Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Bom Dia! Dor na Unidade de Terapia Intensiva:
Perspectiva de um Intensivista Pediátrico Alexandre Serafim Unidade de Neonatologia do Hospital Regional da Asa Sul/SES/DF 16/7/2008

2
Dor Neonatal: os efeitos da anestesia
“agentes anestésicos ou analgésicos são desnecessários na cirurgia de fechamento do canal arterial” Lippmann, Ligation of patent ductus arteriosus in premature infants. Br. J. Anaesth. 48: “59% das enfermeiras acreditam que neonatos não sentem dor da mesma forma que adultos” Franke, L., C. Lurid, and A. Fanaroff A national survey of the assessment and treatment of pain in the newborn intensive care unit (abstract). Pediatr. Res. 20:347A. Twenty-four neonates at weeks' gestation with a weight range of g underwent ligation of patent ductus arteriosus (PDA). The infants had mild to severe respiratory distress syndrome at birth and later developed signs of heart failure as a result of left-to-right shunting through a PDA. Surgical closure of the PDA was performed within 2-31 days after birth. In the period before operation the heart rate was monitored constantly and the arterial blood-gases were assessed frequently. The trachea was intubated and respiration was controlled with a ventilator. Surgery was performed under controlled ventilation and no anaesthesia was used. Care was taken not to overventilate the lungs. Nine infants died. Death was associated with higher peak inspiratory ventilator pressures at the time of operation and with complications occurring during or after the operation. The most common complication was tension pneumomediastinum which appears to be related to excessive ventilator pressures during surgery Br J Anaesth Apr ;48 (4):365-9 Twenty-four neonates at weeks' gestation with a weight range of g underwent ligation of patent ductus arteriosus (PDA). The infants had mild to severe respiratory distress syndrome at birth and later developed signs of heart failure as a result of left-to-right shunting through a PDA. Surgical closure of the PDA was performed within 2-31 days after birth. In the period before operation the heart rate was monitored constantly and the arterial blood-gases were assessed frequently. The trachea was intubated and respiration was controlled with a ventilator. Surgery was performed under controlled ventilation and no anaesthesia was used. Care was taken not to overventilate the lungs. Nine infants died. Death was associated with higher peak inspiratory ventilator pressures at the time of operation and with complications occurring during or after the operation. The most common complication was tension pneumomediastinum which appears to be related to excessive ventilator pressures during surgery Br J Anaesth Apr ;48 (4):365-9
. Pediatr. Res. 20:347A. Twenty-four neonates at weeks gestation with a weight range of g underwent ligation of patent ductus arteriosus (PDA). The infants had mild to severe respiratory distress syndrome at birth and later developed signs of heart failure as a result of left-to-right shunting through a PDA. Surgical closure of the PDA was performed within 2-31 days after birth. In the period before operation the heart rate was monitored constantly and the arterial blood-gases were assessed frequently. The trachea was intubated and respiration was controlled with a ventilator. Surgery was performed under controlled ventilation and no anaesthesia was used. Care was taken not to overventilate the lungs. Nine infants died. Death was associated with higher peak inspiratory ventilator pressures at the time of operation and with complications occurring during or after the operation. The most common complication was tension pneumomediastinum which appears to be related to excessive ventilator pressures during surgery Br J Anaesth Apr ;48 (4): Twenty-four neonates at weeks gestation with a weight range of g underwent ligation of patent ductus arteriosus (PDA). The infants had mild to severe respiratory distress syndrome at birth and later developed signs of heart failure as a result of left-to-right shunting through a PDA. Surgical closure of the PDA was performed within 2-31 days after birth. In the period before operation the heart rate was monitored constantly and the arterial blood-gases were assessed frequently. The trachea was intubated and respiration was controlled with a ventilator. Surgery was performed under controlled ventilation and no anaesthesia was used. Care was taken not to overventilate the lungs. Nine infants died. Death was associated with higher peak inspiratory ventilator pressures at the time of operation and with complications occurring during or after the operation. The most common complication was tension pneumomediastinum which appears to be related to excessive ventilator pressures during surgery Br J Anaesth Apr ;48 (4):")
3
Em 10 prematuros (1223 g ± 263 g), fentanyl
(30 a 50 mcg/kg) foi utilizado em conjunto com Pancurônio (0,1 mg/kg) como anestesia para Ligadura trans-torácica de ducto arterioso patente. Estabilidade hemodinâmica foi observada durante Todo o procedimento. A rigidez torácica foi evitada Com o uso de bloqueadores musculares. Todos os Pacientes estavam acordados 1 hora após o procedimento. Robinson, S., and G. A. Gregory Fentanyl-air-oxygen anesthesia for ligation of patent ductus arteriosus in preterm infants. Anesth. Analg. 60: In 10 premature infants (1123 ± 263 g), fentanyl citrate (30 to 50 µg/kg) was used in conjunction with pancuronium (0.1 mg/kg) as the sole anesthetic for transthoracic ligation of patent ductus arteriosus. Ventilation was controlled with air and oxygen in concentrations sufficient to maintain transcutaneous Po2 between 50 and 70 torr. Circulatory stability was easily maintained throughout the procedure. "Stiff chest" was avoided by the use of muscle relaxants, and the infants were awake within 1 hour after the procedure.
