EM COBAIAS DESENVOLVE CITOLOGIA HORMONAL. COMPARA ESTUDO EM HUMANOS -1954-PUBLICA “ ATLAS DE CITOLOGIA EXFOLIATIVA” GEORGE PAPANICOLAOU ( ) E ANDROMACHE
 E ANDROMACHE.")
4
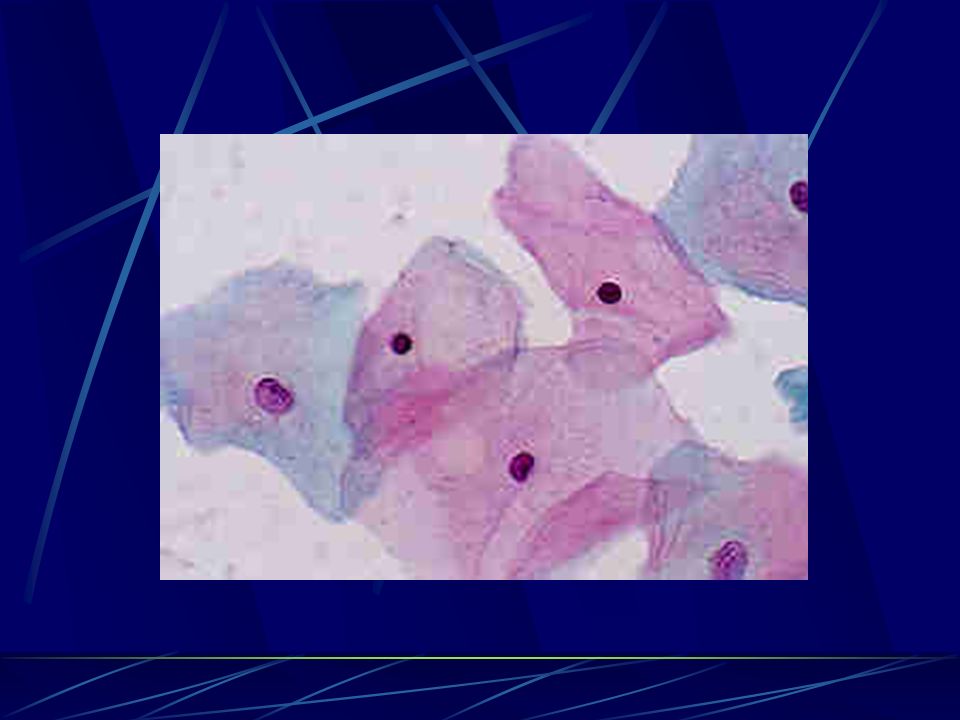
Citologia Colheita: fundo de saco,paredes vaginais, ecto e endocérvice
Informação ao citologista sobre a idade, tempo de menopausa e uso ou não de TRH Fixação Preparo para a colheita

5
TÉCNICA DO EXAME 48 horas antes do exame , evitar: Relações sexuais
Duchas vaginais Cremes vaginais

6
TÉCNICA DO EXAME CITOLOGIA
1947 – Ayre (Canadá) introduz espátula para citologia
 introduz espátula para citologia.")
7
TÉCNICA DO EXAME COLETA DOS FORNICES VAGINAIS E VAGINA

8
TÉCNICA DO EXAME COLETA ECTOCERVICAL JUNÇÃO ESCAMO-COLUNAR

9
TÉCNICA DO EXAME COLETA ENDOCERVICAL

10
TÉCNICA DO EXAME V ECT END

11
TÉCNICA DO EXAME Fixação com álcool absoluto ou Carbovax ( spray)
")
12
TÉCNICA DO EXAME Aplicação da solução de lugol (Schiller)
")
13
BETHESDA Dezembro, Workshop com finalidade de termologia diagnostica uniforme, para facilitar a comunicação entre o patologista e o clínico Inclui Diagnóstico descritivo Avalia se o espécime é adequado Adequação do espécime Esfregaço satisfatório Esfregaço satisfatório mas limitado por ... Esfregaço não satisfatório para avaliação

