Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Medicamentos atuantes no sistema reprodutivo feminino - Anticoncepcionais
Gilberto De Nucci

2
Dúvidas denucci@gilbertodenucci.com Arquivo
Medicamentos atuantes no sistema reprodutivo feminino - Anticoncepcionais Link

3
In the United States according to a study published in 2011
In 2006, 49% of pregnancies were unintended—a slight increase from 48% in Among women aged 19 years and younger, more than 4 out of 5 pregnancies were unintended. The proportion of pregnancies that were unintended was highest among teens younger than age 15 years, at 98%.

4
The anatomy of the female internal genitalia and accessory sex organs
Walter F. Boron/ Emile L. Boulpaep – Medical Physiology – Fig 54-1

5
The anatomy of the female internal genitalia and accessory sex organs
Walter F. Boron/ Emile L. Boulpaep – Medical Physiology – Fig 54-1

6
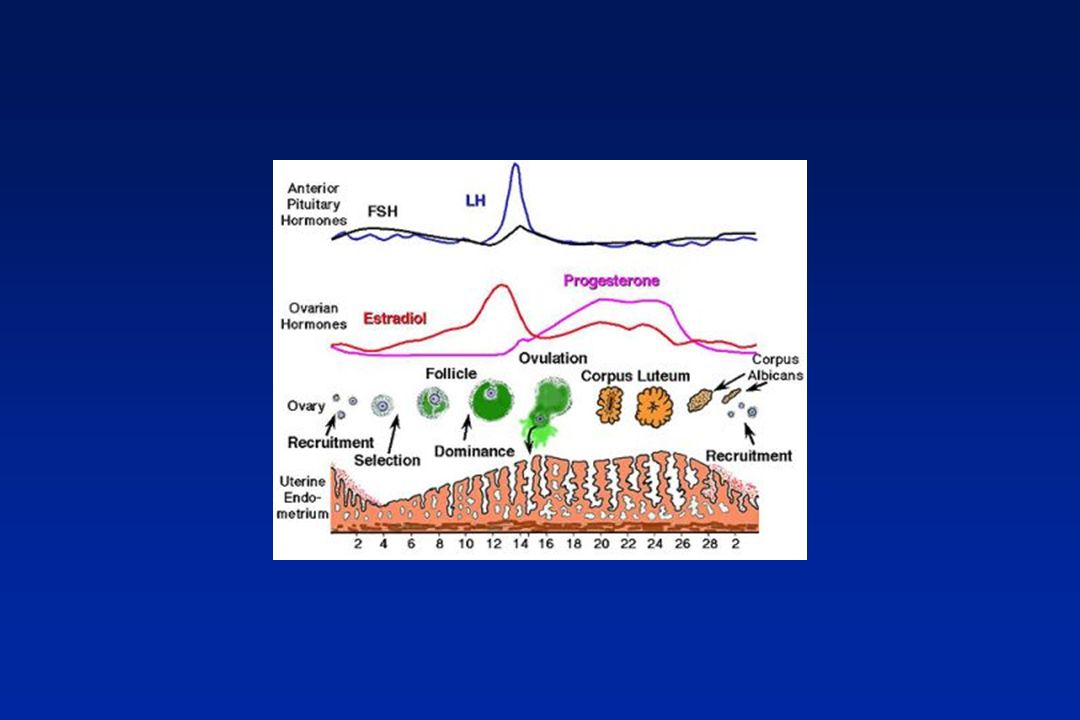
Ovarian cycle Rupture of mature follice and release of ovum (ovulatory phase) Growth and development of the follice (follicular phase) Corpus luteum formation (luteal phase) Corpus luteum degeneration Foyes Principles of Medicinal Chemistry – Fig. 29.2
 Corpus luteum degeneration. Foyes Principles of Medicinal Chemistry – Fig")
7
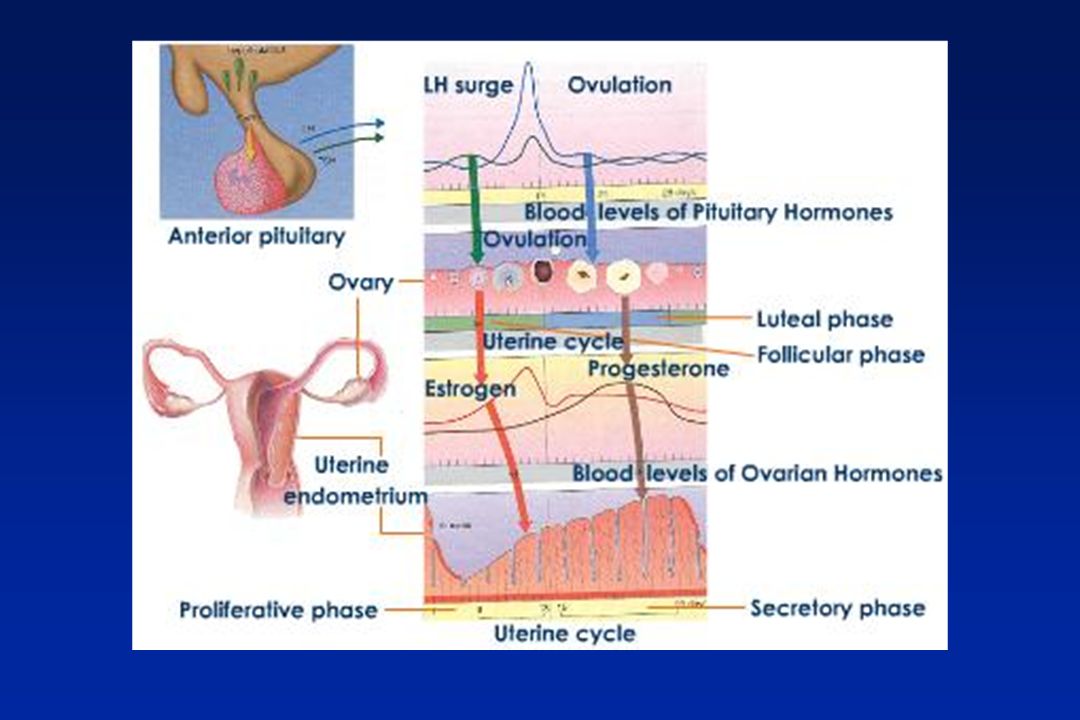
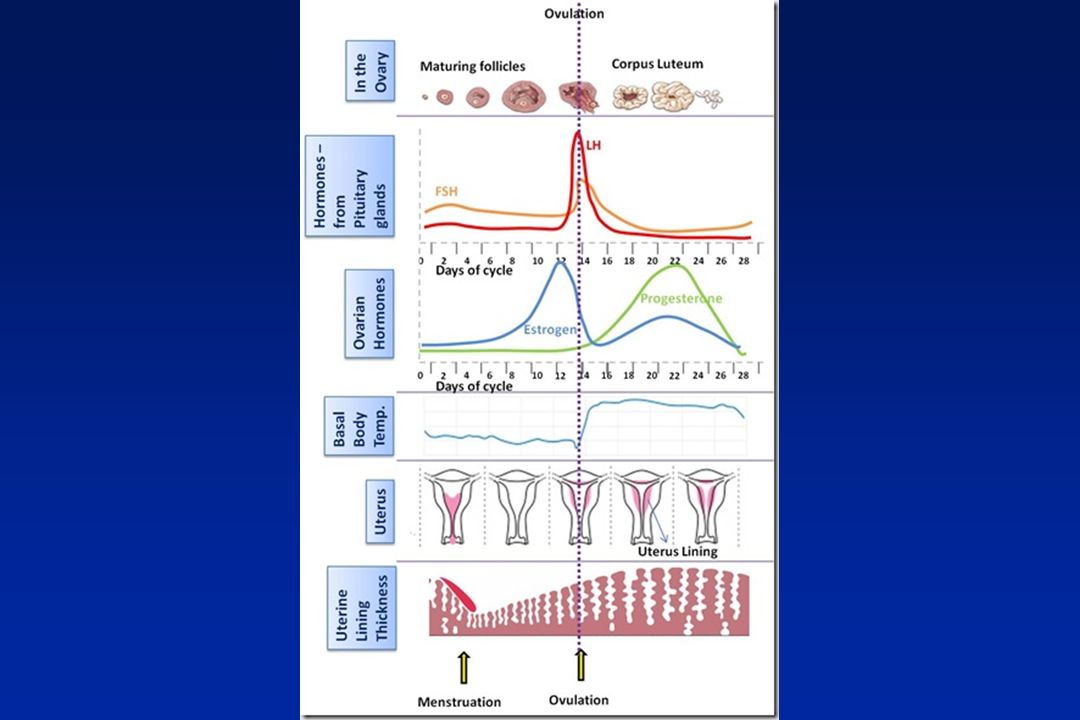
In this illustration, the menstrual cycle is divided into four stages.
an egg matures inside the ovary, which then releases the egg , allowing it to travel through the fallopian tube, where it rests awaiting fertilization If the egg is not fertilized, it is flushed out with the menstrual flow