 foi utilizado em conjunto com. Pancurônio (0,1 mg/kg) como anestesia para. Ligadura trans-torácica de ducto arterioso patente. Estabilidade hemodinâmica foi observada durante. Todo o procedimento. A rigidez torácica foi evitada. Com o uso de bloqueadores musculares. Todos os. Pacientes estavam acordados 1 hora após o procedimento. Robinson, S., and G. A. Gregory Fentanyl-air-oxygen anesthesia. for ligation of patent ductus arteriosus in preterm infants. Anesth. Analg. 60: In 10 premature infants (1123 ± 263 g), fentanyl citrate (30 to 50 µg/kg) was used in conjunction with pancuronium (0.1 mg/kg) as the sole anesthetic for transthoracic ligation of patent ductus arteriosus. Ventilation was controlled with air and oxygen in concentrations sufficient to maintain transcutaneous Po2 between 50 and 70 torr. Circulatory stability was easily maintained throughout the procedure. Stiff chest was avoided by the use of muscle relaxants, and the infants were awake within 1 hour after the procedure.")
4
PAIN AND ITS EFFECTS IN THE HUMAN NEONATE AND FETUS
A ausência de mielinização já foi utilizada como argumento para a não percepção de dor nos neonatos Em adultos, os impulsos nociceptivos percorrem fibras não mielinizadas (C-polimodais) ou pouco mielinizadas (A-delta) Mielinização incompleta implica em velocidade de condução menor, mas as distâncias interneuronais são menores no neonato
 ou pouco mielinizadas (A-delta) Mielinização incompleta implica em velocidade de condução menor, mas as distâncias interneuronais são menores no neonato.")
6
Halothane-morphine compared with high-dose sufentanil for anesthesia and postoperative analgesia in neonatal cardiac surgery 30 neonatos foram randomizados para receber fentanil ou uma combinação de halotano e morfina Os neonatos do grupo sufentanil apresenaram menor elevação de adrenalina e noradrenalina e redução do cortisol, menor incidência de sepse, acidose metabólica e CIVD O grupo que recebeu halotano e morfina apresentou mais hiperglicemia e acidemia láctica, além de maior mortalidade BACKGROUND. Extreme hormonal and metabolic responses to stress are associated with increased morbidity and mortality in sick adults. We hypothesized that administering deep opioid anesthesia to critically ill neonates undergoing cardiac surgery would blunt their responses to stress and might improve clinical outcomes. METHODS. In a randomized trial, 30 neonates were assigned to receive deep intraoperative anesthesia with high doses of sufentanil and postoperative infusions of opiates for 24 hours; 15 neonates were assigned to receive lighter anesthesia with halothane and morphine followed postoperatively by intermittent morphine and diazepam. Hormonal and metabolic responses to surgery were evaluated by assay of arterial blood samples obtained before, during, and after the operations. RESULTS. The neonates who received deep anesthesia (with sufentanil) had significantly reduced responses of beta-endorphin, norepinephrine, epinephrine, glucagon, aldosterone, cortisol, and other steroid hormones; their insulin responses and ratios of insulin to glucagon were greater during the operation. The neonates who received lighter anesthesia (with halothane plus morphine) had more severe hyperglycemia and lactic acidemia during surgery and higher lactate and acetoacetate concentrations postoperatively (P less than 0.025). The group that received deep anesthesia had a decreased incidence of sepsis (P = 0.03), metabolic acidosis (P less than 0.01), and disseminated intravascular coagulation (P = 0.03) and fewer postoperative deaths (none of 30 given sufentanil vs. 4 of 15 given halothane plus morphine, (P less than 0.01). CONCLUSIONS. In neonates undergoing cardiac surgery, the physiologic responses to stress are attenuated by deep anesthesia and postoperative analgesia with high doses of opioids. Deep anesthesia continued postoperatively may reduce the vulnerability of these neonates to complications and may reduce mortality. N Engl J Med 1992; 326: 1–9
 had significantly reduced responses of beta-endorphin, norepinephrine, epinephrine, glucagon, aldosterone, cortisol, and other steroid hormones; their insulin responses and ratios of insulin to glucagon were greater during the operation. The neonates who received lighter anesthesia (with halothane plus morphine) had more severe hyperglycemia and lactic acidemia during surgery and higher lactate and acetoacetate concentrations postoperatively (P less than 0.025). The group that received deep anesthesia had a decreased incidence of sepsis (P = 0.03), metabolic acidosis (P less than 0.01), and disseminated intravascular coagulation (P = 0.03) and fewer postoperative deaths (none of 30 given sufentanil vs. 4 of 15 given halothane plus morphine, (P less than 0.01). CONCLUSIONS. In neonates undergoing cardiac surgery, the physiologic responses to stress are attenuated by deep anesthesia and postoperative analgesia with high doses of opioids. Deep anesthesia continued postoperatively may reduce the vulnerability of these neonates to complications and may reduce mortality. N Engl J Med 1992; 326: 1–9.")
7
Stress Response in Infants Undergoing Cardiac Surgery: A Randomized Study of Fentanyl Bolus, Fentanyl Infusion, and Fentanyl-Midazolam Infusion Grupo 1: Fentanyl bolus 25 mcg/kg Grupo 2: Fentanyl em bolus 25 mcg/kg seguido de infusão contínua 10 mcg/kg/h Grupo 3: Fentanyl (bolus) + midazolam (200mcg/kg) seguido de fentanyl contínuo e midazolam contínuo (100mcg/kg/h) Anesth Analg 2001;92:
 + midazolam (200mcg/kg) seguido de fentanyl contínuo e midazolam contínuo (100mcg/kg/h) Anesth Analg 2001;92:")
8
Figure 2. Changes in cortisol and ACTH concentrations across time
Gruber, E. M. et al. Anesth Analg 2001;92:

