Carregar apresentação
1
Dúvidas denucci@gilbertodenucci.com Arquivo Medicamentos utilizados no tratamento do diabetes mellitus Site www.gilbertodenucci.com Dúvidas denucci@gilbertodenucci.com Arquivo Medicamentos utilizados no tratamento do diabetes mellitus Site www.gilbertodenucci.com

2
Diabetes Mellitus Definição Doença em que o organismo não produz ou utiliza inadequadamente a insulina, o hormônio hipoglicemiante, o que leva a estado de hiperglicemia crônica

3
Guyton & Hall. Textbook of Medical Physiology. Tenth Edition. Glucose tolerance in normal person and in a person with diabetes

4
Principais tipos de Diabetes Mellitus Diabetes Mellitus tipo 1 (juvenil) O DM tipo 1 resulta primariamente da destruição das células pancreáticas tipo beta. Inclui casos decorrentes de doença auto-imune e aqueles nos quais a causa da destruição das células beta não é conhecida

5
Principais tipos de Diabetes Mellitus Diabetes Mellitus tipo 1 (juvenil) Corresponde a 5-10% do total de casos. A forma rapidamente progressiva é geralmente observada em crianças e adolescentes. A forma lentamente progressiva ocorre geralmente em adultos sendo referida como diabetes latente auto- imune do adulto (LADA)
.")
6
Principais tipos de Diabetes Mellitus Diabetes Mellitus tipo 2 (adulto) O DM tipo 2 resulta de graus variáveis de resistência à insulina e deficiência relativa de secreção de insulina. A maioria dos pacientes tem excesso de peso

7
Principais tipos de Diabetes Mellitus Diabetes Mellitus tipo 2 (adulto) Corresponde a 90-95% do total de casos. O diagnóstico é feito geralmente a partir dos 40 anos de idade embora possa ocorrer mais cedo principalmente em associação com a obesidade

8
Diabetes Mellitus tipo 1 x Diabetes Mellitus tipo 2 Tipo 1 Tipo 2 Início< 30 anos> 30 anos História familiar de Diabetes Mellitus Raro Comum Peso corporalNão obeso Obeso Cetoacidose ComumRaro Tratamento com insulina Todos pacientes Alguns pacientes Auto-imunidade SimNão Prevalência na população adulta 0.5% 5% Associação com HLA SimNão

9
Complicações comuns do diabetes tipo 2 Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

10
Intensive glycemic control and risk for microvascular complications Overview of insulin replacement therapy The Journal of Family Practice - August 2009 (Vol. 58, No. 8)
.")
11
Intensive glycemic control and risk for MI and microvascular complications Overview of insulin replacement therapy The Journal of Family Practice - August 2009 (Vol. 58, No. 8)
.")
12
Maiores reduções da HbA conferem maior proteção contra as complicações do diabetes Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

13
Insulina Proteína formada por 51 aminoácidos contidos no interior de 2 cadeias peptídicas: uma cadeia A com 21 aminoácidos e uma cadeia B com 30 aminoácidos As cadeias peptídicas são conectadas por duas pontes dissulfeto e, além disso, há uma outra ponte dissulfeto que liga as posições 6 e 11 da cadeia A

14
Insulina

15
= Carbono = Oxigênio = Nitrogênio, = Enxofre

16
A insulina tende a formar dímeros em solução e hexâmeros na presença do zinco Dímero Hexâmero Insulina

17
Site: http://www.nature.com/nrd/journal/v4/n5/images/nrd1718-f2.jpg Hexâmero Insulina

18
Protein Crystal Recombinant Human Insulin Site: http://mix.msfc.nasa.gov/IMAGES/HIGH/9802450.jpg

19
Insulina A insulina endógena circulante tem meia-vida de 3-5 minutos É catabolizada por insulinases no fígado, nos rins e na placenta sendo que cerca de 50% da insulina são removidos em uma única passagem pelo fígado

20
Insulina A insulina é sintetizada nas células pancreáticas tipo beta das ilhotas de Langerhans

21
Insulina Forma-se inicialmente um pré-pró-hormônio insulínico Este pré-pró-hormônio é clivado para formar uma pró- insulina que, em sua maior parte, é clivada adicionalmente liberando o peptídeo C para formar a insulina

22
Insulina Pró-insulina Insulina Peptídeo C livre Peptidases da célula pancreática tipo beta

23
Controle da liberação de insulina

24
Transportador de Glicose (1-5)
")
25
Transportadores da glicose em humanos GLUT-1 GLUT-3Todos os tecidos Captação basal de glicose GLUT-5 Intestino delgado e espermatozóides Transportador de frutose GLUT-2 GLUT-4Músculo esquelético e tecido adiposo Captação de glicose dependente de insulina Todos os tecidos Captação basal de glicose Fígado e células pancreáticas tipo beta Captação de glicose na hiperglicemia

26
Ação da Insulina Insulina Fusão Captação de glicose Translocação GLUT-4 Fosforilação

27
Effect of insulin in enhancing the concentration of glucose inside muscle cells Guyton & Hall. Textbook of Medical Physiology. Tenth Edition.

28
Schematic of the insulin receptor Guyton & Hall. Textbook of Medical Physiology. Tenth Edition.

29
The actions of insulin and glucagon in liver, muscle and adipose tissue on the overall flow of fuels http://www.ncbi.nlm.nih.gov/books/bv

30
Glucose O CO 2 + H 2 O Glucose O O Triglycerides Fatty acid Glycerol Glycogen Liver Glucose taken up by fat Glucose taken up by muscle Glucose oxidation Insulin permits rapid entry of glucose into muscle and fat cell Adipocyte Postpradial StatePostabsorbtive State Insulin Secretion Meal Insulin Insulin Secretion Glucose O O Circulation Glucose

31
Efeitos da insulina no metabolismo Carboidratos Aumenta o transporte de glicose Aumenta a síntese de glicogênio Inibe a glicogenólise Inibe a gliconeogênese Lipídeos Aumenta a atividade da lipoproteína lipase Aumenta o armazenamento de gordura nos adipócitos Aumenta a síntese de lipoproteínas no fígado Inibe a lipólise Inibe a oxidação de ácidos graxos Proteínas Aumenta o transporte de aminoácidos Aumenta a síntese de proteínas