14
Papanicolaou - Bethesda
Ausência de alter. Reativa-reparativa LIE - BG(lesão intra-epitelial escamosa de baixo grau) LIE –AG(lesão intra-epitelial escamosa de alto grau Classe I –normal Classe II –Inflamat. Classe II-HPV } Classe III-suspeita III A- D.leve (NICI) III B- D. moderada (NICII) } IIIC- D.grave (NICIII) } Classe IV- Ca ”in situ” (NICIII) }
 LIE –AG(lesão intra-epitelial escamosa de alto grau. Classe I –normal. Classe II –Inflamat. Classe II-HPV } Classe III-suspeita. III A- D.leve (NICI) III B- D. moderada. (NICII) } IIIC- D.grave (NICIII) } Classe IV- Ca in situ (NICIII) }")
16
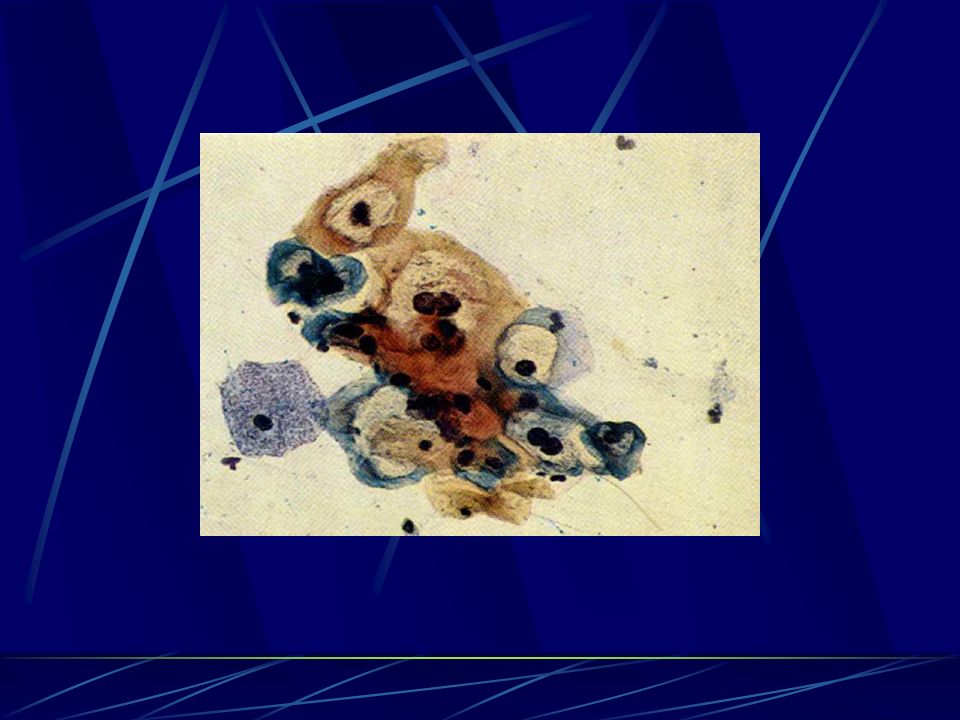
Reativa-Reparativa

18
LIE - Baixo Grau

19
História Natural do Câncer de Colo do Útero e Lesões Precursoras
( RICHART & BARRON – 1969) 10 anos 7 anos Ca invasor Reativo NIC I NIC III
 10 anos. 7 anos. Ca invasor. Reativo. NIC I. NIC III.")
20
LIE de alto grau – NIC III

21
LIE alto grau – tipo sincício

22
Carcinoma de Células escamosas
Classe V

23
BETHESDA 2001 Classificar Atypical Squamous Cells (ASC) como “Significado Indeterminado (ASC-US)” ou “Impossibilidade de Excluir HSIL (ASC-H)” Nos casos de diagnostico de ASC com limitação de interpretação por fatores tecnicos, o mesmo deve ser referido no laudo. ASC não deve exceder 5% do total das citologias com taxa de ASC:SIL inferior a 2:1 ou 3:1 em rastreamentos na população geral.

24
Inflamatória ASC US /ASC-H AGC NIC I Displasia leve LIE de baixo grau
CLASSES Papanicolaou 1954 DESCRIÇÃO GRADAÇÃO NIC Richart 1969 SISTEMA BETHESDA 1988 I Normal II Inflamatória Atipia Reativa/Reparativa Displasia acentuada LIE de alto grau (HSIL)ou(LIEAG) IV Carcinoma in situ V Câncer invasivo ASC US /ASC-H AGC Displasia leve NIC I LIE de baixo grau (LSIL)ou(LIEBG) Displasia moderada I I I NIC II 10 anos NIC III
ou(LIEAG) IV. Carcinoma in situ. V. Câncer invasivo. ASC US /ASC-H. AGC. Displasia leve. NIC I. LIE de baixo grau. (LSIL)ou(LIEBG) Displasia moderada. I I I. NIC II. 10 anos. NIC III.")
25
Aspectos Citológicos na Mulher Climatérica
Climatério sem TH e sem preparo : Cuidado com sinais de hiper-estrogenismo ! Hipoestrogenismo: cuidado com Falso positivo citológico (ASC-US, ASC-H, LIE BG por descamação de células basais e para-basais)
")
26
ASC-US Atrofia

27
BETHESDA 2001 Classificar Atypical Glandular Cells (AGC)
")
28
AGC

29
AGU - AIS

30
CARCINOMA SEROSO PAPILAR DE OVÁRIO

31
Pesquisa de DNA HPV Hibridização “in situ” PCR Captura híbrida

32
Diagnóstico do HPV Biologia Molecular PCR

33
Detecção de HPV por Captura Híbrida
1. Desnaturação do Espécime 2. Hibridização com sonda de RNA 3. Captura de Híbridos 4. Reação com o conjugado 5. Amplificação do sinal dos Híbridos por Quimioluminescência

34
O teste DNA-HPV deve ser utilizado em duas situações:
FDA aprovou recentemente o teste DNA HPV em associação com citologia em mulheres com idade superior a 30 anos. Orienta não realizar em idade inferior a esta, pois é mais freqüente haver DNA HPV, porém é transitório portanto o resultado pode não ser significante podendo trazer mais confusão que benefícios. - O teste DNA HPV é ainda usado em citologias levemente anormais para determinar se mais testes ou tratamento serão necessários. A C S