9
Figure 1. Changes in plasma epinephrine and norepinephrine concentrations across time
There have been significant changes in the management of neonates and infants undergoing cardiac surgery in the past decade. We have evaluated in this prospective, randomized, double-blinded study the effect of large-dose fentanyl anesthesia, with or without midazolam, on stress responses and outcome. Forty-five patients < 6 mo of age received bolus fentanyl (Group 1), fentanyl by continuous infusion (Group 2), or fentanyl-midazolam infusion (Group 3). Epinephrine, norepinephrine, cortisol, adrenocortical hormone, glucose, and lactate were measured after the induction (T1), after sternotomy (T2), 15 min after initiating cardiopulmonary bypass (T3), at the end of surgery (T4), and after 24 h in the intensive care unit (T5). Plasma fentanyl concentrations were obtained at all time points except at T5. Within each group epinephrine, norepinephrine, cortisol, glucose and lactate levels were significantly larger at T4 (P values < 0.01), but there were no differences among groups. Within groups, fentanyl levels were significantly larger in Groups 2 and 3 (P < 0.001) at T4, and among groups, the fentanyl level was larger only at T2 in Group 1 compared with Groups 2 and 3 (P<0.006). There were no deaths or postoperative complications, and no significant differences in duration of mechanical ventilation or intensive care unit or hospital stay. Fentanyl dosing strategies, with or without midazolam, do not prevent a hormonal or metabolic stress response in infants undergoing cardiac surgery. Implications: We demonstrated a significant endocrine stress response in infants with well compensated congenital cardiac disease undergoing cardiac surgery, but without adverse postoperative outcome. The use of large-dose fentanyl, with or without midazolam, with the intention of providing "stress free" anesthesia, does not appear to be an important determinant of early postoperative outcome. Gruber, E. M. et al. Anesth Analg 2001;92:
, fentanyl by continuous infusion (Group 2), or fentanyl-midazolam infusion (Group 3). Epinephrine, norepinephrine, cortisol, adrenocortical hormone, glucose, and lactate were measured after the induction (T1), after sternotomy (T2), 15 min after initiating cardiopulmonary bypass (T3), at the end of surgery (T4), and after 24 h in the intensive care unit (T5). Plasma fentanyl concentrations were obtained at all time points except at T5. Within each group epinephrine, norepinephrine, cortisol, glucose and lactate levels were significantly larger at T4 (P values < 0.01), but there were no differences among groups. Within groups, fentanyl levels were significantly larger in Groups 2 and 3 (P < 0.001) at T4, and among groups, the fentanyl level was larger only at T2 in Group 1 compared with Groups 2 and 3 (P<0.006). There were no deaths or postoperative complications, and no significant differences in duration of mechanical ventilation or intensive care unit or hospital stay. Fentanyl dosing strategies, with or without midazolam, do not prevent a hormonal or metabolic stress response in infants undergoing cardiac surgery. Implications: We demonstrated a significant endocrine stress response in infants with well compensated congenital cardiac disease undergoing cardiac surgery, but without adverse postoperative outcome. The use of large-dose fentanyl, with or without midazolam, with the intention of providing stress free anesthesia, does not appear to be an important determinant of early postoperative outcome. Gruber, E. M. et al. Anesth Analg 2001;92:")