32
Insulinas de Mamíferos

35
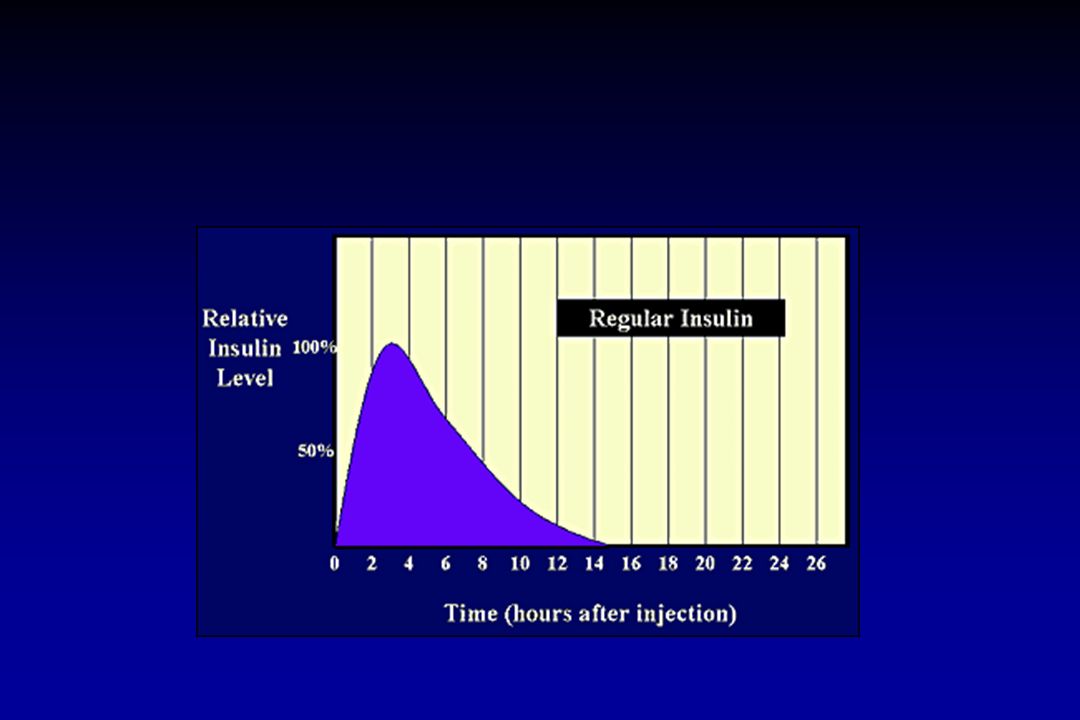
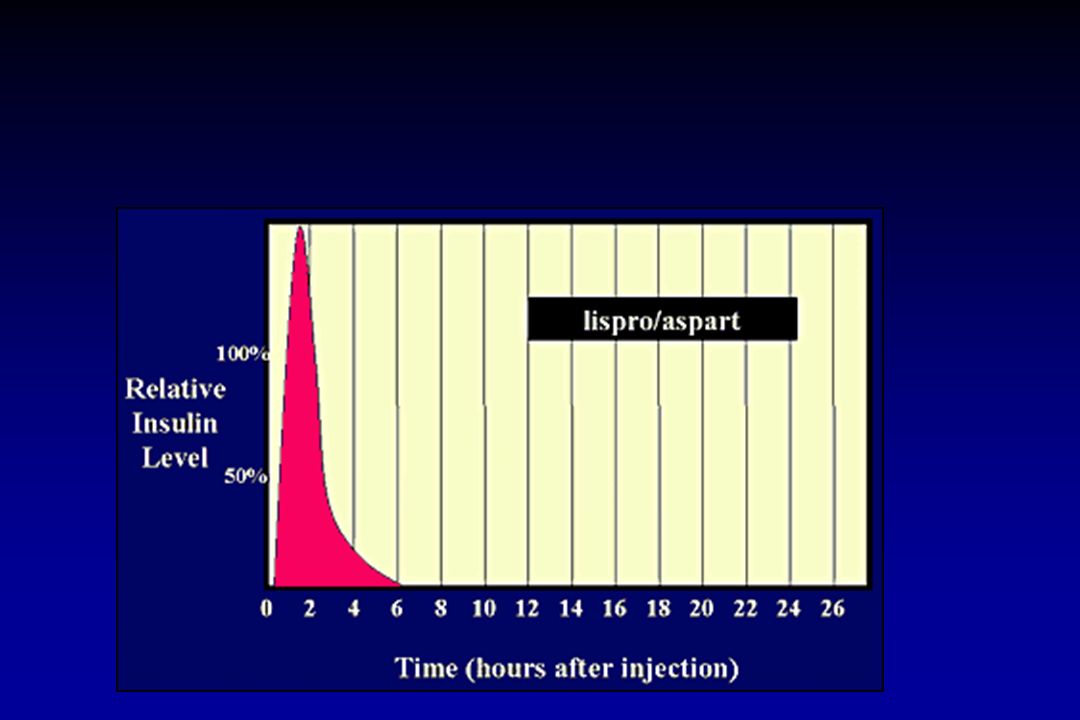
Rapid-acting analogue (clear) Onset: 10–15 min Peak: 60–90 min Duration: 4– 5 h Humalog® (insulin lispro) NovoRapid® (insulin aspart)
 Onset: 10–15 min Peak: 60–90 min Duration: 4– 5 h Humalog® (insulin lispro) NovoRapid® (insulin aspart)")
37
Insulin LisPro

38
Insulina Lispro e Aspart

39
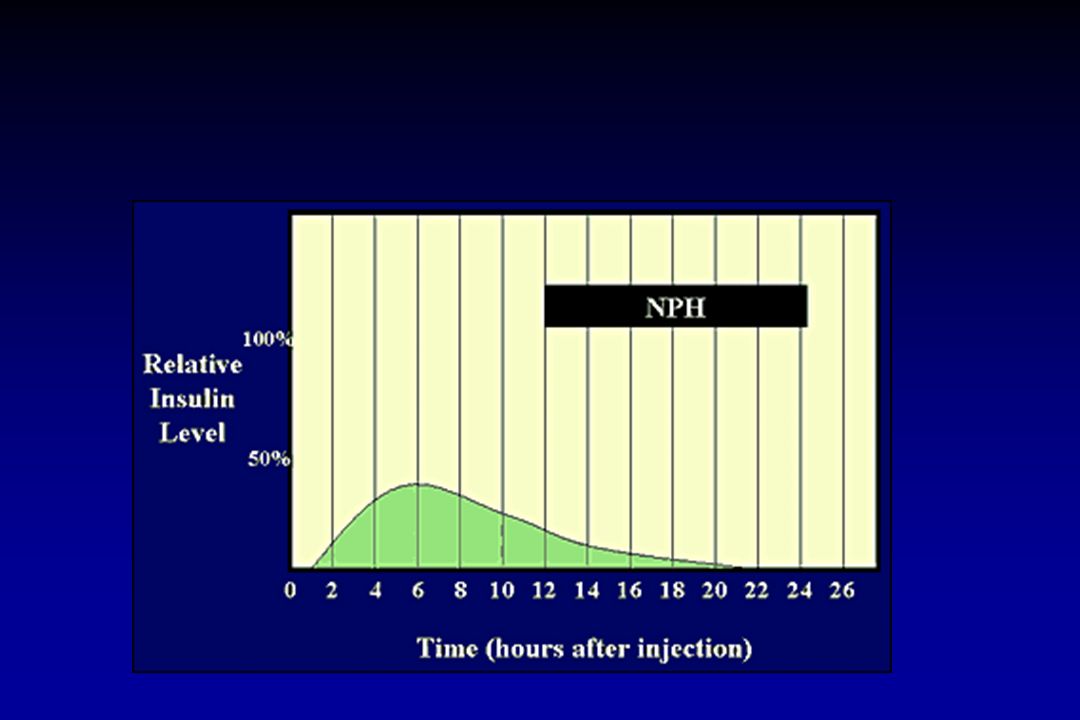
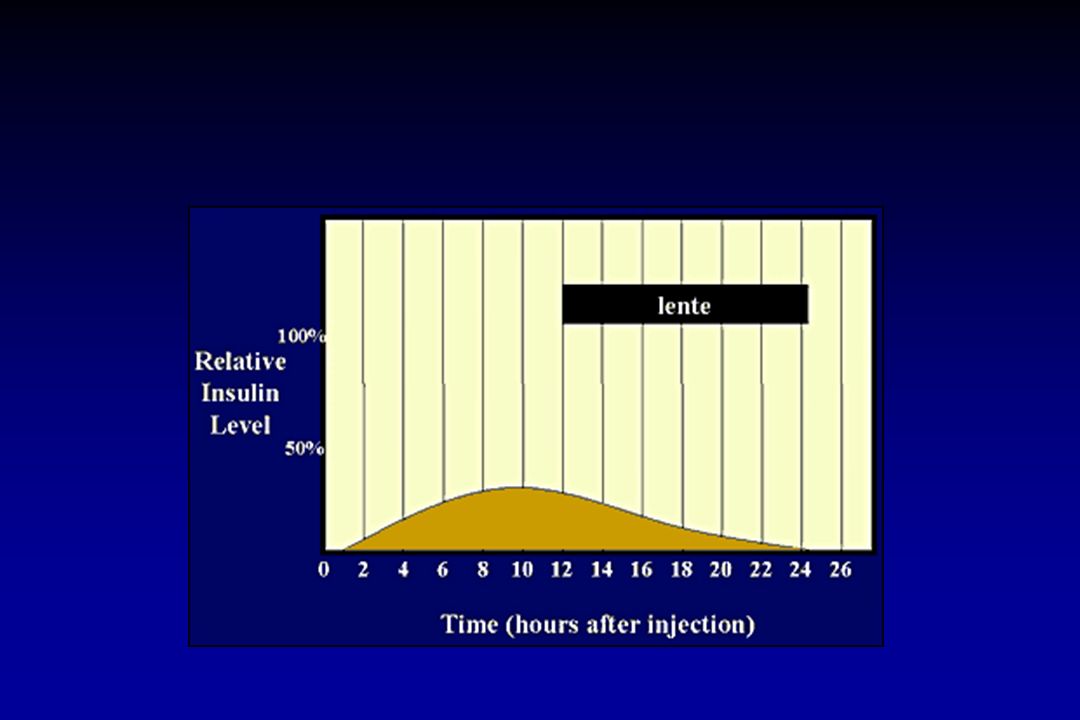
Intermediate-acting (cloudy) Onset: 1–3 h Peak: 5–8 h Duration: up to 18 h Humulin®-N Humulin®-L Novolin®ge NPH
 Onset: 1–3 h Peak: 5–8 h Duration: up to 18 h Humulin®-N Humulin®-L Novolin®ge NPH")
41
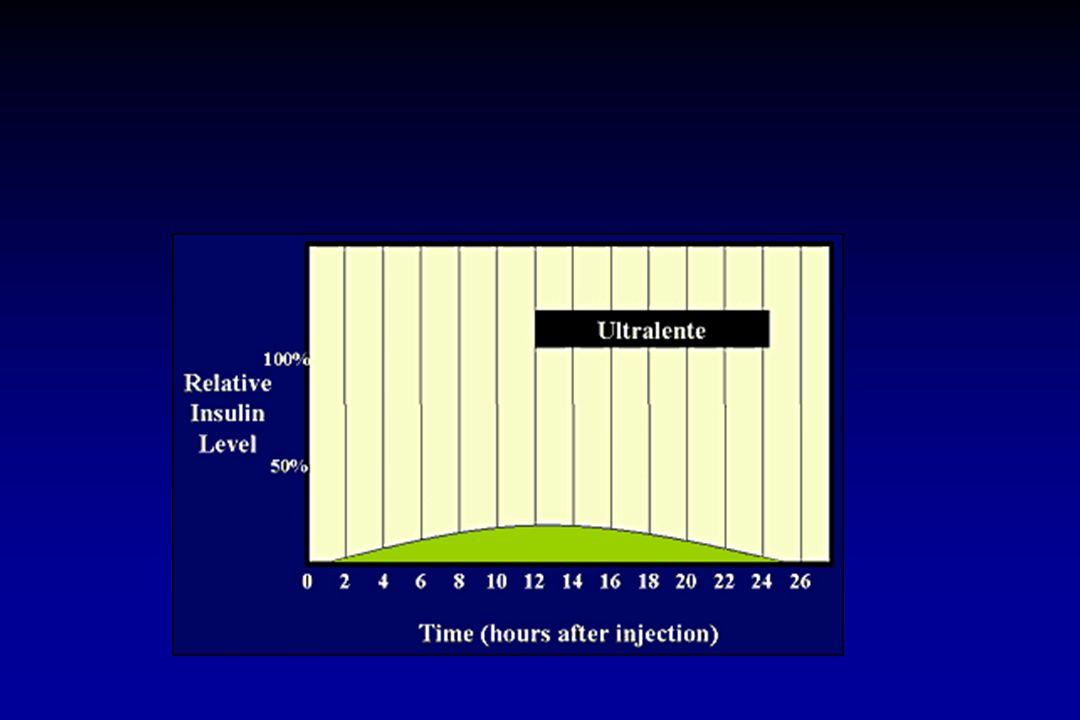
Long-acting (cloudy) Onset: 3–4 h Peak: 8–15 h Duration: 22–26 h Humulin®-U
 Onset: 3–4 h Peak: 8–15 h Duration: 22–26 h Humulin®-U")
43
Extended long-acting analogue Onset: 90 min Duration:24 h Lantus®* (insulin glargine)
")
44
Insulina Glarginina (Lantus)
")
45
Premixed (cloudy) A single vial contains a fixed ratio of insulin (% rapid- or fast-acting to % intermediate- acting insulin) Humalog® Mix25TM Humulin® (20/80, 30/70) Novolin®ge (10/90, 20/80, 30/70, 40/60, 50/50)
 A single vial contains a fixed ratio of insulin (% rapid- or fast-acting to % intermediate- acting insulin) Humalog® Mix25TM Humulin® (20/80, 30/70) Novolin®ge (10/90, 20/80, 30/70, 40/60, 50/50)")
46
40 30 20 10 0 Insulina plasmática em não diabéticos µU/mL 120 100 80 8am 10 12 2pm 4 6 8 10 12 2am 4 6 8am DesjejumAlmoço JantarLanche Glicemia em não diabéticos mg/dL Terapia com insulina