35
Alterações citológicas e colposcópicas
ASC-US –repetir exame em 6 meses,com reposição estrogênica ASC- H – Colposcopia imediata AGC –pesquisar canal endocervical, endométrio, ovário realizar US transvaginal

36
Alterações colposcópicas
Epitelio aceto branco Mosaico Pontilhado Vasos atípicos Área iodo-negativa Queratose( Miscelânia)
")
37
Colposcopia

38
Colposcopia – Teste de Schiller

39
Diagnóstico Histopatológico

44
LIE Baixo grau –NIC I Conduta expectante Conduta excisional
se persistir por dois anos

45
LIE Alto grau Conização: Fria- se suspeita de invasão ou AGC
CAF –atenção a canal Cone laser

47
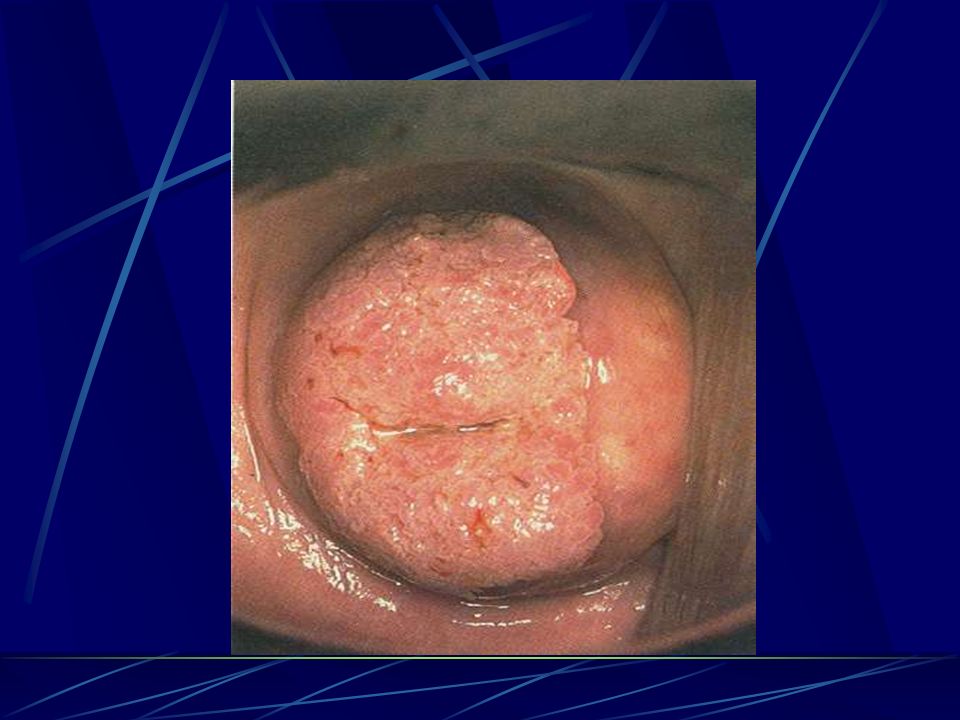
PREVENÇÃO DO CÂNCER DE COLO

48
HPV Causa câncer ????

49
Solo Semente Condições

50
Solo ZT –célula metaplásica Microfissuras

51
Semente HPV Baixo Risco e Alto Risco Vírus DNA 8000 nucleotídeos
Semente HPV Baixo Risco e Alto Risco Vírus DNA 8000 nucleotídeos Genoma circular