10
Diferenças entre os estudos de Gruber e Anand
No estudo de Eva Gruber houve elevação dos níveis de cortisol durante a cirurgia,enquanto Anand observou uma redução nos níveis de cortisol no grupo sufentanil Anand demonstrou um aumento entre 0,5 e 1 x nos níveis de epinefrina, enquanto no estudo Gruber, a epinefrina aumentou 8 x no Grupo 1, 12 x no Grupo 2 e 15 x no Grupo 3 Direct comparisons between the two studies clearly are not possible. In the earlier study, patients in were younger (mean age, 5.3 days), the diagnoses, surgical procedures, and bypass techniques were different (e.g., 15 of 45 patients underwent a Stage I repair for hypoplastic left heart syndrome), and a larger circuit prime volume and different laboratory assays were used to measure the neuroendocrine response (2). The magnitude of the change in neuroendocrine response may also be different between the two studies, particularly as the original study included neonates managed in the ICU before surgery. Further, sufentanil was used in the early study whereas fentanyl is currently more commonly used in our institution for congenital cardiac surgery. At equipotent doses (5–10:1 ratio), sufentanil and fentanyl have a similar pharmacodynamic profile and stress hormone release during cardiac surgery (3,17,18). In contrast, one study involving adult volunteers suggested that sufentanil may have an increased affinity for the µ1 receptor compared with fentanyl (19), although there are no data to support this in pediatric patients. The total bolus dose of sufentanil used in the early study (total 30 µg/kg) is relatively larger than the total bolus dose of fentanyl used in this study (100 µg/kg), which may account for the smaller increase in epinephrine levels in the early study (2).
, the diagnoses, surgical procedures, and bypass techniques were different (e.g., 15 of 45 patients underwent a Stage I repair for hypoplastic left heart syndrome), and a larger circuit prime volume and different laboratory assays were used to measure the neuroendocrine response (2). The magnitude of the change in neuroendocrine response may also be different between the two studies, particularly as the original study included neonates managed in the ICU before surgery. Further, sufentanil was used in the early study whereas fentanyl is currently more commonly used in our institution for congenital cardiac surgery. At equipotent doses (5–10:1 ratio), sufentanil and fentanyl have a similar pharmacodynamic profile and stress hormone release during cardiac surgery (3,17,18). In contrast, one study involving adult volunteers suggested that sufentanil may have an increased affinity for the µ1 receptor compared with fentanyl (19), although there are no data to support this in pediatric patients. The total bolus dose of sufentanil used in the early study (total 30 µg/kg) is relatively larger than the total bolus dose of fentanyl used in this study (100 µg/kg), which may account for the smaller increase in epinephrine levels in the early study (2).")
13
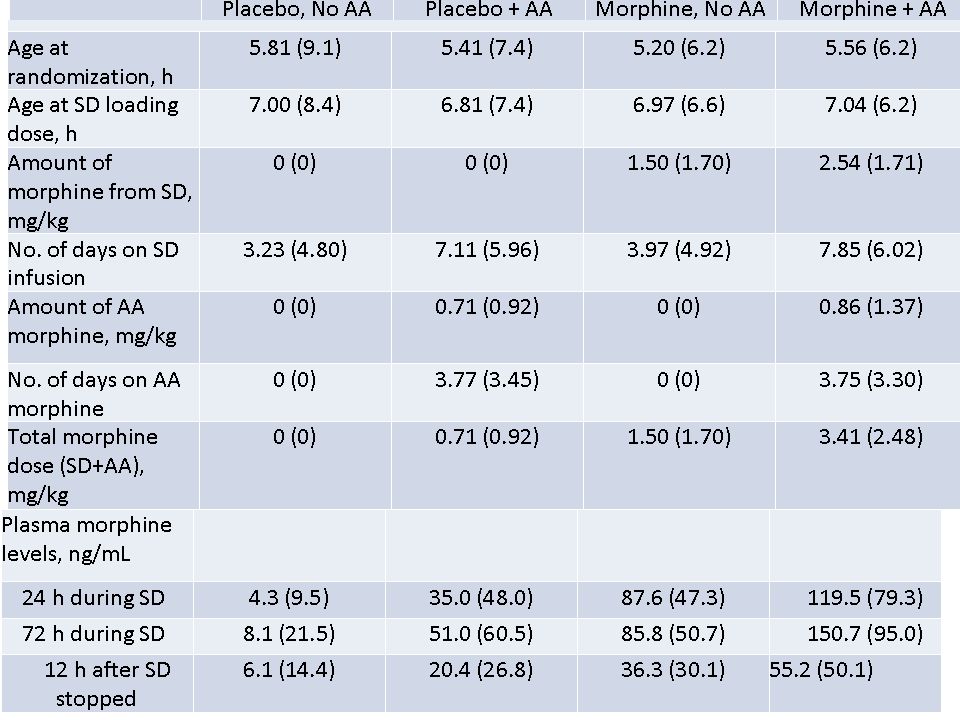
NEOPAIN: Resultados Óbito neonatal: OR: 1.16; 95% confidence interval (CI): 0.72–1.88; P = .5459 HIV grave: OR: 1.33; 95% CI: 0.85–2.10; P = .2153 Leucomalácia periventricular: OR: 0.80; 95% CI: 0.47–1.36; P = .4080