47
NPH + Regular Regime misto NPH Regular Ultralente + Regular Insulina Ultralente Regular Ultralente Terapia com insulina 8am 10 12 2pm 4 6 8 10 12 2am 4 6 8am

49
Pacientes em uso de CSII nos EUA 10.000 20.000 30.000 40.000 50.000 60.000 70.000 80.000 90.000 100.000 90 91 92 93 94 95 96 97 98 99 00 6.600 8.700 11.400 15.000 20.000 26.500 35.000 42.000 60.000 81.000 100.000 Número absoluto Ano

50
Autores n Idade média (anos ± DP) HbA 1c * pré- CSII (%) HbA 1c * pós- CSII (%) P Folow-up (meses) Bode (adultos) 14334 ± 138.287.46<0.00142 Bode (adolescentes) 5014.9 ± 2.69.648.24<0.00142 Rudolph and Hirsch 10736 ± 10.47.67.1<0.000136 Chanteleau 11629 ± 17.76.7<0.00154 Roland 2513.8 ± 2.18.47.50.0212 Controle de glicemia em uso de CSII * mg/dL
 HbA 1c * pré- CSII (%) HbA 1c * pós- CSII (%) P Folow-up (meses) Bode (adultos) ± < Bode (adolescentes) ± < Rudolph and Hirsch ± < Chanteleau ± < Roland ± Controle de glicemia em uso de CSII * mg/dL")
51
Adolescentes Adultos n = 50 n=413 Pré-CSII Pós-CSII 10 9 8 7 6 HbA1c (%) 9.64 8.248.28 7.46 * * * P < 0.001 Controle de glicemia: adolescentes x adultos
 * * * P < Controle de glicemia: adolescentes x adultos")
52
Hipoglicemia pré e pós CSII 0.01 7613413.8 ± 2.1 25 Roland 10ND29 ± 1 116 Chanteleau <0.0001 19.273.236 ± 10.4 107 Rudolph and Hirsch <0.0001 2213839.2 ± 12.9 55 Bode P Hipoglicemia pós-CSII (%) Hipoglicemia pré-CSII (%) Idade média (anos ± DP) nAutores ND – Não disponível
 Hipoglicemia pré-CSII (%) Idade média (anos ± DP) nAutores ND – Não disponível")
53
Hipoglicemia pré e pós CSII 0 50 100 150 138 22 26 39 36 Pré CSII 1 ano 2 anos 3 anos 4 anos -------------------CSII----------------

54
Pré-CSII Pós-CSII * P < 0.001 0 0,1 0,2 0,3 0,4 0,5 0,1 0,3 0,01 Adolescentes Adultos n = 43 n = 229 * Eventos por ano Redução no número de episódios de cetoacidose após uso de CSII