52
HPV HPV S S - Genoma - Oncogênese LCR (Forma Episomal) LCR
( Forma Integrada)
")
53
HPV o Vírus >100 tipos identificados2 ~30 afetam a genitalia2,3
~15 ALTO RISCO*,2,3, Os tipos de HPV 16 e 18 presentes na maioria dos cânceres cervico-uterinos em todo o mundo.4 Tipos BAIXO RISCO** HPV 6 e 11 associados com maior freqüência com verrugas genitais externas.3 1.Howley PM, Lowy DR. En: Knipe DM, Howley PM, eds. Philadelphia, Pa: Lippincott-Raven; 2001:2197–2229. 2. Schiffman M, Castle PE. Arch Pathol Lab Med. 2003;127:930– Wiley DJ, Douglas J, Beutner K, y cols. Clin Infect Dis. 2002;35 (suppl 2):S210–S Muñoz N, Bosch FX, Castellsagué X, y cols. Int J Cancer.2004;111:278–285.
:S210–S Muñoz N, Bosch FX, Castellsagué X, y cols. Int J Cancer.2004;111:278–285.")
54
Penetração da semente no solo
Inoculação(Fase 0): Microtrauma- vírions na camada basal, atravessam a membrana citoplasmática
: Microtrauma- vírions na camada basal, atravessam a membrana citoplasmática.")
55
Spectrum of Changes in Cervical Squamous Epithelium Caused by HPV Infection
Normal Cervix HPV Infection/ CIN* 1 CIN 2 / CIN 3 / Cervical Cancer Key Point Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is linked to the activity of E6 and E7 proteins.2 Background In benign HPV-associated skin lesions, the HPV virus maintains its genome as episomes at low copy numbers (10–200 copies/cell) in the basal cells of the epithelium separate from the host cell DNA. To maintain its viral DNA as an episome, viral E1 and E2 proteins are expressed. Failure to express E1 leads to the integration of the HPV genome into the host cell chromosome.3 Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is considered an important step in tumor progression.2 In malignant HPV-associated skin lesions, HPV DNA integration into the host cell’s chromosome regularly occurs through a break in the viral genome around the E1/E2 region. Integration-mediated disruption of E2 may trigger uncontrolled expression of E6 and E7, resulting in cellular transformation.2 The E6 protein associates with the tumor suppressor protein p53 and promotes proteolytic destruction of the protein. This leads to malignant transformation and loss of regulated cell growth. The E7 protein associates with the retinoblastoma protein (pRB), which inactivates the cell cycle restriction function of this protein.2 References 1. Gallo G, Bibbo M, Bagella L, et al. Study of viral integration of HPV-16 in young patients with LSIL. J Clin Pathol. 2003;56:532–536. 2. Syrjänen KJ, Syrjänen SM. Molecular biology of papillomaviruses. In: Papillomavirus Infections in Human Pathology. Chichester, United Kingdom: John Wiley & Sons, Inc.; 2000:11–51. 3. Doorbar J. The papillomavirus life cycle. J Clin Virol. 2005;32(suppl):S7–S15. *CIN = cervical intraepithelial neoplasia Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564.
 in the basal cells of the epithelium separate from the host cell DNA. To maintain its viral DNA as an episome, viral E1 and E2 proteins are expressed. Failure to express E1 leads to the integration of the HPV genome into the host cell chromosome.3. Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is considered an important step in tumor progression.2 In malignant HPV-associated skin lesions, HPV DNA integration into the host cell’s chromosome regularly occurs through a break in the viral genome around the E1/E2 region. Integration-mediated disruption of E2 may trigger uncontrolled expression of E6 and E7, resulting in cellular transformation.2. The E6 protein associates with the tumor suppressor protein p53 and promotes proteolytic destruction of the protein. This leads to malignant transformation and loss of regulated cell growth. The E7 protein associates with the retinoblastoma protein (pRB), which inactivates the cell cycle restriction function of this protein.2. References. 1. Gallo G, Bibbo M, Bagella L, et al. Study of viral integration of HPV-16 in young patients with LSIL. J Clin Pathol. 2003;56:532– Syrjänen KJ, Syrjänen SM. Molecular biology of papillomaviruses. In: Papillomavirus Infections in Human Pathology. Chichester, United Kingdom: John Wiley & Sons, Inc.; 2000:11– Doorbar J. The papillomavirus life cycle. J Clin Virol. 2005;32(suppl):S7–S15. *CIN = cervical intraepithelial neoplasia. Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564.")
56
Penetração da semente no solo
Período de incubação (fase 1): 15 d - 8 m Fase Precoce (fase 2): início da resposta imune adquirida – regressão ou f. expressão ativa Fase Tardia (fase 3): remissão ou recidiva
: 15 d - 8 m. Fase Precoce (fase 2): início da resposta imune adquirida – regressão ou f. expressão ativa. Fase Tardia (fase 3): remissão ou recidiva.")
57
Oncogênese HPV - Infecção - - Produtiva - Transformante

58
- Infecção Transformante - Integração no genoma da cél. hospedeira
Oncogênese HPV - Infecção Transformante - NCII III M.I. Ca Invasor Cofatores Infecção Produtiva Integração no genoma da cél. hospedeira

59
This diagram was developed several years ago to explain the natural history of HPV infections to clinicians. The first step in infection is the initial infection with HPV.

60
INFECÇÃO POR HPV E SISTEMA IMUNE
Eliminação do HPV % HPV(-) após teste (+) Estudos atuais revelam que existe eliminação espontânea do vírus, através da ativação do sistema imune, em mais de 90% dos indivíduos infectados no período de 24 meses. Ambas as infecções por HPV de baixo e alto risco podem regredir espontaneamente sugerindo que o sistema imune responde aos dois grupos de vírus. Em uma pequena minoria, a infecção pelo HPV torna-se persistente levando à neoplasia e câncer genital. Estes dados sugerem que algumas pessoas estabelecem controle imunológico apropriado após infecção ou expressão da doença, enquanto outras falham em estabelecer ou expressar imunidade efetiva. Ho et al. NEJM 328:423-8, 1998.
 após teste (+) Estudos atuais revelam que existe eliminação espontânea do vírus, através da ativação do sistema imune, em mais de 90% dos indivíduos infectados no período de 24 meses. Ambas as infecções por HPV de baixo e alto risco podem regredir espontaneamente sugerindo que o sistema imune responde aos dois grupos de vírus. Em uma pequena minoria, a infecção pelo HPV torna-se persistente levando à neoplasia e câncer genital. Estes dados sugerem que algumas pessoas estabelecem controle imunológico apropriado após infecção ou expressão da doença, enquanto outras falham em estabelecer ou expressar imunidade efetiva. Ho et al. NEJM 328:423-8,")
61
INFECÇAO HPV Alto Risco Alta Carga viral Integrada Persistente
Oncogênese Alto Risco Alta Carga viral Integrada Persistente Permissividade celular Condições imunológicas/ genéticas propícias -

