Carregar apresentação
1
Avanços em Ventilação Mecânica
(Advances in mechanical ventilation). Martin J. Tobin N Engl J Med 2001;334: Apresentação: Danielli Feitosa Unidade de Neonatologia do HRAS/SES/DF
. Martin J. Tobin. N Engl J Med 2001;334: Apresentação: Danielli Feitosa. Unidade de Neonatologia do HRAS/SES/DF.")
2
Introdução Suporte ventilatório é uma das principais causas de internação em terapia intensiva Este artigo apresenta os princípios básicos de ventilação mecânica (VM) bem como as atualizações revista pelo autor
 bem como as atualizações revista pelo autor.")
3
Princípios básicos Indicações para VM (N=1638)
Insuficiência respiratória aguda: 66% Coma: 15% Exarcebação aguda da Doença pulmonar obstrutiva crônica (DPOC): 13% Distúrbios neuromusculares 5%
: 13% Distúrbios neuromusculares 5%")
4
Insuficiência Respiratória Aguda
Síndrome do desconforto respiratório agudo (SDRA) Insuficiência cardíaca congestiva Pneumonia Sepses Complicações de Pós-operatória Trauma
 Insuficiência cardíaca congestiva. Pneumonia. Sepses. Complicações de Pós-operatória. Trauma.")
5
Objetivos da VM Diminuir o trabalho respiratório
Reverter a hipoxemia e corrigir a acidose respiratória progressiva

6
Modalidades Assisto-controlada Mandatório intermitente
Pressão de suporte

7
Assisto controlado Modalidade mais usada
Permite a ventilação espontânea do paciente. quando o mesmo tem a capacidade de ativar o respirador Quando o paciente não possui “drive” respiratório , o ventilador é ativado em um tempo selecionado

8
Ventilação mandatória intermitente
Foi introduzida para prover níveis graduais de assistência O médico ajusta o número de ventilações mandatórias de volume fixo e entre essas respirações o pct pode respirar espontaneamente Dificuldade de adaptação suporte menor do que o necessário

9
Pressão de suporte Escolha do nível de pressão mais do que o de volume
Os níveis de pressão escolhidos são ajustados de acordo com a freqüência respiratória (16 a 30)
")
10
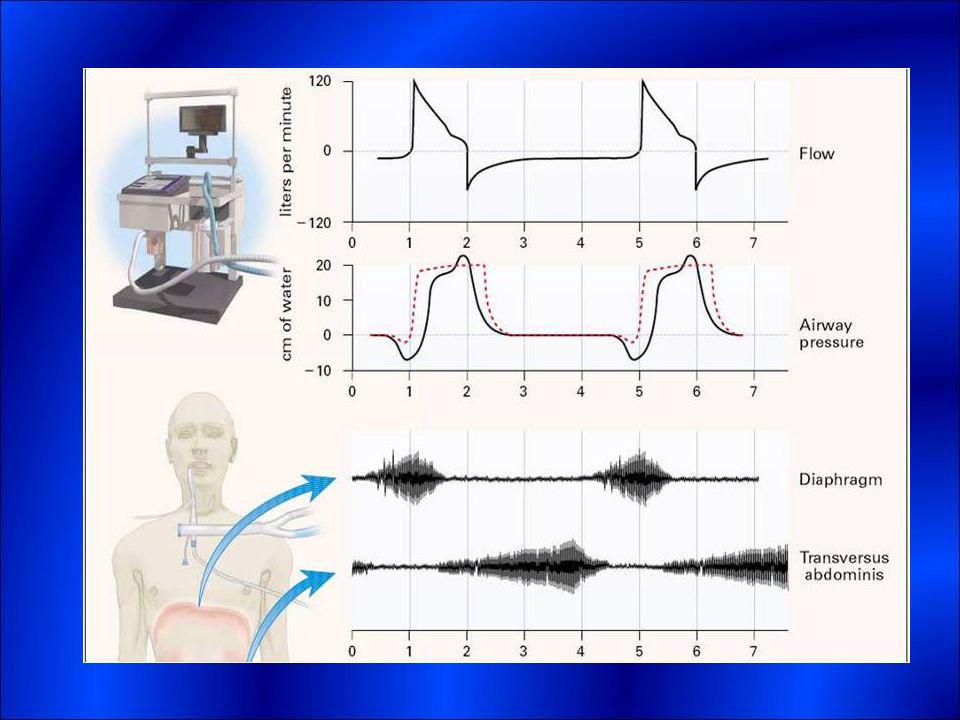
Coordenação do esforço respiratório e ventilação mecânica
Pacientes críticos em que o esforço respiratório se mantém sustentado leva a uma fadiga da musculatura lesão estrutural nos músculos fatigados Não basta conectar ao ventilador É necessário ajuste dos parâmetros de modo a fornecer uma ventilação adequada e eficiente