14
Analgesia para procedimentos: Epidemiologia

17
Procedimentos dolorosos Número
% sob analgesia específica (para o procedimento) % sob analgesia sistêmica (indicada por outro motivo) Punções arteriais 921 zero 41% Punções venosas 1.045 29% Punções capilares 1.437 27% Punções lombares 64 39% Inserções de cateteres centrais 73 8% 37% Inserções de dreno torácico 8 100% 75% Intubações traqueais 115 28% Frequência do emprego de analgésicos em UTI Neonatais J Pediatr (Rio J) 2005
 % sob analgesia sistêmica (indicada por outro motivo) Punções arteriais zero. 41% Punções venosas % Punções capilares % Punções lombares % Inserções de cateteres centrais % 37% Inserções de dreno torácico % 75% Intubações traqueais % Frequência do emprego. de analgésicos em. UTI Neonatais. J Pediatr (Rio J)")
18
Roberts, K. D. et al. Pediatrics 2006;118:1583-1591
FIGURE 2 Time results The purpose of this work was to investigate whether using a muscle relaxant would improve intubation conditions in infants, thereby decreasing the incidence and duration of hypoxia and time and number of attempts needed to successfully complete the intubation procedure. PATIENTS/METHODS: This was a prospective, randomized, controlled, 2-center trial. Infants requiring nonemergent intubation were randomly assigned to receive atropine and fentanyl or atropine, fentanyl, and mivacurium before intubation. Incidence and duration of hypoxia were determined at oxygen saturation thresholds of < or = 85%, < or = 75%, < or = 60%, and < or = 40%. Videotape was reviewed to determine the time and number of intubation attempts and duration of action of mivacurium. RESULTS: Analysis of 41 infants showed that incidence of oxygen saturation < or = 60% of any duration was significantly less in the mivacurium group (55% vs 24%). The incidence of saturation level of any duration < or = 85%, 75%, and 40%; cumulative time > or = 30 seconds; and time below the thresholds were not significantly different. Total procedure time (472 vs 144 seconds) and total laryngoscope time (148 vs 61 seconds) were shorter in the mivacurium group. Successful intubation was achieved in < or = 2 attempts significantly more often in the mivacurium group (35% vs 71%). CONCLUSIONS: Premedication with atropine, fentanyl, and mivacurium compared with atropine and fentanyl without a muscle relaxant decreases the time and number of attempts needed to successfully intubate while significantly reducing the incidence of severe desaturation. Premedication including a short-acting muscle relaxant should be considered for all nonemergent intubations in the NICU. Roberts, K. D. et al. Pediatrics 2006;118: Ensaio clínico controlado e randomizado comparando atropina e fentanyl com atropina, fentanyl e mivacurium
. The incidence of saturation level of any duration < or = 85%, 75%, and 40%; cumulative time > or = 30 seconds; and time below the thresholds were not significantly different. Total procedure time (472 vs 144 seconds) and total laryngoscope time (148 vs 61 seconds) were shorter in the mivacurium group. Successful intubation was achieved in < or = 2 attempts significantly more often in the mivacurium group (35% vs 71%). CONCLUSIONS: Premedication with atropine, fentanyl, and mivacurium compared with atropine and fentanyl without a muscle relaxant decreases the time and number of attempts needed to successfully intubate while significantly reducing the incidence of severe desaturation. Premedication including a short-acting muscle relaxant should be considered for all nonemergent intubations in the NICU. Roberts, K. D. et al. Pediatrics 2006;118: Ensaio clínico controlado e randomizado comparando atropina e fentanyl. com atropina, fentanyl e mivacurium.")
19
Analgesia para Procedimentos: Emergência Pediátrica

20
Safe and Efficacious Use of Procedural Sedation and Analgesia by Nonanesthesiologists
in a Pediatric Emergency Department Figure 2. Type and frequency of use of procedural sedation and analgesia (PSA) regimens. IV indicates intravenous; IM, intramuscular. Arch Pediatr Adolesc Med. 2003;157:
 regimens. IV indicates intravenous; IM, intramuscular. Arch Pediatr Adolesc Med. 2003;157:")
21
Figure 3. Number and type of adverse reactions noted during sedation.

22
Perfil do uso de analgésicos e sedativos entre pacientes clínicos e cirúrgicos
que necessitaram de ventilação mecânica por mais de doze horas Clínicos (n = 92) n (%) Cirúrgicos (n = 32) n (%) P Midazolan 84 (91,3) 16 (50,0) < 0,001 Fentanil 70 (76,1) 14 (43,8) Morfina 4 (4,3) 11 (34,4) 0,01 Quetamina 21 (22,8) J Pediatr (Rio J) 2003;79(4):343-8
 n (%) Cirúrgicos (n = 32) n (%) P. Midazolan. 84 (91,3) 16 (50,0) < 0,001. Fentanil. 70 (76,1) 14 (43,8) Morfina. 4 (4,3) 11 (34,4) 0,01. Quetamina. 21 (22,8) J Pediatr (Rio J) 2003;79(4):")
23
Sedação e Analgesia Contínua na UTI Pediátrica