62
HPV tipo não ononcogênico
Estimativa mundial do diagnóstico relatado do HPV Foco em Doença Cervical e Verruga Genital 1/Parkin/ p. 91/col 2/¶4 Câncer Cervical : milhões em20021 2/WHO/ p. 6/¶2 LIE- AG: 10 milhões2 LIE-BG: 30 milhões2 3/WHO/ p. 1/¶2 2/WHO/ p. 6/¶2 Verruga Genital: 30milhões3 HPV tipo oncogênico Infecção por HPV sem amormalidades citológicas detectáveis: 300 milhões2 HPV tipo não ononcogênico Key Points HPV infection is very common, but, in the majority of cases, has no clinical significance. Of all HPV-related conditions, cervical cancer is the most serious manifestation of the virus. However, most HPV-related morbidity is associated with cervical dysplasia or genital warts. Cervical dysplasia is caused by both oncogenic and non-oncogenic types, and genital warts by non-oncogenic types. Background According to estimates from the World Health Organization, worldwide annual incidence of HPV infection and low- and high-grade dysplasia is 300 million, 30 million, and 10 million cases, respectively.1 The World Health Organization estimates that 30 million cases of genital warts occur every year.2 The largest number of cases of cervical HPV infection have no detectable cytologic abnormalities, and many of these are self-limited. However, an important subset will subsequently become associated with disease.1 HPV infection with oncogenic types, notably types 16 and 18, is associated with both low-grade and high-grade cervical lesions. HPV infection with these types can lead to cervical cancer.3 Nononcogenic HPV types, notably types 6 and 11, are associated with low-grade cervical lesions and with anogenital warts.3,4 In a study by Gissmann and colleagues (N=63), HPV 6 and 11 DNA was detected in >90% of anogenital warts.5 References 1. World Health Organization. The current status of development of prophylactic vaccines against human papillomavirus infection. Report of a technical meeting, 16–18 February Geneva, Switzerland: World Health Organization; 1999:1–22. 2. World Health Organization. Sexually transmitted infections increasing–250 million new infections annually. WHO Office of Information. WHO Features. 1990;152:1–6. 3. Burd EM. Human papillomavirus and cervical cancer. Clin Microbiol Rev. 2003;16:1–17. 4. Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clin Infect Dis. 2002;35(suppl 2):S210–S224. 5. Gissmann L, Wolnik L, Ikenberg H, Koldovsky U, Schnurch HG, zur Hausen H. Human papillomavirus types 6 and 11 DNA sequences in genital and laryngeal papillomas and in some cervical cancers. Proc Natl Acad Sci USA. 1983;80:560–563. 1/WHO/ p. 6/¶2 2/WHO/ p. 1/¶2 1/WHO/ p. 6/¶2 1. Parkin DM, Bray F, Ferlay J, Pisani P. CA Cancer J Clin. 2005;55:74– World Health Organization. Geneva, Switzerland: World Health Organization; 1999:1– World Health Organization. WHO Office of Information. WHO Features. 1990;152:1–6. 3/Burd/p. 2/ Table 1. 4/Wiley/p. S210/col 2/¶1. 5/Gissmann/p. 561/Table 2.
, HPV 6 and 11 DNA was detected in >90% of anogenital warts.5. References. 1. World Health Organization. The current status of development of prophylactic vaccines against human papillomavirus infection. Report of a technical meeting, 16–18 February Geneva, Switzerland: World Health Organization; 1999:1– World Health Organization. Sexually transmitted infections increasing–250 million new infections annually. WHO Office of Information. WHO Features. 1990;152:1–6. 3. Burd EM. Human papillomavirus and cervical cancer. Clin Microbiol Rev. 2003;16:1– Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clin Infect Dis. 2002;35(suppl 2):S210–S Gissmann L, Wolnik L, Ikenberg H, Koldovsky U, Schnurch HG, zur Hausen H. Human papillomavirus types 6 and 11 DNA sequences in genital and laryngeal papillomas and in some cervical cancers. Proc Natl Acad Sci USA. 1983;80:560–563. 1/WHO/ p. 6/¶2. 2/WHO/ p. 1/¶2. 1/WHO/ p. 6/¶2. 1. Parkin DM, Bray F, Ferlay J, Pisani P. CA Cancer J Clin. 2005;55:74– World Health Organization. Geneva, Switzerland: World Health Organization; 1999:1– World Health Organization. WHO Office of Information. WHO Features. 1990;152:1–6. 3/Burd/p. 2/ Table 1. 4/Wiley/p. S210/col 2/¶1. 5/Gissmann/p. 561/Table 2.")
63
Mecanismos de prevenção
Secundária: -Citologia - Colposcopia - Histopatologia - DNA HPV Primária : Vacina contra o HPV

64
This approach to cervical cancer prevention has been highly successful
This approach to cervical cancer prevention has been highly successful. In the 1950’s prior to widespread screening using the Pap test the incidence of invasive cervical cancer in the US was between 35 and 40 cases per 100,000 women annually. By 1990 the incidence of invasive cervical cancer had been reduces approximately 75% to about 10 cases per 100,000 women. This is the major success story of cancer prevention.