8
Approximate plasma concentrations of the gonadotropins and ovarian hormones during the normal female sexual cycle 800 600 400 200 Progesterone 8 6 4 2 Ovulation Estradiol Menstruation Progesterone (ng/ml) Estradiol (pg/ml) 800 600 400 200 LH Ovulation FSH and LH (ng/ml) FSH Days of female sexual cycle Guyton & Hall – Textbook of Medical Physiology – fig 81.3
 Estradiol (pg/ml) LH. Ovulation. FSH and LH (ng/ml) FSH Days of female sexual cycle. Guyton & Hall – Textbook of Medical Physiology – fig")
15
Mechanism of Action of Estrogen/Progestin Contraceptives
Inhibition of ovulation by suppression of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) Alteration of cervical mucus to inhibit sperm transport Interference with ovum transport Inhibition of implantation by suppression of normal endometrial development Essential of Reproductive Medicine – Tab. 26.1
 and luteinizing hormone (LH) Alteration of cervical mucus to inhibit sperm transport. Interference with ovum transport. Inhibition of implantation by suppression of normal endometrial development. Essential of Reproductive Medicine – Tab")
16
Fertilization process

17
Estrogens excreted in urine
Estrogen secretion throughout the sexual life of the female human being 400 300 200 100 Puberty Menopause Estrogens excreted in urine (µg/24 hr) Age (yr) Guyton & Hall – Textbook of Medical Physiology – fig 81.10
 Age (yr) Guyton & Hall – Textbook of Medical Physiology – fig")
18
MÉTODOS ANTICONCEPCIONAIS
Tabela – Natural Barreira – impede o encontro - Diafragma - Preservativo - DIU normal Medicamentoso DIU – cobre ou progestogênico Skin patch Anel vaginal Implante Pílula

19
A clinical guide for contraception – fifth Ed – pg 191

20
CONTRACEPTIVOS HORMONAIS
Forma eficaz, segura e reversível. - Puros: somente progestágeno - Combinados: associação de estrogênio e progestágeno

21
Historical Landmarks Animal experiments in the late 1930s demonstrated that high- dose progesterone could arrest ovulation Carl Djerassi synthetized progestin from an extract of Mexican wild yam root in late 1940 First pill marketed for cycle control (1960) - Enovid 10 – mg norethynodrel microg mestranol Not legal to discuss contraception or prescribe the pill for the indication of contraception until 1969 Pope Paul VI Humanae Vitae (1968) – pill sinful Essential of Reproductive Medicine – Tab. 26.1
 - Enovid 10 – 9.85 mg norethynodrel microg mestranol. Not legal to discuss contraception or prescribe the pill for the indication of contraception until Pope Paul VI Humanae Vitae (1968) – pill sinful. Essential of Reproductive Medicine – Tab")
22
ESTROGÊNIO Década de 60 - Pró-Hormônio – Mestranol 150 mcg
Etinil Estradiol - Alta dose (> ou = 50 mcg) - Baixa dose (35, 30, 20, 15 mcg) - Tendência – Ultrabaixa (sem consenso)
 - Baixa dose (35, 30, 20, 15 mcg) - Tendência – Ultrabaixa (sem consenso)")
23
Mestranol (pró-droga)
A clinical Guide For Contraception - Fifth edition - pag 36