24
Pacientes clínicos Dose média + dp
Comparação das doses médias utilizadas nos pacientes clínicos e cirúrgicos submetidos à ventilação mecânica por mais de doze horas Pacientes clínicos Dose média + dp Pacientes cirúrgicos Dose média + dp p Midazolan (mg/kg/hora) 0,546+0,3 0,424+0,3 0,172 Fentanil (μg/kg/hora) 5,5+3,8 4,87+3,3 0,597 Morfina (μg/kg/hora) 22,2+17,0 12,86+5,3 0,325 Quetamina (μg/kg/min) 33,8+9,6 - Incidência de abstinência 49% J Pediatr (Rio J) 2003;79(4):343-8
 0,546+0,3. 0,424+0,3. 0,172. Fentanil (μg/kg/hora) 5,5+3,8. 4,87+3,3. 0,597. Morfina (μg/kg/hora) 22,2+17,0. 12,86+5,3. 0,325. Quetamina (μg/kg/min) 33,8+9,6. - Incidência de abstinência 49% J Pediatr (Rio J) 2003;79(4):")
25
Midazolam (n) Média + dp
Relação entre o tempo de uso dos sedativos e analgésicos e a dose média empregada nos pacientes submetidos à ventilação mecânica < 3 dias (a) (A) 3 - 7 dias (B) > 7 dias (C) p Midazolam (n) Média + dp (mg/kg/h) (26) 0,394+0,288 (40) 0,460+0,266 (34) 0,707+0,351 AxB= 0,355 AxC= 0,0004 BxC= 0,001 Fentanil (n) Média + dp ( g/kg/h) (21) 4,00+2,93 (34) 4,51+2,82 (29) 7,31+4,25 AxB= 0,528 AxC= 0,002 BxC= 0,004 Morfina (n) Média + dp (8) 12,18+3,96 (4) 15,50+7,31 (3) 23,65+19,15 AxB= 0,466 AxC= 0,409 BxC= 0,544 Ketamina (n) Média + dp ( g/kg/min) (3) 36,31+15,01 (5) 37,21+12,41 (12) 31,89+7,19 AxB= 0,934 AxC= 0,666 BxC= 0,409
 (A) dias (B) > 7 dias (C) p. Midazolam (n) Média + dp. (mg/kg/h) (26) 0,394+0,288. (40) 0,460+0,266. (34) 0,707+0,351. AxB= 0,355 AxC= 0,0004 BxC= 0,001. Fentanil (n) Média + dp. ( g/kg/h) (21) 4,00+2,93. (34) 4,51+2,82. (29) 7,31+4,25. AxB= 0,528 AxC= 0,002 BxC= 0,004. Morfina (n) Média + dp. (8) 12,18+3,96. (4) 15,50+7,31. (3) 23,65+19,15. AxB= 0,466 AxC= 0,409 BxC= 0,544. Ketamina (n) Média + dp. ( g/kg/min) (3) 36,31+15,01. (5) 37,21+12,41. (12) 31,89+7,19. AxB= 0,934 AxC= 0,666 BxC= 0,409.")
26
Problemas da Sedação e Analgesia
Interrupção diária da sedoanalgesia Avaliação diária de capacidade de respiração espontânea Uso de medidas não farmacológicas Rodízio de drogas Uso de naloxone junto com opióides (?) Uso de drogas de curta duração (dexmedetomidina) Prolonga o tempo de Ventilação Mecânica Tolerância Síndrome de Abstinência Imunossupressão
 Uso de drogas de curta duração (dexmedetomidina) Prolonga o tempo de Ventilação Mecânica. Tolerância. Síndrome de Abstinência. Imunossupressão.")
27
Lira, MF. Presença dos pais na UTIP: avaliação do impacto no estresse dos crianças internadas.