55
Endocr J. 2011 Aug 9. Effects of a novel short-term continuous subcutaneous insulin infusion program evaluated by continuous glucose monitoring on young adult type 1 diabetic patients in Taiwan. Lin CH, Huang CH, Tsai JS, Hsieh SH, Sun JH, Huang BY, Huang MJ, Huang YY. Source Division of Endocrinology and Metabolism, Department of Internal Medicine, Chang Gung Memorial Hospital and Chang Gung University, Taiwan. Abstract The aim of this study is to evaluate the effectiveness of blood sugar control by a short-course reinforcement program, consisting of using continuous subcutaneous insulin infusion (CSII) and continuous glucose monitoring (CGM) for young adult type 1 diabetic patients. Twenty-six pump-naïve type 1 diabetic patients were successively enrolled in two years. The mean disease duration was 13 years and the mean HbA1c was 8.8 %. Initially, a 3-day course of CGM was used to evaluate the baseline glycemic status of the subjects, followed by 6-day intensive insulin adjustment by CSII therapy. Thereafter, a second course of CGM was performed to evaluate the effectiveness of our outcomes in comparison to the initial measurements. All participants received necessary education and instruction as required throughout the course of the program. The glucose variability as measured by standard deviation of plasma glucose and mean amplitude of glucose excursion decreased significantly (67.8 ± 2.7 to 52.0 ± 1.8 mg/dL and 140.4 ± 6.5 to 105.5 ± 5.3 mg/dL, p < 0.001). The hypoglycemic events noted per patient were reduced by 46.4% (p = 0.003) and occurred significantly less often during nocturnal periods (-63.2%, p = 0.002). Following the adjustment, the mean daily insulin requirement was reduced by 28.05% (from 0.82 to 0.59 IU/kg) and the new proportion of 40% as basal insulin was found. The short-term CSII program provided significant improvement in blood sugar control for Type 1 diabetic patients, by reducing hypoglycemic events, glucose excursion, and insulin dosage in our examined subjects.
 and continuous glucose monitoring (CGM) for young adult type 1 diabetic patients. Twenty-six pump-naïve type 1 diabetic patients were successively enrolled in two years. The mean disease duration was 13 years and the mean HbA1c was 8.8 %. Initially, a 3-day course of CGM was used to evaluate the baseline glycemic status of the subjects, followed by 6-day intensive insulin adjustment by CSII therapy. Thereafter, a second course of CGM was performed to evaluate the effectiveness of our outcomes in comparison to the initial measurements. All participants received necessary education and instruction as required throughout the course of the program. The glucose variability as measured by standard deviation of plasma glucose and mean amplitude of glucose excursion decreased significantly (67.8 ± 2.7 to 52.0 ± 1.8 mg/dL and ± 6.5 to ± 5.3 mg/dL, p < 0.001). The hypoglycemic events noted per patient were reduced by 46.4% (p = 0.003) and occurred significantly less often during nocturnal periods (-63.2%, p = 0.002). Following the adjustment, the mean daily insulin requirement was reduced by 28.05% (from 0.82 to 0.59 IU/kg) and the new proportion of 40% as basal insulin was found. The short-term CSII program provided significant improvement in blood sugar control for Type 1 diabetic patients, by reducing hypoglycemic events, glucose excursion, and insulin dosage in our examined subjects..")
56
Inhaled Insulin Device. The Exubera inhaled insulin device is closed for portability and opened before use. It is activated after insertion of an insulin blister. The release unit must be changed every 2 weeks.

57
Exubera

58
Sulfoniluréias Sulfoniluréias (clorpropamida, glibenclamida, glipizida, gliclazida e glimepirida) Estimulam a secreção de insulina ligando-se a um receptor específico na célula beta o qual determina o fechamento dos canais de potássio dependentes de ATP resultando em despolarização da célula
 Estimulam a secreção de insulina ligando-se a um receptor específico na célula beta o qual determina o fechamento dos canais de potássio dependentes de ATP resultando em despolarização da célula")
59
Controle da liberação de insulina

60
Chlorpropamide (t ½ = 36 h) (1 st generation) Site: http://en.wikipedia.org/wiki/File:Chlorpropamide.svg
 (1 st generation) Site:")
61
Gliclazide (1 st generation) Site: http://en.wikipedia.org/wiki/File:Gliclazide.svg
 Site:")
62
Tolbutamide (1 st generation) Site: http://en.wikipedia.org/wiki/File:Tolbutamide.svg
 Site:")
63
Glibenclamide (t ½ = 10h) (2 st generation) Site: http://en.wikipedia.org/wiki/File:Glibenclamide.svg
 (2 st generation) Site:")
64
Glipizide ( t ½ = 2-4 hs) (2 st generation) Site: http://en.wikipedia.org/wiki/File:Glipizide.svg
 (2 st generation) Site:")
65
Glimepiride (t ½ = 5 h) (3 st generation) Site: http://en.wikipedia.org/wiki/File:Glimepiride.svg
 (3 st generation) Site:")
66
Meglitinidas Derivados do ácido benzóico (repaglinida) Derivados da d-fenilalanina (nateglinida) Estimulam a secreção de insulina ligando-se a receptores na célula beta em sítios distintos dos canais de potássio dependentes de ATP.
 Derivados da d-fenilalanina (nateglinida) Estimulam a secreção de insulina ligando-se a receptores na célula beta em sítios distintos dos canais de potássio dependentes de ATP.")
67
Controle da liberação de insulina

68
Repaglinide

69
Nateglinide

70
Glucose Glucose-PO 4 Pyruvic acid Lactic acid Lipogenesis Krebs cycle Inhibition of oxidative metabolism Blood insulin Blood glucose (nondiabetic) Blood glucose (diabetic) Administration Blood Glucose, mg/100ml 200 100 Insulin Microunits/ml 15 Hours 0 1 2 3 Metformin Suggested mode action: Reduces hepatic glucose production and glycogen metabolism Improves insulin resistance via enhancing insulin-mediated glucose uptake by skeletal muscle Lowers triglycerides and total cholesterol levels Raises high-density lipoprotein (HDL) levels and causes weight loss Helpful in stabilizing blood sugar in brittle diabetics on insulin therapy Indicated alone in obese, mild diabetics because, unlike insulin, it does not enhance lipogenesis Biguanides
 Blood glucose (diabetic) Administration Blood Glucose, mg/100ml Insulin Microunits/ml 15 Hours Metformin Suggested mode action: Reduces hepatic glucose production and glycogen metabolism Improves insulin resistance via enhancing insulin-mediated glucose uptake by skeletal muscle Lowers triglycerides and total cholesterol levels Raises high-density lipoprotein (HDL) levels and causes weight loss Helpful in stabilizing blood sugar in brittle diabetics on insulin therapy Indicated alone in obese, mild diabetics because, unlike insulin, it does not enhance lipogenesis Biguanides")
71
Metformin

74
Tiazolidinedionas Rosiglitazona Pioglitazona

75
Thiazolidinedione Site: http://en.wikipedia.org/wiki/File:Thiazolidinedione.png

76
Rosiglitazone Site: http://www.3dchem.com/imagesofmolecules/Rosiglitazone.gif

77
Pioglitazone Site: http://www.dalton.com/images/pioglitazone.gif

78
Tiazolidinedionas Reduz glicose plasmática Aumenta uptake periférico de glicose Reduz níveis de triglicerídeos Aumenta a sensibilidade à insulina em tecidos periféricos

79
Peroxisome proliferator-activated receptor (PPAR) α (alpha) - liver, kidney, heart, muscle, adipose tissue and others β/δ (beta/delta) - expressed in many tissues but markedly in brain, adipose tissue and skin γ (gamma) - although transcribed by the same gene, this PPAR through alternative splicing is expressed in three forms: γ1 - expressed in virtually all tissues, including heart, muscle, colon, kidney, pancreas, and spleen γ2 - expressed mainly in adipose tissue (30 amino acids longer) γ3 - expressed in macrophages, large intestine, white adipos tissue.
 α (alpha) - liver, kidney, heart, muscle, adipose tissue and others β/δ (beta/delta) - expressed in many tissues but markedly in brain, adipose tissue and skin γ (gamma) - although transcribed by the same gene, this PPAR through alternative splicing is expressed in three forms: γ1 - expressed in virtually all tissues, including heart, muscle, colon, kidney, pancreas, and spleen γ2 - expressed mainly in adipose tissue (30 amino acids longer) γ3 - expressed in macrophages, large intestine, white adipos tissue.")
80
Alternative splicing resulting in protein isoforms Site: http://en.wikipedia.org/wiki/File:Splicing_overview.jpg

81
Peroxisome proliferator - activated receptor pathway diagram Site: http://en.wikipedia.org/wiki/File:PPAR-diagram.png

82
Thiazolidinediones

83
Effect of rosiglitazone and metformin on subcutaneous abdominal adipose tissue (SCAAT) and visceral adipose tissue Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280
 and visceral adipose tissue Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280")
85
Bioactive GLP-1(7-36)amide and GIP (1-42) are released from the small intestine after meal ingestion and enhance glucose stimulated insulin secretion (incretin action). DPP-4 rapidly converts GLP-1 and GIP to their inactive metabolites GLP-1 (9-36) and GIP (3-42) in vivo. Inhibition of DPP-4 activity prevents GLP-1 and GIP degradation, thereby enhancing incretin action. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157
 and GIP (3-42) in vivo. Inhibition of DPP-4 activity prevents GLP-1 and GIP degradation, thereby enhancing incretin action. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157.")
86
GIP actions in peripheral tissues. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157