24
Ethinyl estradiol A clinical Guide For Contraception - Fifth edition - pag 36

25
Estradiol Valerate a

26
Low – Dose Oral Contraceptives
Products containing less than 50 mcg of ethinylestradiol

27
Classification of oral contraceptives
Into generation according to the type of progestogens associated with estrogen Combined (estrogen + progestin) or progesting only
 or progesting only.")
28
First-Generation Oral Contraceptives
Products containing either norethisterone acetate, lynestrenol, ethynodiol acetate or norethynodrel.

29
Testosterone Ethisterone
A clinical Guide For Contraception - Fifth edition - pag 37

30
Progestagional derivatives of testosterone
Ethisterone Norethindrone A clinical Guide For Contraception - Fifth edition - pag 37

31
A clinical Guide For Contraception - Fifth edition - pag 38

32
A clinical Guide For Contraception - Fifth edition - pag 38

33
Second-Generation Oral Contraceptives
Products containing levonorgestrel or norgestimate

34
A clinical Guide For Contraception - Fifth edition - pag 38

35
A clinical Guide For Contraception - Fifth edition - pag 41

36
Dienogest A clinical Guide For Contraception - Fifth edition - pag 42

37
Third-generation Oral Contraceptives
Products containing desogestrel, norgestimate or gestodene

38
A clinical Guide For Contraception - Fifth edition - pag 39

39
Fourth-Generation Oral Contraceptives
Products containing drospirenone, dienogest or nomegestrol acetate

40
Drospirenone A clinical Guide For Contraception - Fifth edition - pag 42

41
Nomegestrel s

42
Dienogest s

45
Change in adjusted mean number of lesions (papules, pustules, open and closed comedones) from baseline to end point (full analysis set). DRSP, drospirenone; EE, ethinyl estradiol; COC, indicates combined oral contraceptive; Hormonal Contraceptives for Acne Management – CUTANEOUS MEDICINE FOR THE PRACTITIONER - VOL. 81 NO. 1S JANUARY 2008

46
Oral Contraceptives With Acne Benefits
Pharmacology of Hormonal Contraceptives and Acne – CUTANEOUS MEDICINE FOR THE PRACTITIONER - VOL. 81 NO. 1S JANUARY 2008

47
Progestin only Low daily doses of progestin (norethindrone, levonorgestrel or desogestrel) Injectable 3-month contraceptives (depot medroxyprogesterone acetate) IM Levenorgestrel implant or etonogestrel single-rod implant – 3 years Intrauterine device containing levonorgestrel – 5 years
 IM. Levenorgestrel implant or etonogestrel single-rod implant – 3 years. Intrauterine device containing levonorgestrel – 5 years.")
48
Contraceptive use in the United States, 1995. Hysterectomy/ Menopause
Percentage of Women Ages 15-50 30 25 20 15 10 5 26% 24% 19% 7% 6% 3% 1% 1% 1% Pill Sterilization Condom Withdrawa/ Rhythm Hysterectomy/ Menopause Injectable Spermicide IUD Implants Method Essential of Reproductive Medicine – Fig. 26.2