65
HPV Genotype (%) in cancer of cervix in World
53,5% 70,7% 77,4% 80,3% HPV types 53,5 2,3 2,2 1,4 1,3 1,2 1,0 0,7 0,6 0,5 0,3 4,4 2,.6 17,2 6,7 2,9 10 20 30 40 50 60 70 80 90 100 X Outros 82 73 68 39 51 56 59 35 58 52 33 31 45 18 16 MUÑOZ N et al. Int J Cancer; 111: 278–85, 2004.

66
HPV Vaccine Gardasil ® Merk Sharp Dome (HPV 6,11,16,18) 0,2 , 6 month
Cervarix ® Glaxo Smith Kline (HPV 16,18,31,45) 0, 1 , 6 month
 0, 1 , 6 month.")
67
CERVARIX - Vacina GSK VLPs dos HPVs 16 e 18 no substrato celular de Spodoptera frugipera Sf-9 e Trichoplusia ni Hi-5. Vacina bivalente com volume de 0,5mL contém: 20 μg de cada um dos VLPs de HPV 16 e 18 associados ao adjuvante AS04 : 500 μg hidróxido de alumínio 50 μg de 3-desacilato monofosforil lipídio A. Efeitos Adversos leves como dor local, edema e eritema (~placebo) e sintomas gerais : fadiga, queixas gastrintestinais, prurido e erupções.
 e sintomas gerais : fadiga, queixas gastrintestinais, prurido e erupções.")
68
Vacina contra HPV oncogênico
Morfologicamente idênticos aos vírus intactos Proteína L1 recombinante Não infectantes (não contém material genético, não replicam) Produzida em baculovírus Auto-arranjo em estrutura espacial Composição: 20 µg L1 HPV-16 20 µg L1 HPV- 18 500 µg Al(OH)3 50 µg MPL AS 04 HARPER, DM et al. The Lancet, 367: , 2006.
 Produzida em baculovírus. Auto-arranjo em estrutura espacial. Composição: 20 µg L1 HPV µg L1 HPV µg Al(OH)3. 50 µg MPL. AS 04. HARPER, DM et al. The Lancet, 367: ,")
69
GARDASIL™ Merck’s Quadrivalent HPV L1 VLP Vaccine1
1/Villa/p. 271/abstract. Tipos 6, 11, 16, 18) L1 VLP VLPs em Saccharomyces cerevisiae Aluminum adjuvante 225 μg por dose - 20μg de HPV-6, 40 μg de HPV-11 40 μg de HPV 16 20 μg de HPV-18 0.5 mL volume 3 doses em 6 meses 1/Villa/p. 272 /col 1/¶3. 1/Villa/p. 272 /col 1/¶4. 1/Villa/p. 272 /col 2/¶2. 1/Villa/p. 272 /col 2/¶2. Key Point GARDASIL™ is Merck’s quadrivalent HPV L1 VLP vaccine. It is produced in recombinant yeast, like the hepatitis B vaccine, and adsorbed on a proprietary aluminum adjuvant, like the tetanus vaccine. Background Merck’s quadrivalent vaccine has the advantage that it targets 4 HPV types (6, 11, 16 and 18).1 Together, HPV Types 16 and 18 account for about 70% of cervical cancer and high-grade lesions, whereas HPV Types 6 and 11 are associated with approximately 90% of anogenital warts.1 Together, these 4 types are responsible for over 40% of low-grade cervical lesions,2 and HPV 16 and 18 account for over 50% of high-grade lesions.3 The active quadrivalent vaccine is a mixture of 4 recombinant HPV type-specific VLPs consisting of the L1 major capsid proteins of HPV 6, 11, 16, and 18 synthesized in Saccharomyces cerevisiae.1 Expression of the L1 protein in yeast generates noninfectious VLPs that resemble HPV virions.1 A similar method is used for hepatitis B vaccine.4 The 4 VLP types were purified and absorbed onto amorphous aluminum hydroxyphosphate sulfate adjuvant.1 The adjuvant dose was 225 micrograms per dose, and the vaccine injection volume was 0.5 mL, given by intramuscular injection at Day 1, Month 2, and Month 6.1 GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. References 1. Villa LL, Costa RLR, Petta CA, et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: A randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol. 2005;6:271–278. 2. Clifford GM, Rana RK, Franceschi S, Smith JS, Gough G, Pimenta JM. Human papillomavirus genotype distribution in low-grade cervical lesions: Comparison by geographic region and with cervical cancer. Cancer Epidemiol Biomarkers Prev. 2005;14:1157–1164. 3. Clifford GM, Smith JS, Plummer M, Muñoz N, Franceschi S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br J Cancer. 2003;88:63–73. 4. Recombivax HB® Hepatitis B Vaccine (Recombinant) prescribing information. Merck & Co, Inc. Whitehouse Station, NJ 1/Villa/p. 271/col 2/ ¶1. 1/Villa/p. 271/col 1/ ¶2. 2/Clifford/ p.1159/col 2/¶3, table 2 3/Clifford/p.65/ col 2/¶2 GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. *VLP = Virus-like particle. 1. Villa LL, Costa RL, Petta CA, et al. Lancet Oncol. 2005;6:271–278. 1/Villa/p. 272/col 1/ ¶3. 1/Villa/p. 271/col 2/ ¶1. 3/Recombivax HB/p. 1/¶1. 1/Villa/p. 272/col 1/ ¶3. 1/Villa/p. 272/col 2/ ¶1,2.