87
Exenatide (Byetta) 53% idêntico ao GLP-1 Resistente a DPP-IV Aumenta a secreção de insulina Reduz a secreção de glucagon Aumenta o tempo de esvaziamento gástrico Sensação de saciedade – provoca queda de peso
 53% idêntico ao GLP-1 Resistente a DPP-IV Aumenta a secreção de insulina Reduz a secreção de glucagon Aumenta o tempo de esvaziamento gástrico Sensação de saciedade – provoca queda de peso")
88
GLP-1 actions in peripheral tissues. The majority of the effects of GLP-1 are mediated by direct interaction with GLP-1Rs on specific tissues. However, the actions of GLP-1 in liver, fat, and muscle most likely occur through indirect mechanisms. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157

89
The inactivation process of GLP-1 by DPP-IV. GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081.")
90
Saxagliptin Site: http://en.wikipedia.org/wiki/File:Saxagliptin.svg

91
Sitagliptin Site: http://en.wikipedia.org/wiki/File:Sitagliptin.svg

92
Vildagliptin Site: http://en.wikipedia.org/wiki/File:Vildagliptin_Structural_Formulae.png

93
Mechanism of action of vildagliptin. In response to a meal, active glucagonlike peptide-1 (GLP-1) is secreted by the L cells of the intestines. Without the presence of vildagliptin, GLP-1 is rapidly inactivated and degraded by the enzyme dipeptidyl peptidase IV (DPP4); when vildagliptin is present, vildagliptin binds to DPP4, allowing GLP-1 to remain active. Active GLP-1 causes the pancreas to increase insulin release and decrease glucagon release. Vildagliptin: A novel oral therapy for type 2 diabetes mellitus - Am J Health-Syst PharmVol 64 Jun 15, 2007
 is secreted by the L cells of the intestines. Without the presence of vildagliptin, GLP-1 is rapidly inactivated and degraded by the enzyme dipeptidyl peptidase IV (DPP4); when vildagliptin is present, vildagliptin binds to DPP4, allowing GLP-1 to remain active. Active GLP-1 causes the pancreas to increase insulin release and decrease glucagon release. Vildagliptin: A novel oral therapy for type 2 diabetes mellitus - Am J Health-Syst PharmVol 64 Jun 15,")
94
Target 2 physiologic glucose-lowering actions with a single oral agent Glucose-dependent mechanism target 2 key defects: insulin release and hepatic glucose production Site: www.januvia.com

95
Rapidly increased active incretins (GLP-1 and GIP) through a full 24 hours In a single-dose pharmacokinetic study of patients with type 2 diabetes Site: www.januvia.com
 through a full 24 hours In a single-dose pharmacokinetic study of patients with type 2 diabetes Site:")
96
A single oral dose sustains powerful DPP-4 inhibition for a full 24 hours Site: www.januvia.com

97
Significantly improved key meassures of beta-cell and alpha-cell responsiveness to glucose Site: www.januvia.com

99
Amylin 37 amino acid compound Co-secreted with insulin from beta cells Deficient in type 1 and type 2 DM Renal clearance

100
Amylin - Physiological effects 1. Suppression of endogenous glucagon production (especially in the postprandial state) 2. Reduction in postprandial hepatic glucose production 3. Reduction in gastric emptying time 4. Centrally mediated induction of satiety 5. Reduction in postprandial glucose levels
 2. Reduction in postprandial hepatic glucose production 3. Reduction in gastric emptying time 4. Centrally mediated induction of satiety 5. Reduction in postprandial glucose levels.")
101
Pramlintide Synthetic analogue of Amylin (3 amino acid substitutions with proline for native amino acids) Subcutaneous administration
 Subcutaneous administration")
102
Pramlintide The most commonly reported adverse effects associated with pramlintide use in type 1 DM were nausea, anorexia, and hypoglycemia in these studies.

103
Mean percent changes in lipid values in 203 type 2 diabetic patients on placebo and 3 different doses of pramlintide for 4 weeks. Byron J Hoogwerf, Krupa B Doshi, Dima Diab Pramlintide, the synthetic analogue of amylin: physiology, pathophysiology, and effects on glycemic control, body weight, and selected biomarkers of vascular risk. Vascular Health and Risk Management 2008:4(2) 355–362
 355–362.")
105
Diabetic Neuropathy 1 - accumulation of advanced glycation end products 2 - formation of reactive oxygen species 3 - activation of protein kinase C, development of diabetic microangiopathy (disease of the small blood vessels) 4 - increased aldose reductase activity
 4 - increased aldose reductase activity")
106
The Polyol Pathway Site: http://www.medbio.info/images/Time%203-4/new_se11.gif

107
Epalrestat

109
SGLT2 mediates glucose reabsorption in the kidney. SGLT2 catalyzes the active transport of glucose (against a concentration gradient) across the luminal membrane by coupling it with the downhill transport of Na+. The inward Na+ gradient across the luminal epithelium is maintained by active extrusion of Na+ (driven by ATP) across the basolateral surface into the intercellular fluid, which is in equilibrium with the blood. Glucose passively diffuses of the cell down a concentration gradient via basolateral facilitative transporters, GLUT2 (and GLUT1). A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - Figure 1.
 across the luminal membrane by coupling it with the downhill transport of Na+. The inward Na+ gradient across the luminal epithelium is maintained by active extrusion of Na+ (driven by ATP) across the basolateral surface into the intercellular fluid, which is in equilibrium with the blood. Glucose passively diffuses of the cell down a concentration gradient via basolateral facilitative transporters, GLUT2 (and GLUT1). A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - Figure 1..")
110
Comparison of sodium-Glucose Contransporters A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - tab 01

111
Normal glucose homeostasis. Diagram outlining the hormonal interactions that are important in regulating normal glucose homeostasis. Normal fasting glucose homeostasis involves the hormonal regulation of glucose utilization and production, as well as the filtration and reabsorption of glucose by the kidney. Under basal conditions, glucose uptake by the tissues is matched by glucose production from the liver; this enables fine regulation of glucose at a very fixed level. Gluconeogenesis in the liver helps prevent hypoglycemia. Adapted from DeFronzo RA. Pharmacologic therapy for type 2 diabetes mellitus. A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - Ann Intern Med 131(4):281-303, 1999 – fig 02
: , 1999 – fig 02.")
112
Renal glucose handling before and following inhibition of SGLT2. With gradual infusion of glucose, as the plasma glucose concentration increases, the reabsorption progressively increases following the line marked reabsorption curve (in red). At plasma glucose concentrations <200 mg/dL, all the filtered glucose is reabsorbed and there is no excretion. When glucose reaches a threshold, around 200-250 mg/dL, the maximum capacity of the renal tubule to reabsorb glucose -- or the T max - is exceeded and once it passes this, glucose begins to be excreted into the urine (green line, labeled excretion). The breaking point, however, is not abrupt -- splay, which represents glucose excretion in the urine before saturation (T max ) is fully attained; and is explained by some nephrons releasing glucose at a slightly lower threshold, some a bit higher; and the relatively low affinity of the Na-glucose carriers. The dotted yellow lines depict renal glucose handling after SGLT2 inhibition. The SGLT2 inhibitors lower the T max of glucose, which in turn increases the excretion of glucose via the kidneys A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - Figure 4.
. At plasma glucose concentrations <200 mg/dL, all the filtered glucose is reabsorbed and there is no excretion. When glucose reaches a threshold, around mg/dL, the maximum capacity of the renal tubule to reabsorb glucose -- or the T max - is exceeded and once it passes this, glucose begins to be excreted into the urine (green line, labeled excretion). The breaking point, however, is not abrupt -- splay, which represents glucose excretion in the urine before saturation (T max ) is fully attained; and is explained by some nephrons releasing glucose at a slightly lower threshold, some a bit higher; and the relatively low affinity of the Na-glucose carriers. The dotted yellow lines depict renal glucose handling after SGLT2 inhibition. The SGLT2 inhibitors lower the T max of glucose, which in turn increases the excretion of glucose via the kidneys A Paradigm Shift in Diabetes Therapy Dapagliflozin and Other SGLT2 Inhibitors - Figure 4..")
113
Acarbose É um inibidor competitivo de α-glicosidases intestinais tais como maltase, isomaltase, sacarase e glicoamilase, retardando a absorção de carboidratos