49
A clinical Guide For Contraception - Fifth edition - pag 63

50
A clinical Guide For Contraception - Fifth edition - pag 66

51
Number of deaths from cardiovascular diseases per 100,000 women by smoking status or nonuse of oral contraceptives. 250 200 150 100 50 nonuser, nonsmoker user, nonsmoker nonuser, heavy smoker user, heavy smoker Deaths / 100,000 women 0 0 20-24 25-29 30-34 35-39 40-44 Age group (years) Essential of Reproductive Medicine – Fig. 26.4
 Essential of Reproductive Medicine – Fig")
52
Relative Risk and Actual Incidence of Venous Thromboembolism
Population Relative Risk Incidence Young women-general population per 100,000 per year Pregnant women High-dose oral contraceptives Low dose oral contraceptives Leiden mutation carrier Leiden carrier and oral contraceptives Leiden mutation – homozygous A Clinical Guide for Contraception – tab. Pag 53

53
Noncontraceptive Health Benefits of Oral Contraceptives
Percent Reduction/ Protection (%) Minium Use Required Duration of Effect OCP Formulation Comments Definitive evidence Ovarian cancer months At least >20 µg EE Also protective against years hereditary ovarian cancer Endometrial cancer months years All monophasic No data on multiphasic or progestin-only forms Benign breast disease months year >20 µg EE Effect consistent across all age groups Pelvic inflamatory months Current use >20 µg EE ? Effect on outpatient disease cases of PID Ectopic pregnancy Current use Current use >20 µg EE No increased risk for ectopic pregnancy in women who become pregnant with OCP use Essential of Reproductive Medicine – Tab. 26.2
 Minium Use Required. Duration of Effect. OCP Formulation. Comments. Definitive evidence. Ovarian cancer months At least 15 >20 µg EE Also protective against. years hereditary ovarian cancer. Endometrial cancer months 15 years All monophasic No data on multiphasic or. progestin-only forms. Benign breast disease months 1 year >20 µg EE Effect consistent across all age groups. Pelvic inflamatory months Current use >20 µg EE Effect on outpatient. disease cases of PID. Ectopic pregnancy 90 Current use Current use >20 µg EE No increased risk for ectopic. pregnancy in women who become. pregnant with OCP use. Essential of Reproductive Medicine – Tab")
54
Noncontraceptive Health Benefits of Oral Contraceptives
Percent Reduction/ Protection (%) Conflicting evidence, favor beneficial effect Bone mineral density Unknown Unknown >35 µg EE Decreased incidence of hip fractures with higher doses Colorectal cancer months Unknown >50 µg EE Increasing protection with increased duration Uterine leiomyomas , years; Unknown Unclear If used in setting of fibroids no 7 years clinically significant uterine growth Toxic shock syndrome Current use Current use Unclear May be influenced by change in tampon composition/absorbency Minium Use Required Duration of Effect OCP Formulation Comments Essential of Reproductive Medicine – Tab. 26.2
 Conflicting evidence, favor beneficial effect. Bone mineral density 60 Unknown Unknown >35 µg EE Decreased incidence of hip fractures. with higher doses. Colorectal cancer months Unknown >50 µg EE Increasing protection with. increased duration. Uterine leiomyomas 30, years; Unknown Unclear If used in setting of fibroids no. 7 years clinically significant uterine growth. Toxic shock syndrome 50 Current use Current use Unclear May be influenced by change in. tampon composition/absorbency. Minium Use Required. Duration of Effect. OCP Formulation. Comments. Essential of Reproductive Medicine – Tab")
55
Noncontraceptive Health Benefits of Oral Contraceptives
Percent Reduction/ Protection (%) Conflicting evidence, favor no effect Functional ovarian cysts 80, 48, 8 Current use Current use Monophasic No statistically significant effect >35 µg EE; Monophasic <35 mcg EE triphasic all types Rheumatoid arthritis Current use Current use Unclear May alter severity and clinical course rather development Minium Use Required Duration of Effect OCP Formulation Comments Essential of Reproductive Medicine – Tab. 26.2
 Conflicting evidence, favor no effect. Functional ovarian cysts 80, 48, 8 Current use Current use Monophasic No statistically significant effect. >35 µg EE; Monophasic. <35 mcg EE. triphasic all types. Rheumatoid arthritis 40 Current use Current use Unclear May alter severity and clinical. course rather development. Minium Use Required. Duration of Effect. OCP Formulation. Comments. Essential of Reproductive Medicine – Tab")
56
Benefícios dos AOC Menor risco de câncer endometrial e ovariano.
Menor risco de prenhez ectópica Menstruaçãoo mais regular (menor fluxo, menor dismenorréia, menor anemia) Menor incidência de salpingite Aumento da densidade óssea
 Menor incidência de salpingite. Aumento da densidade óssea.")
57
AOC e câncer Redução de 50% do risco de câncer de endométrico
Redução de 40% do risco de câncer de ovário Sem efeito no câncer de cérvix uterina ou no câncer de mama.