28
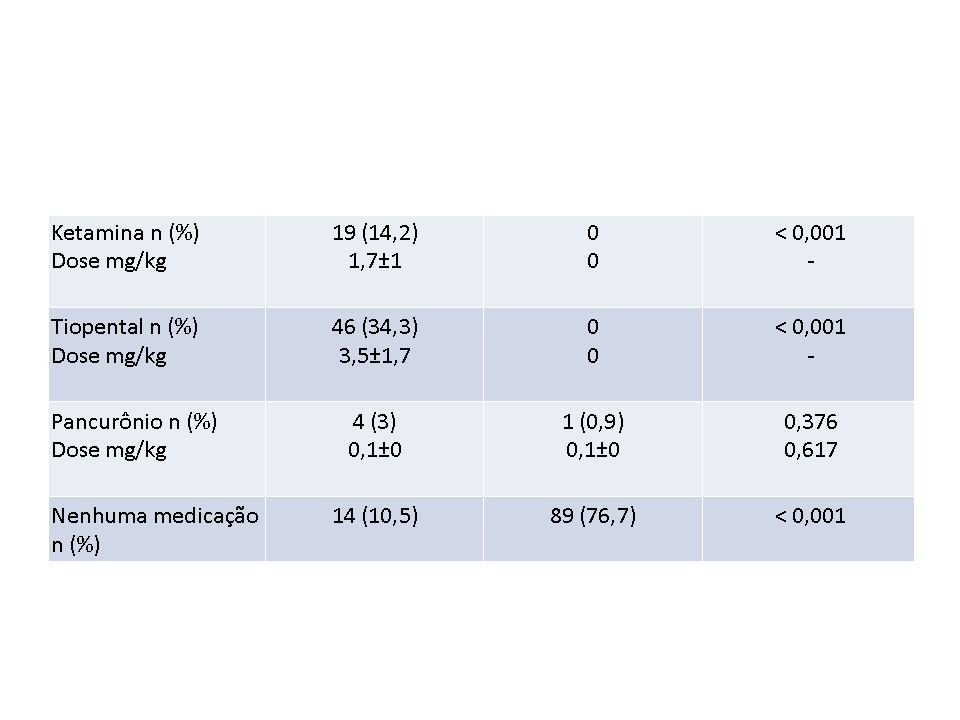
Ketamina a. Dissociativa [Ann Emerg Med, 2004. 44(5): p. 460-71]
b. Analgesia, Sedação, Amnésia, Broncodilatação c. Ketamina Oral a 10mg/kg[Pediatr Emerg Care, (2): p. 93-7] 1) 2/15 vomitaram 2) Início da sedação em 35 minutos d. Ketamine IV [Ann Emerg Med, (3): p ] 1) Início da sedação em 60 segundos[Crit Care Med, (6): p ] - 13 minutos 2) Eventos adversos VAS/Desat. 2%,4.5%, [Ann Emerg Med, (6): p ] 11%[Pediatrics, (4): p. e ] 3) Emergência 6 – 15% 4) Recuperação 50,[Crit Care Med, 2002 ] 64 minutos[. Ann Emerg Med, 2000 ] – 85min[Pediatrics, (4): p. e ] 5) Uso de analgésicos previamente pode retardar a recuperação [Pediatr Emerg Care, (2): p ] e. Ketamine IM a 4 -5 mg/kg[Acad Emerg Med, (1): p ] 1) Início da sedação em 5 minutos 2) De 431 pacientes no PS[Acad Emerg Med, 1999 ], desalinhamento das VAS (n = 7),laringoespasmo (n = 4) apnéia (n = 2), e depressão respiratória(n = 1) 3) Emergência 17.2% 4) Tempo para recuperação 118 minutos
![Ketamina a. Dissociativa [Ann Emerg Med, (5): p ]](http://slideplayer.com.br/slide/1226839/3/images/28/Ketamina+a.+Dissociativa+%5BAnn+Emerg+Med%2C+%285%29%3A+p+%5D.jpg "b. Analgesia, Sedação, Amnésia, Broncodilatação. c. Ketamina Oral a 10mg/kg[Pediatr Emerg Care, (2): p. 93-7] 1) 2/15 vomitaram. 2) Início da sedação em 35 minutos. d. Ketamine IV [Ann Emerg Med, (3): p ] 1) Início da sedação em 60 segundos[Crit Care Med, (6): p ] - 13 minutos. 2) Eventos adversos VAS/Desat. 2%,4.5%, [Ann Emerg Med, (6): p ] 11%[Pediatrics, (4): p. e ] 3) Emergência 6 – 15% 4) Recuperação 50,[Crit Care Med, 2002 ] 64 minutos[. Ann Emerg Med, 2000 ] – 85min[Pediatrics, (4): p. e ] 5) Uso de analgésicos previamente pode retardar a recuperação. [Pediatr Emerg Care, (2): p ] e. Ketamine IM a 4 -5 mg/kg[Acad Emerg Med, (1): p ] 1) Início da sedação em 5 minutos. 2) De 431 pacientes no PS[Acad Emerg Med, 1999 ], desalinhamento das VAS. (n = 7),laringoespasmo (n = 4) apnéia (n = 2), e depressão respiratória(n = 1) 3) Emergência 17.2% 4) Tempo para recuperação 118 minutos.")
29
Potential of ketamine and midazolam, individually or in combination, to induce apoptotic neurodegeneration in the infant mouse brain Br J Pharmacol September; 146(2): 189–197 A análise quantitativa da caspase-3 demonstrou que a combinação entre midazolam e ketamina causou mais apoptose neuronal que as drogas isoladamente Em (a) no caudado-putamen, a combinação ketamina-midazolam produziu uma densidade de C3A de 35,7 e em (b) no córtex, a combinação produziu uma densidade de 16 mm²
: 189–197. A análise quantitativa da caspase-3. demonstrou que a combinação entre. midazolam e ketamina causou mais. apoptose neuronal que as drogas. isoladamente. Em (a) no caudado-putamen, a. combinação ketamina-midazolam. produziu uma densidade de C3A de 35,7. e em (b) no córtex, a combinação. produziu uma densidade de 16 mm².")
30
Coloração prata de De Olmos 7 horas após a infusão de salina ou ketamina 40 mg/kg
Após 7 horas da infusão, os neurônios que estão mortos ou morrendo estão impregnados pela prata, e revelam uma aparência condensada e fragmentada