115
Activation and inactivation of poly(ADP-ribose) polymerase (PARP): interactions with specific signal-transduction pathways Site: http://www.nature.com/nrd/journal/v4/n5/images/nrd1718-f2.jpg
 polymerase (PARP): interactions with specific signal-transduction pathways Site:")
116
Insulina Canal de potássio dependente de ATP, sensível à gliburida K+K+ Ca 2+ Insulina Liberação de insulina Exocitose Retículo endoplasmático ATP Célula pancreática tipo beta estimulada por glicose

118
Significantly improved measures of insulin synthesis and release from the beta cell Site: www.januvia.com

119
Structures of (A) the proglucagon gene, (B) mRNA, and (C) protein. (D) Tissue-specific posttranslational processing of proglucagon in the pancreas leads to the generation of Glicentin- related polypeptide (GRPP), glucagon (GLUC), intervening peptide-1 (IP-1), and major proglucagon fragment (MPGF), whereas glicentin, oxyntomodulin (OXM), intervening peptide-2 (IP-2), and GLP-1 and GLP-2 are liberated after proglucagon processing in the intestine and brain. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157
 Tissue-specific posttranslational processing of proglucagon in the pancreas leads to the generation of Glicentin- related polypeptide (GRPP), glucagon (GLUC), intervening peptide-1 (IP-1), and major proglucagon fragment (MPGF), whereas glicentin, oxyntomodulin (OXM), intervening peptide-2 (IP-2), and GLP-1 and GLP-2 are liberated after proglucagon processing in the intestine and brain. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157.")
120
(A) ProGIP gene, (B) mRNA, and (C) protein. Bioactive GIP is generated from its proGIP protein precursor by posttranslational cleavage at single arginine residues that flank GIP. Biology of Incretins: GLP-1 and GIP - GASTROENTEROLOGY 2007;132:2131–2157

121
01 - Structure of the primary transcript of RNA 02 -Mature messenger (m) RNA after exicision of the introns 03 - Structure of proinsulin after cleavage of the signal sequence from pre-proinsulin 04 - Cleavage of the C peptide leaving biologically active insulin 05 - Packaging of insulin and C-peptide in secretory granules for storage and release Structure, synthesis and metabolism of insulin and glucagon http://www.ncbi.nlm.nih.gov/books/bv
 RNA after exicision of the introns 03 - Structure of proinsulin after cleavage of the signal sequence from pre-proinsulin 04 - Cleavage of the C peptide leaving biologically active insulin 05 - Packaging of insulin and C-peptide in secretory granules for storage and release Structure, synthesis and metabolism of insulin and glucagon")
122
Schematic representation of the major products of proglucagon in the human pancreas and intestine. The processing of glucagon in the gut produces two important peptides - glucagon-like peptide 1 (GLP-1) and oxyntomodulin - which are known as incretins as they increase the insulin response to glucose. GRPP, glucagon related pancreatic peptide; IP, intervening peptide Synthesis of glucagon and post-translational processing of the proglucagon gene http://www.ncbi.nlm.nih.gov/books/bv
 and oxyntomodulin - which are known as incretins as they increase the insulin response to glucose. GRPP, glucagon related pancreatic peptide; IP, intervening peptide Synthesis of glucagon and post-translational processing of the proglucagon gene")
123
Ação da insulina Domínio intra- citoplasmático COOH Estrutura do receptor de insulina Receptor de insulina Cascata de fosforilações (GLUT- 4, transferrina, LDL-R e IGF 2-R) COOH NH 2 β β Domínio de ligação da insulina Insulina Receptor de insulina ativado (ação tirosina- quinase intrínseca)
 COOH NH 2 β β Domínio de ligação da insulina Insulina Receptor de insulina ativado (ação tirosina- quinase intrínseca)")
124
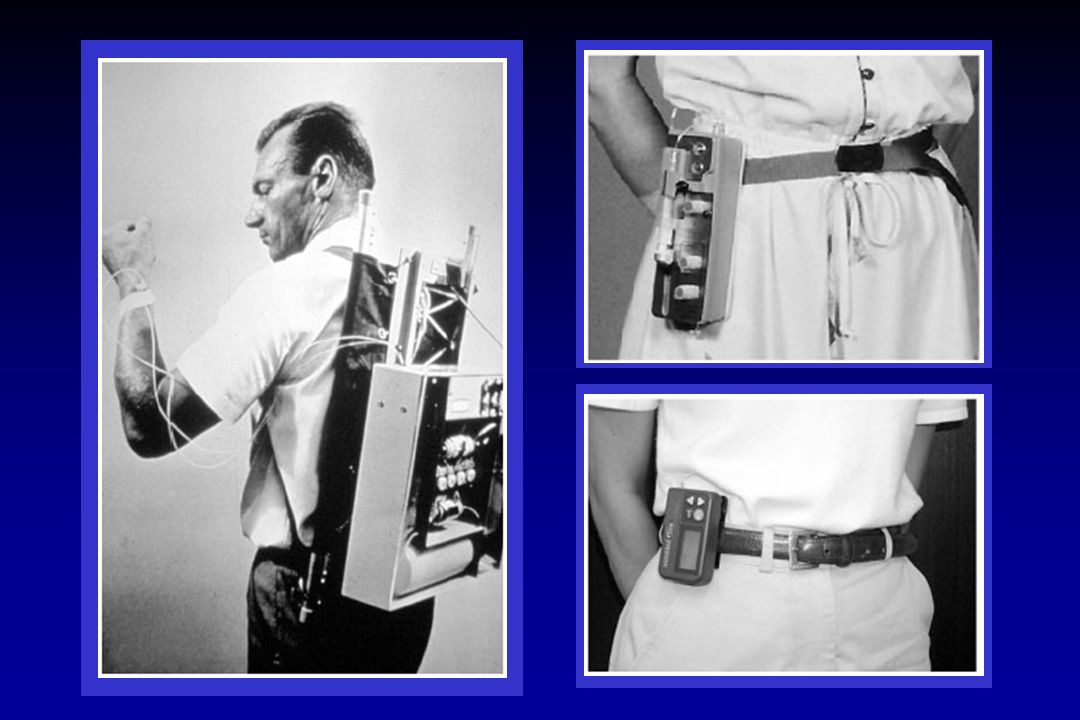
Tratamento do Diabetes Mellitus Nova modalidade de tratamento CSII (Continuous subcutaneous insulin infusion) Terapia que utiliza bomba de infusão subcutânea contínua de insulina indicada quando 3 ou 4 aplicações diárias ainda são insuficientes para o controle da glicemia Também indicada para pacientes motivados com cotidiano que não permite a terapia convencional com auto-aplicações de insulina
 Terapia que utiliza bomba de infusão subcutânea contínua de insulina indicada quando 3 ou 4 aplicações diárias ainda são insuficientes para o controle da glicemia Também indicada para pacientes motivados com cotidiano que não permite a terapia convencional com auto-aplicações de insulina")
125
Tratamento do Diabetes Mellitus Objetivo Glicemia de jejum em torno de 110 mg/dL Glicemia após 2 h de refeição em torno de 140 mg/dL

126
Glucose O CO 2 + H 2 O Glucose O O Triglycerides Fatty acid Glycerol Glycogen Liver Glucose taken up by muscle Glucose oxidation Adipocyte Muscle Thiazolidinediones: Clinical Rationale and Adverse Effects Glucose O O Hepatic glucose production reduced Glycogenolysis Reduced triglycerides increased HDL and LDL Thiazolidinediones increase sensitivity of cells to existing insulin Rosiglitazone