58
Possible Contradications to Use of Combined Oral Contraceptive Pills
Absolute Contraindications 1. Thrombophlebitis or Thromboembolic disorders 2. Past history of deep vein thrombophlebitis or thromboembolic disorders 3. Cerebrovascular or coronary artery disease 4. Known or suspected breast carcinoma 5. Known or suspected estrogen-dependent neoplasia 6. Pregnancy 7. Benign or malignant liver tumor 8. Known impaired liver function 9. Previous cholestasis during pregnancy or with prior pill use Essential of Reproductive Medicine – Tab. 26.6

59
Possible Contradications to Used of Combined Oral Contraceptive Pills (cont)
Strong Relative Contraindications 10. Severe headaches, particularly vascular or migraine headaches, that start after initiation of oral contraceptives 11. Hypertension with resting diastolic BP of 140 mmHg or greater on three or more separate visits or an accurate measurement of 110 mmHg diastolic or more on single visit 12. Mononucleosis, acute phase 13. Elective major surgery or major surgery requiring immobilization planned in next 4 week 14. Long-leg cast or major injury to lower leg 15. Over 40 years old, accompanied by a second risk factor for the development of cardiovascular disease (such as diabetes or hypertension) 16. Over 35 years old and currently a heavy smoker (15 or more cigarettes/day) 17. Abnormal genital bleeding Essential of Reproductive Medicine – Tab. 26.6
 16. Over 35 years old and currently a heavy smoker (15 or more cigarettes/day) 17. Abnormal genital bleeding. Essential of Reproductive Medicine – Tab")
60
Contraindicado formalmente em doença colestática aguda ou crônica
AOC e Fígado Transporte ativo de componentes biliares é inibido por estrógenos e progestágenos. Contraindicado formalmente em doença colestática aguda ou crônica

61
Importante Não há evidências de aumento de incidência de doença hepática séria causado por uso de ACO

62
Contraceptivo Oral e Trombose
Estrógenos, mas não progestágenos, aumentam a produção de fatores de coagulação. Tabagismo e uso de estrógenos apresentam efeito aditivo no risco de trombose arterial. Contraceptivos de dose baixa de estrógeno (< 50 microg EE) não aumentam o risco de IM ou AVC em mulheres saudáveis, não fumantes, independente da idade. IM e AVC podem ocorrer em mulheres que usam contraceptivos de alta dose, ou que apresentam fatores de risco cardiovascular acima da idade de 35 anos.
 não aumentam o risco de IM ou AVC em mulheres saudáveis, não fumantes, independente da idade. IM e AVC podem ocorrer em mulheres que usam contraceptivos de alta dose, ou que apresentam fatores de risco cardiovascular acima da idade de 35 anos.")
63
Medications That Decrease Serum Concentrations of Hormonal Contraception
Anticonvulsants Anti-infective agents Barbiturates Carbamazepine Phenytoin Rifampin Topiramate Vigabatrin Oral Contraceptives: Mechanism of Action, Dosing, Safety, and Efficacy – CUTANEOUS MEDICINE FOR THE PRACTITIONER - VOL. 81 NO. 1S JANUARY 2008

64
Monophasic pill Contains a fixed combination of a estrogen (generally ethinyl estradiol) and a progestogen
 and a progestogen.")
65
Biphasic Pill - Kariva 21 white tablets contains 0.15 mg desogestrel and 0.02 mg ethinyl estradiol. 2 light-green tablets contains inert ingredients 5 light-blue tablet contains 0.01 mg ethinyl estradiol.