31
Doppler ultrasound assessment of the effects of ketamine on neonatal cerebral circulation
“ketamina mantém a estabilidade hemodinâmica com mínimos efeitos sobre o fluxo sanguíneo cerebral em neonatos em ventilação mecânica” The effects of a single dose of 5 mg.kg-1 of ketamine administered intravenously to 10 critically ill preterm infants prior to epicutaneo-caval catheterization were analyzed using pulsed-wave Doppler ultrasound. The infants weighed between 670 and 1,885 g and their gestational ages ranged from 26 to 33 weeks. Arterial pressure (MAP), cardiac output (CO), transcutaneous oxygen pressure (TcPO2), transcutaneous carbon dioxide pressure (TcPCO2), end-diastolic velocity (EDV), peak systolic velocity (PSV), mean arterial velocity (MAV) of the cerebral anterior artery as well as Pourcelot's resistance index (PRI) were measured before and after injection of the drug. We observed a significant decrease in arterial pressure at 2 min after injection while heart rate and CO did not vary significantly. TcPO2 and TcPCO2, also remained unchanged throughout the period of measurement. EDV, PSV, and MAV did not vary significantly nor did PRI. As this drug provides major comfort to the baby during painful procedures and considerably facilitates difficult thin vessel catheterization, we believe that it may be used in such conditions. Anand KJS, Johnston CC, Oberlander T, Taddio A, Tutag-Lehr V, Walco GA. Analgesia and local anesthesia during invasive procedures in the neonate. Clin Ther. 2005;27 :844 –876 Berde CB, Jaksic T, Lynn AM, Maxwell LG, Soriano SG, Tibboel D. Anesthesia and analgesia during and after surgery in neonates. Clin Ther. 2005;27 :900 –92 Dev Pharmacol Ther. 1993;20 :9 –13
, cardiac output (CO), transcutaneous oxygen pressure (TcPO2), transcutaneous carbon dioxide pressure (TcPCO2), end-diastolic velocity (EDV), peak systolic velocity (PSV), mean arterial velocity (MAV) of the cerebral anterior artery as well as Pourcelot s resistance index (PRI) were measured before and after injection of the drug. We observed a significant decrease in arterial pressure at 2 min after injection while heart rate and CO did not vary significantly. TcPO2 and TcPCO2, also remained unchanged throughout the period of measurement. EDV, PSV, and MAV did not vary significantly nor did PRI. As this drug provides major comfort to the baby during painful procedures and considerably facilitates difficult thin vessel catheterization, we believe that it may be used in such conditions. Anand KJS, Johnston CC, Oberlander T, Taddio A, Tutag-Lehr V, Walco GA. Analgesia and local anesthesia during invasive procedures. in the neonate. Clin Ther. 2005;27 :844 –876. Berde CB, Jaksic T, Lynn AM, Maxwell LG, Soriano SG, Tibboel D. Anesthesia and analgesia during and after surgery in neonates. Clin Ther. 2005;27 :900 –92. Dev Pharmacol Ther. 1993;20 :9 –13.")
32
Propofol Anestésico (hipnótico) intravenoso Antiemético Amnésia
Relaxamento muscular Não tem efeito analgésico

33
Doses de Propofol Pacientes Ambulatoriais Pacientes Hospitalizados p Indução (mg/kg) 2 ± 0,8 0,74 Total (mg/kg) 6,6 ± 2,3 7,9 ± 2,4 0,13 Hertzog et al, Pediatrics 2000
 6,6 ± 2,3. 7,9 ± 2,4. 0,13. Hertzog et al, Pediatrics")
34
Duração das Diferentes Fases dos Procedimentos
Tempo em Minutos Tempo de Indução 1,5 ± 0,7 Tempo de Procedimento 14,3 ± 11,3 Tempo de Recuperação 23,4 ± 11,5

35
Ocorrência de Efeitos Adversos com a Infusão de Propofol
Efeito Adverso Ocorrência % Hipotensão 64 Dessaturação 4 Obstrução das VAS 12 Apnéia 2 Mioclônus Dor à infusão 6

36
That´s all, Folks!

37
Apresentação: Cássio R. Borges, Flávia G. de Campos
Nota do Editor do site Dr. Paulo R. Margotto: Dor neonatal Humanização UTI Consultem: Comparação da Sedação entre Propofol e Pentobarbital/Midazolam/Fentanil para Ressonância Nuclear Magnética craniana em crianças Autor(es): Penshad J et al. Apresentação:Mariana Aires Vieira, Mariana Ribeiro de Siqueira, Marina Barichello Cerqueira, Paulo R. Margotto Comparação do uso do Propofol com Morfina/ Atropina e Succinilcolina como agentes indutores para entubação endotraqueal neonatal: ensaio randomizado e controlado Autor(es): Satish Ghanta et al. Apresentação:Lauro Francisco Felix Junior Analgesia e sedação no recém-nascido em ventilação mecânica (uso do propofol como premedicação na intubação endotraqueal neonatal não emergencial) Autor(es): Paulo R. Margotto Apresentação: Cássio R. Borges, Flávia G. de Campos
: Penshad J et al. Apresentação:Mariana Aires Vieira, Mariana Ribeiro de Siqueira, Marina Barichello Cerqueira, Paulo R. Margotto. Comparação do uso do Propofol com Morfina/ Atropina e Succinilcolina como agentes indutores para entubação endotraqueal neonatal: ensaio randomizado e controlado Autor(es): Satish Ghanta et al. Apresentação:Lauro Francisco Felix Junior. Analgesia e sedação no recém-nascido em ventilação mecânica (uso do propofol como premedicação na intubação endotraqueal neonatal não emergencial) Autor(es): Paulo R. Margotto. Apresentação: Cássio R. Borges, Flávia G. de Campos.")
38
DOR NEONATAL Autor(es): Paulo R. Margotto/Débora Nunes
Tese de Mestrado (Universidade de Brasília): A interferência do acompanhante no estresse de crianças internadas em Unidade de Terapia Intensiva Pediátrica Autor(es): Mércia Maria Fernandes de Lima Lira DOR NEONATAL Autor(es): Paulo R. Margotto/Débora Nunes
: A interferência do acompanhante no estresse de crianças internadas em Unidade de Terapia Intensiva Pediátrica Autor(es): Mércia Maria Fernandes de Lima Lira. DOR NEONATAL Autor(es): Paulo R. Margotto/Débora Nunes.")
Apresentações semelhantes

 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")









. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")
 Prognostic factors and survival in neonates with congenital.>")



 2.Comparação.>")