127
Navigation About this bookThe endocrine pancreasGlucose turnoverAnabolic and catabolic phases of glucose metabolismActions of insulin and glucagonLipid metabolism - insulinopenia and diabetic ketosisProtein metabolism and the anabolic actions of insulinDefinition and diagnosis of diabetes mellitusEtiology of type 1 DMPrevention of type 1 DMStructure, synthesis and metabolism of insulin and glucagon Anatomical features of pancreatic islets in relation to hormone secretion and its control Control of insulin and glucagon secretionType 2 DMCauses of DMGenetic disorders of β-cell functionCounter-regulatory hormones and DMComplications of DMMacrovascular circulatory changesMicrovascular changes - diabetic retinopathy, nephropathy and neuropathyDiabetes and the neuropathic footDiabetes and insulin resistance of pregnancyDevelopment of the pancreas: effects of DM on organogenesisTreatment of DM - rationale and practical considerationsHypoglycemiaPhysiological responses to hypoglycemia and its treatmentHypoglycemia and insulinomaHypoglycemia in infancyDisorders of the α, γ and PP cells of the islets Clinical case questions Search

128
Adverse reactions reported in 5.0% of patients and more commonly than in patients given placebo, regardless of investigator assessment of causality, number of patients(%) Site: www.januvia.com
 Site:")
129
Proven 24-hours glycemic control Dosage for patients with renal insufficency Site: www.januvia.com

130
Fatores de risco para o desenvolvimento de doença coronariana nos pacientes com diabetes tipo 2 Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

131
Relação contínua entre os níveis de HbA após o tratamento do diabetes e a incidência de complicações do diabetes Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

132
Taxas constantemente baixas de controle glicêmico em pacientes tratados na comunidade Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

133
O desenvolvimento de resistência à insulina e o comprometimento relativo da secreção de insulina fazem parte da progressão do diabetes tipo 2 Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

134
Estratégia para o controle mais intensivo do diabetes, como uso mais precoce do tratamento combinado Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

135
Propriedades farmacocinéticas de Glucovance e da associação livre de metformina e glibenclamida Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

136
Esquema terapêutico diário de um paciente que apresenta diabetes tipo 2 e doenças concomitantes típicas. Este paciente precisa tomar um total de 19 comprimidos por dia, em quatro horários diferentes. Monografia de Glucovance – Site: http://www.merck.com.br/pdf/glucovance_monografia.pdf

137
Selective insulin resistance in T2DM. In skeletal muscle, insulin action on glucose transport and utilisation is impaired due to decreased IRS tyrosine phosphorylation and activity of the kinases PI 3- kinase and Akt. In endothelial cells (EC), the defect in insulin-stimulated PI 3-kinase/Akt activity is also responsible for reduced eNOS synthesis and nitric oxide (NO) generation, which contributes to endothelial dysfunction. The defective glucose metabolism leads to increased insulin concentrations (hyperinsulinaemia), which stimulate the Shc/MAP kinase pathway normally or more effectively than normal in vascular smooth muscle cells (VSMC), leading to increased secretion of plasminogen activator inhibitor-1 (PAI-1) and endothelin-1 (ET-1), which further exacerbate endothelial dysfunction. PY, tyrosine phosphorylation; eNOS, endothelial nitric oxide synthase. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract. 2005 Jun;68 Suppl1:S22-9.
, the defect in insulin-stimulated PI 3-kinase/Akt activity is also responsible for reduced eNOS synthesis and nitric oxide (NO) generation, which contributes to endothelial dysfunction. The defective glucose metabolism leads to increased insulin concentrations (hyperinsulinaemia), which stimulate the Shc/MAP kinase pathway normally or more effectively than normal in vascular smooth muscle cells (VSMC), leading to increased secretion of plasminogen activator inhibitor-1 (PAI-1) and endothelin-1 (ET-1), which further exacerbate endothelial dysfunction. PY, tyrosine phosphorylation; eNOS, endothelial nitric oxide synthase. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract Jun;68 Suppl1:S")
138
Mechanisms of action of thiazolidinediones (TZDs). The TZDs act by binding to the nuclear receptor peroxisome proliferator activated receptors-γ (PPARγ), thereby inducing expression of genes involved in glucose and lipid metabolism in adipocytes, as well as secretion of the adipokines adiponectin and tumor necrosis factor (TNF)-α. In addition, the TZDs inhibit hepatic gluconeogenesis, stimulate lipid uptake and oxidation by the liver, and promote glucose oxidation by the skeletal muscle. The ultimate effects are to lower circulating FFA and enhance whole-body insulin sensitivity. GLUT4, insulin-stimulated glucose transporter; CAP, cbl-associated protein involved in insulin signaling; LPL, lipoprotein lipase; FATP, fatty acid transport protein; ACS, acetyl CoA synthase; UCP, uncoupling protein; FFA, free fatty acid; PEPCK, phosphoenolpyruvate carboxykinase. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract. 2005 Jun;68 Suppl1:S22-9.
, thereby inducing expression of genes involved in glucose and lipid metabolism in adipocytes, as well as secretion of the adipokines adiponectin and tumor necrosis factor (TNF)-α. In addition, the TZDs inhibit hepatic gluconeogenesis, stimulate lipid uptake and oxidation by the liver, and promote glucose oxidation by the skeletal muscle. The ultimate effects are to lower circulating FFA and enhance whole-body insulin sensitivity. GLUT4, insulin-stimulated glucose transporter; CAP, cbl-associated protein involved in insulin signaling; LPL, lipoprotein lipase; FATP, fatty acid transport protein; ACS, acetyl CoA synthase; UCP, uncoupling protein; FFA, free fatty acid; PEPCK, phosphoenolpyruvate carboxykinase. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract Jun;68 Suppl1:S")
139
Potential mechanisms leading to β-cell dysfunction in T2DM. Potential Causes of β-Cell Dysfunction in Type 2 Diabetes SUR1/Kir6, complex formed by the sulphonylureas receptor (SUR) and the K+ channel; IPF-1, insulin promoter factor-1; HNF, hepatocyte nuclear factor; IRS-1, insulin receptor substrate-1. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract. 2005 Jun;68 Suppl1:S22-9. Reversible metabolic abnormalities Glucotoxicity Lipotoxicity Hormonal changes Inadequate incretin action Increased glucagon secretion Genetic abnormalities of β-cell proteins Glucokinase, SUR1/Kir6, IPF-1, HNF-4α, HNF-2α, Insulin receptor, IRS-1 Reduction of β-cell mass Increase in amyloid Apoptosis
 and the K+ channel; IPF-1, insulin promoter factor-1; HNF, hepatocyte nuclear factor; IRS-1, insulin receptor substrate-1. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract Jun;68 Suppl1:S22-9. Reversible metabolic abnormalities Glucotoxicity Lipotoxicity Hormonal changes Inadequate incretin action Increased glucagon secretion Genetic abnormalities of β-cell proteins Glucokinase, SUR1/Kir6, IPF-1, HNF-4α, HNF-2α, Insulin receptor, IRS-1 Reduction of β-cell mass Increase in amyloid Apoptosis.")
140
Schematic flow-chart of the use of hypoglycaemic drugs in the therapy of T2DM. When diet and physical activity fail to achieve an HbA1c value of <7%, insulin-sensitizing agents and insulin secretagogues are used alone or in various combinations. If the HbA1c target of <7% is still not met, insulin therapy should be considered. A basal insulin, such as NPH insulin or glargine, is used to lower fasting plasma glucose (FPG) below 100 mg/dl; a prandial insulin, preferably a short-acting analogue such as lispro or aspart, is used to control post-prandial glucose (PPG) excursions below 140 mg/dl. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract. 2005 Jun;68 Suppl1:S22-9. Use of Hypoglycaemic drugs in the therapy of T2DM Diet + Physical activity HbA 1 c>7% Insulin-sensitizing agent and/or insulin secretagogue HbA 1 c>7% Basal insulin (NPH/Glargine) FPG target: <100 mg/dl Prandial insulin (Lispro/Aspart) PPG target: <140 mg/dl
 below 100 mg/dl; a prandial insulin, preferably a short-acting analogue such as lispro or aspart, is used to control post-prandial glucose (PPG) excursions below 140 mg/dl. Pathophysiology of type 2 diabetes: Rationale for different oral antidiabetic treatment strategies - Diabetes Res Clin Pract Jun;68 Suppl1:S22-9. Use of Hypoglycaemic drugs in the therapy of T2DM Diet + Physical activity HbA 1 c>7% Insulin-sensitizing agent and/or insulin secretagogue HbA 1 c>7% Basal insulin (NPH/Glargine) FPG target: <100 mg/dl Prandial insulin (Lispro/Aspart) PPG target: <140 mg/dl.")
141
Change in weight (%) by category in patients with type 2 diabetes treated with rosiglitazone plus metformin (n ¼ 10,321). Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280