 L1 VLP. VLPs em Saccharomyces cerevisiae. Aluminum adjuvante 225 μg por dose. - 20μg de HPV-6, 40 μg de HPV μg de HPV μg de HPV mL volume. 3 doses em 6 meses. 1/Villa/p. 272 /col 1/¶3. 1/Villa/p. 272 /col 1/¶4. 1/Villa/p. 272 /col 2/¶2. 1/Villa/p. 272 /col 2/¶2. Key Point. GARDASIL™ is Merck’s quadrivalent HPV L1 VLP vaccine. It is produced in recombinant yeast, like the hepatitis B vaccine, and adsorbed on a proprietary aluminum adjuvant, like the tetanus vaccine. Background. Merck’s quadrivalent vaccine has the advantage that it targets 4 HPV types (6, 11, 16 and 18).1 Together, HPV Types 16 and 18 account for about 70% of cervical cancer and high-grade lesions, whereas HPV Types 6 and 11 are associated with approximately 90% of anogenital warts.1 Together, these 4 types are responsible for over 40% of low-grade cervical lesions,2 and HPV 16 and 18 account for over 50% of high-grade lesions.3. The active quadrivalent vaccine is a mixture of 4 recombinant HPV type-specific VLPs consisting of the L1 major capsid proteins of HPV 6, 11, 16, and 18 synthesized in Saccharomyces cerevisiae.1 Expression of the L1 protein in yeast generates noninfectious VLPs that resemble HPV virions.1 A similar method is used for hepatitis B vaccine.4. The 4 VLP types were purified and absorbed onto amorphous aluminum hydroxyphosphate sulfate adjuvant.1 The adjuvant dose was 225 micrograms per dose, and the vaccine injection volume was 0.5 mL, given by intramuscular injection at Day 1, Month 2, and Month 6.1. GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. References. 1. Villa LL, Costa RLR, Petta CA, et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: A randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol. 2005;6:271– Clifford GM, Rana RK, Franceschi S, Smith JS, Gough G, Pimenta JM. Human papillomavirus genotype distribution in low-grade cervical lesions: Comparison by geographic region and with cervical cancer. Cancer Epidemiol Biomarkers Prev. 2005;14:1157– Clifford GM, Smith JS, Plummer M, Muñoz N, Franceschi S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br J Cancer. 2003;88:63– Recombivax HB® Hepatitis B Vaccine (Recombinant) prescribing information. Merck & Co, Inc. Whitehouse Station, NJ /Villa/p. 271/col 2/ ¶1. 1/Villa/p. 271/col 1/ ¶2. 2/Clifford/ p.1159/col 2/¶3, table 2. 3/Clifford/p.65/ col 2/¶2. GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. *VLP = Virus-like particle. 1. Villa LL, Costa RL, Petta CA, et al. Lancet Oncol. 2005;6:271–278. 1/Villa/p. 272/col 1/ ¶3. 1/Villa/p. 271/col 2/ ¶1. 3/Recombivax HB/p. 1/¶1. 1/Villa/p. 272/col 1/ ¶3. 1/Villa/p. 272/col 2/ ¶1,2.")
70
Vacina Anti HPV Acs mantém-se por anos Quem vacinar?
9 a 26 anos (mulheres) Meninos Mulheres até 45 anos
 Meninos. Mulheres até 45 anos.")
71
Risco de Aquisição do HPV Após a Primeira Relação Sexual
Risco cumulativo de infecção pelo HPV no colo do útero em adolescentes do sexo feminino com apenas um parceiro sexual1 Estudo em estudantes universitárias2 Risco cumulativo de infecção pelo HPV (%) 36 45 60 24 12 Meses desde a primeira relação sexual 10 40 50 70 30 20 N= 242 Adaptado de Collins e cols.1 46% HPV+ em 3anos 70 60 N= 603 40 Risco cumulativo de infecção pelo HPV (%) 20 4 8 12 16 20 24 28 32 36 40 44 48 52 56 Meses desde a primeira relação sexual Adaptado de Winer e cols.2 1. Collins S, Mazloomzadeh S, Winter H et al. BJOG 2002;109:96– Winer RL, Lee S-K, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: Incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218–226, com permissão da Oxford University Press.
 Meses desde a primeira relação sexual N= 242. Adaptado de Collins e cols.1. 46% HPV+ em 3anos N= Risco cumulativo de infecção pelo HPV (%) Meses desde a primeira relação sexual. Adaptado de Winer e cols Collins S, Mazloomzadeh S, Winter H et al. BJOG 2002;109:96– Winer RL, Lee S-K, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: Incidence and risk factors in a cohort of female university students. Am J Epidemiol 2003;157:218–226, com permissão da Oxford University Press.")
72
Projected Age-Specific Prevalence of HPV: Duke Model*,1
45 55 65 75 0.05 0.1 0.15 0.2 35 25 15 Age 0.30 0.25 Prevalence LSIL HSIL HPV Key Point The mathematical model of natural history of infection used to evaluate the prevalence of HPV infection and disease is calibrated with real life epidemiological data. This model shows that the peak prevalence of HPV occurs in adolescents and young adults, with a small rebound in middle age. Background As part of a systematic review of cervical cytology conducted at the Duke University Evidence-Based Practice Center between October 1997 and September 1998, Myers and colleagues constructed a Markov model of the natural history of cervical cancer building on previous studies and recent epidemiologic evidence. They projected that the prevalence of HPV rises sharply through adolescence, peaking at 24.7% in women 21 years of age. The prevalence of low-grade squamous intraepithelial lesions (LSIL) resulting from HPV infection peaks slightly later, at 28 years of age (prevalence = 8.3%). Prevalence of high-grade squamous intraepithelial lesions (HSIL) peaks at 42 years of age (prevalence = 2.6%).1 Reference 1. Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection and cervical carcinogenesis. Am J Epidemiol. 2000;151:1158–1171. Adapted from Myers, et al. *Cohort of women age 15 to 85 years LSIL = low-grade squamous intraepithelial lesions HSIL = high-grade squamous intraepithelial lesions 1. Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Am J Epidemiol. 2000;151:1158–1171.