66
Triphasic pill - Ortho Tri-Cyclen 28
7 tablet contains mg of norgestimate and mg of ethinyl estradiol 7 light blue tablet contains mg of norgestimate and mg of ethinyl estradiol 7 dark blue tablet contains mg of norgestimate and mg of ethinyl estradiol 7 green tablet contains only inert ingredients

67
Quadraphasic pill - Natazia
2 dark yellow tablets containing 3 mg estradiol valerate 5 red tablets containing 2 mg estradiol valerate and 2 mg dienogest 17 light yellow tablets containing 2 mg estradiol valerate and 3 mg dienogest 2 dark red tablets each containing 1 mg estradiol valerate 2 white tablets (inert)
")
68
Return of fertility after stopping contraception (Doll et al., 2001)
(with permission). Intrauterine devices and intrauterine systems - Human Reproduction Update, Vol.14, No.3 pp. 197–208, 2008
. Intrauterine devices and intrauterine systems - Human Reproduction Update, Vol.14, No.3 pp. 197–208,")
71
Escolha uma posição confortável para inserir o anel
Retire do Sachê Pressione o anel

72
Figura A Figura B Figura C Coloque o anel na vagina com uma das mãos (fig. A). Se necessário o lábio pode ser afastado com a outra mão. Empurre o anel para dentro da vagina até senti-lo confortável (fig. B) Deixe o anel no lugar durante 3 semanas (fig. C)
 Deixe o anel no lugar durante 3 semanas (fig. C)")
73
40 mm 2 mm Core: 40% Ethylene vinyl acetate (EVA)
60% Etogestrel (68 mg) Rate-controlling membrane: (.06 mm) 100% EVA
 Rate-controlling membrane: (.06 mm) 100% EVA.")
74
Required Equipment for Implanon Insertion

75
Implantation technique

76
Contraindication for Implanon
Known or suspected pregnancy Current or past history of thrombotic disease Hepatic tumors or active liver disease Undiagnosed abnormal genital bleeding Known, suspected or history of breast cancer Hypersensitivity to any of the components in Implanon™ A New Implantable Contraceptive - Nursing for Women’s Health - Volume 11 - Issue 6

78
Technique for the Tcu-380A

79
Níveis de levonorgestrel
A Clinical Guide for Contraception - Pag. 169

80
Serum levels of LNG according to delivery.
Author Route of delivery Serum levels (ng/ml) Raudaskoski et al. IUS –0.2 (1995) (PMW) Lahteenmaki et al mg oral ~ 1.7 (1995) Kives et al. (2005) mg oral 1.5 mg vaginal 5.4 Sivin et al. (1997) Implant 1.4–1.0 Rod Intrauterine devices and intrauterine systems - Human Reproduction Update, Vol.14, No.3 pp. 197–208, 2008
 Raudaskoski et al. IUS 0.1–0.2. (1995) (PMW) Lahteenmaki et al mg oral ~ 1.7. (1995) Kives et al. (2005) 1.5 mg oral mg vaginal 5.4. Sivin et al. (1997) Implant 1.4–1.0. Rod Intrauterine devices and intrauterine systems - Human Reproduction Update, Vol.14, No.3 pp. 197–208,")
81
HORMONIOS EM TRATAMENTOS
Correção de ciclos irregulares Reposição em caso de perdas de orgão produtores Complementos (Climatério)
")
Apresentações semelhantes





 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")







. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")





 2003 by Valery Sklyarov and Iouliia Skliarova: DETUA, IEETA, Aveiro University, Portugal.>")