142
Mean change in weight in the United Kingdom Prospective Diabetes Study (overweight cohort). Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280

143
Effect of rosiglitazone 8 mg/day vs. placebo on intra-abdominal, subcutaneous and intrahepatic fat Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280

144
The time course of changes in serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) during treatment with rosiglitazone Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280
 and aspartate aminotransferase (AST) during treatment with rosiglitazone Thiazolidinediones, insulin resistance and obesity: finding a balance - Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, October 2006, 60, 10, 1272–1280")
145
The pathway of muscle glycogen synthesis. GLUT 4 glucose transporter 4; UDP uridine 5-diphosphate. Etiology of Insulin Resistance - The American Journal of Medicine (2006) Vol 119 (5A), 10S-16S
 Vol 119 (5A), 10S-16S.")
146
The mechanism of fatty acid-induced insulin resistance in muscle (A) and liver (B). GLUT 4 = glucose transporter 4; IRS = insulin-receptor substrate; PI 3-kinase = phosphatidylinositol 3-kinase; nPKC = novel protein kinase C. Etiology of Insulin Resistance - The American Journal of Medicine (2006) Vol 119 (5A), 10S-16S
 Vol 119 (5A), 10S-16S.")
147
Alternative causes of insulin resistance (IR) mediated via fat accumulation in skeletal muscle and liver. Etiology of Insulin Resistance - The American Journal of Medicine (2006) Vol 119 (5A), 10S-16S
 Vol 119 (5A), 10S-16S.")
148
Antidiabetogenic effects of GLP-1 GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081")
149
GLP-1 mimetics under development GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081")
150
Potency and selectivity of some DPP-IV inhibitors GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081")
151
Structures of DPP-IV inhibitors. GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081.")
152
DPP-IV inhibitors in various clinical phases GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081")
153
Physiological processes modulated by DPP-IV activity GLP-1 based therapy for type 2 diabetes - european journal of pharmaceutical sciences 2 8 ( 2 0 0 6 ) 96–1081
 96–1081")
154
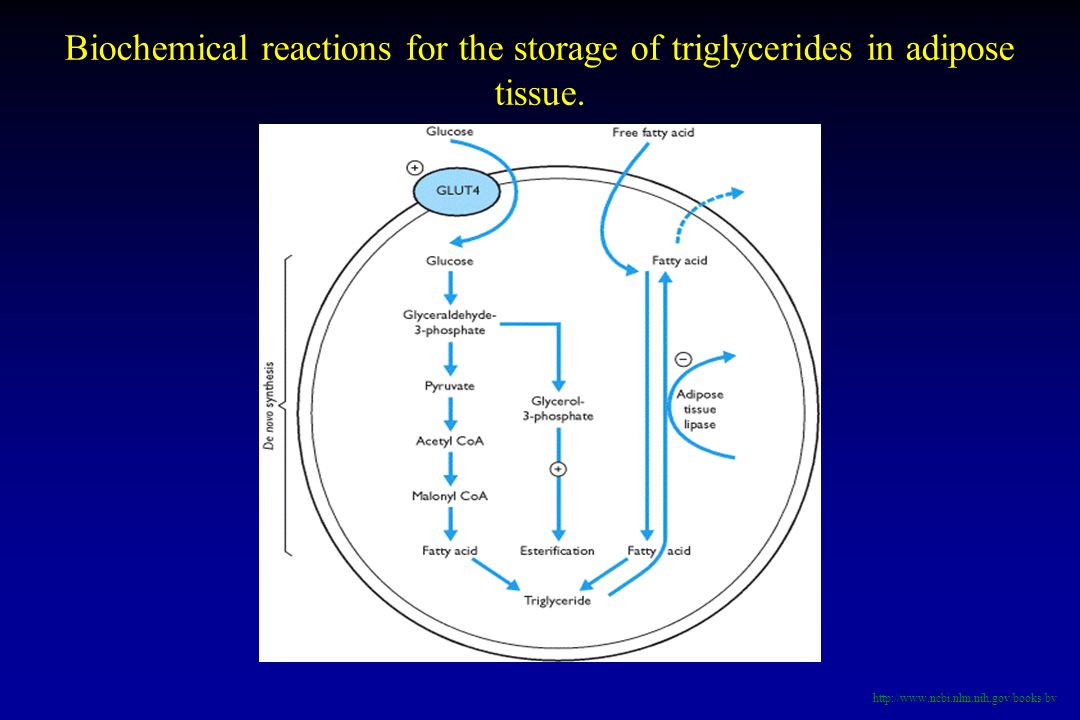
Biochemical reactions for the storage of triglycerides in adipose tissue. http://www.ncbi.nlm.nih.gov/books/bv
155
Major aspects of lipid turnover in man http://www.ncbi.nlm.nih.gov/books/bv

156
The formation of ketone bodies Acetyl CoA, formed from pyruvate and fatty oxidation hydrolysis enters the TCA cycle. In diabetes or fasting, oxaloacetate is consumed by the gluconeogenic pathway. There is reduced incorporation of acetyl CoA into citrate (x) and hence acetyl CoA is converted to form ketone bodies. http://www.ncbi.nlm.nih.gov/books/bv
 and hence acetyl CoA is converted to form ketone bodies.")
157
The family of glucose transporters (GLUTs 1–5) http://www.ncbi.nlm.nih.gov/books/bv
")
158
Therapies for DM - 1 Human insulin replacement http://www.ncbi.nlm.nih.gov/books/bv

159
Therapies for DM - 1 Human insulin replacement http://www.ncbi.nlm.nih.gov/books/bv

160
Increase in plasma insulin concentration after a sudden increase in blood glucose to two to three times the normal range Guyton & Hall. Textbook of Medical Physiology. Tenth Edition.

161
Approximate insulin secretion at different plasma glucose levels Guyton & Hall. Textbook of Medical Physiology. Tenth Edition.

162
Approximate plasma glucagon concentration at different blood glucose levels

163
Guyton & Hall. Textbook of Medical Physiology. Tenth Edition. Changes in blood constituents in diabetic coma, showing normal values (light bars) and diabetic coma values (dark bars)
 and diabetic coma values (dark bars).")
164
Action of insulin on the adipocyte The effects of insulin on adipose tissue. http://www.ncbi.nlm.nih.gov/books/bv
167
insulin signaling system in healthy normal glucose tolerant A) and T2DM B) subjects. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 01

168
The triumvirate: insulin resistance in liver and muscle with impaired insulin secretion represent the three core defects in T2DM. Reproduced with permission from DeFronzo RA. Lilly lecture. The triumvirate: Beta-cell, muscle, liver. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 02

169
Effect of thiazolidinedione (TZD) treatment on beta cell function. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 03

170
Pioglitazone positively affects the insulin signaling system resulting in improved glycemic control, generation of nitric oxide and decreased MAP kinase pathway activation. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 04

171
Effect of thiazolidinediones (TZDs) on body fat distribution. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 05

172
GLP-1 levels decline as glucose tolerance deteriorates A), whereas GiP levels are normal or elevated in patients with type 2 diabetes mellitus B). Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 06

173
Percentage (%) of subjects achieving select HbA targets with alogliptin in Phase 3 trials. Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 08

174
Necessity for hyperglycemic rescue* in Phase iii trials with alogliptin Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 09

175
The ominous octet: pathophysiologic abnormalities in type 2 diabetes mellitus Pioglitazone and alogliptin combination therapy in type 2 diabetes: a pathophysiologically sound Treatment - Vascular Health and Risk Management 2010:6 671–690 – Fig 10











 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")















 deste empréstimo é 4% a.m. Quanto vai ser pago no.>")