 resulting from HPV infection peaks slightly later, at 28 years of age (prevalence = 8.3%). Prevalence of high-grade squamous intraepithelial lesions (HSIL) peaks at 42 years of age (prevalence = 2.6%).1. Reference. 1. Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection and cervical carcinogenesis. Am J Epidemiol. 2000;151:1158–1171. Adapted from Myers, et al. *Cohort of women age 15 to 85 years. LSIL = low-grade squamous intraepithelial lesions. HSIL = high-grade squamous intraepithelial lesions. 1. Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Am J Epidemiol. 2000;151:1158–1171.")
73
GARDASIL™ Phase III Adolescent Immunogenicity Substudy: Neutralizing Anti-HPV GMTs* at Month 7
Females 10–15 Years of Age Males 10–15 Years of Age Females 16–23 Years of Age Data on file/ Protocol 016/p /Tables; Nolan/ (females) slide 10; (males) slide 11. Key Point Higher antibody responses to each HPV type were observed in adolescent males and females compared with adult women in this Phase II study. Background Estimated GMTs for neutralizing anti-HPV 6, anti-HPV 11, anti-HPV 16, and anti-HPV 18 for adolescent females and males 10–15 years of age and females 16–23 years of age participating in this trial are shown on this slide.1 A noninferiority analysis demonstrated that immunogenic responses in adolescents were not inferior to those observed in older adolescents and adult females. In fact, younger adolescents showed higher antibody responses compared to older adolescents or adult females.1,2 Month 7 neutralizing anti-HPV GMTs in girls and boys were to 2.7-fold higher (noninferior, P<0.001) than in the other group.1,2 These results support the bridging of efficacy findings in older adolescent and young adult females to younger adolescents.1,2 GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. Reference 1. Nolan T, Block SL, Reisinger KS, et al. Comparison of the immunogenicity and tolerability of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, 18) L1 virus-like particle (VLP) vaccine in male and female adolescents and young adult women. Presented at: European Society for Paediatric Infectious Diseases (ESPID). Valencia, Spain; May 18–20, 2005. 1/Data on file/ Protocol 016/p /Tables; Nolan/ (females) slide 10; (males) slide 11 2/Nolan/ abstract/¶4, 1/Data on file/Protocol 016/p.17-18/Tables. 2/Nolan/slide 14. GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. *GMT = geometric mean titers 1/Data on file/Protocol /p26/¶ 2 1/Nolan/slide 15; 2/Nolan/abstract/ ¶5.
 slide 10; (males) slide 11. Key Point. Higher antibody responses to each HPV type were observed in adolescent males and females compared with adult women in this Phase II study. Background. Estimated GMTs for neutralizing anti-HPV 6, anti-HPV 11, anti-HPV 16, and anti-HPV 18 for adolescent females and males 10–15 years of age and females 16–23 years of age participating in this trial are shown on this slide.1 A noninferiority analysis demonstrated that immunogenic responses in adolescents were not inferior to those observed in older adolescents and adult females. In fact, younger adolescents showed higher antibody responses compared to older adolescents or adult females.1,2 Month 7 neutralizing anti-HPV GMTs in girls and boys were to 2.7-fold higher (noninferior, P<0.001) than in the other group.1,2. These results support the bridging of efficacy findings in older adolescent and young adult females to younger adolescents.1,2. GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. Reference. 1. Nolan T, Block SL, Reisinger KS, et al. Comparison of the immunogenicity and tolerability of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, 18) L1 virus-like particle (VLP) vaccine in male and female adolescents and young adult women. Presented at: European Society for Paediatric Infectious Diseases (ESPID). Valencia, Spain; May 18–20, /Data on file/ Protocol 016/p /Tables; Nolan/ (females) slide 10; (males) slide 11. 2/Nolan/ abstract/¶4, 1/Data on file/Protocol 016/p.17-18/Tables. 2/Nolan/slide 14. GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. *GMT = geometric mean titers. 1/Data on file/Protocol /p26/¶ 2. 1/Nolan/slide 15; 2/Nolan/abstract/ ¶5.")
74
Prevenção Condon Citologia aos 20 anos ou ao iniciar a vida sexual ativa

Apresentações semelhantes