11
Coordenação do esforço respiratório e ventilação mecânica
Fornecer suporte ventilatório mas tentando manter um drive do próprio paciente evitando a atrofia muscular que levaria a dificuldade do desmame O período de inspiração mecânica deve coincidir com o tempo inspiratório neural A inatividade mecânica momento de expiração do paciente

12
Coordenação do esforço respiratório e ventilação mecânica
A dificuldade na sincronização acontece quando o esforço inspiratório do paciente não coincide com fluxo dado pelo ventilador O esforço inspiratório do paciente permite ativar o ventilador O ajuste é feito para iniciar a ventilação mecânica quando o sistema é submetido a uma pressão de -1 a -2cmH2O sensibilidade

14
Melhorando a oxigenação e prevenindo o dano pulmonar
O objetivo inicial da ventilação mecânica é melhorar a oxigenação Lesões alveolares SDRA representa um desafio SDRA é uma forma de edema pulmonar não cardiogênico resultado de um dano alveolar agudo severo

15
Pseudocistos à esquerda Pneumatocele à direita
Secção de pulmão salientando pseudocisto Pneumatocele paramediastinal

16
Melhorando a oxigenação e prevenindo o dano pulmonar
Aumento na concentração de oxigênio e da pressão nas vias aéreas promove m uma melhor oxigenação arterial potencial tóxico Estudos anteriores mostram que a VM pode causar ruptura alveolar e escape de ar Webb e Tierney lesão estrutural independente do escape de ar

17
Melhorando a oxigenação e prevenindo o dano pulmonar
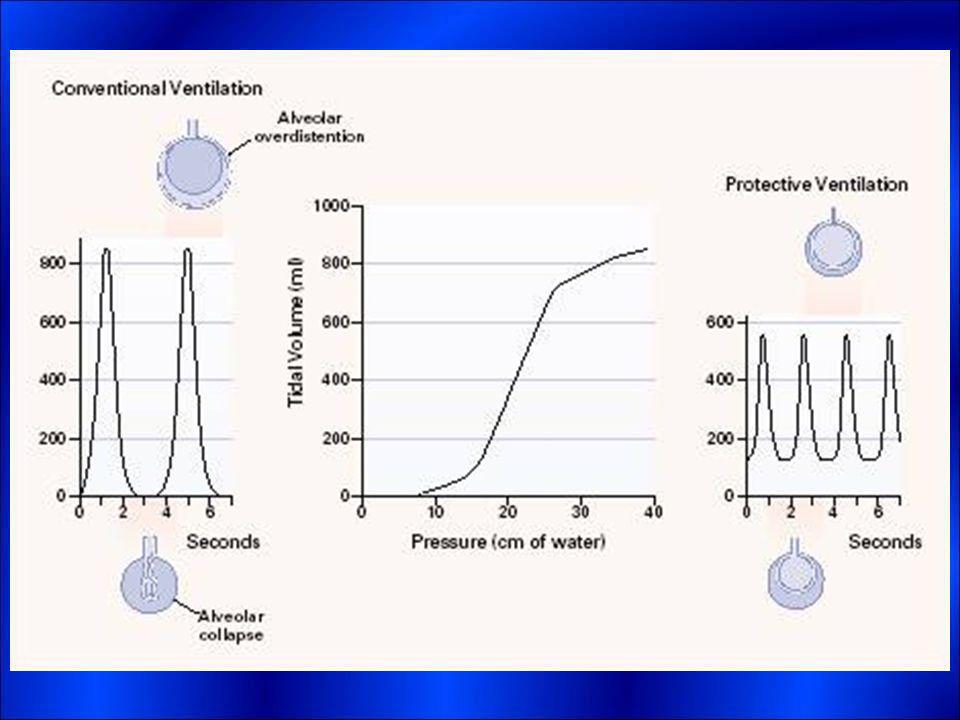
A superdistensão alveolar causa mudanças na permeabilidade do endotélio e epitélio, hemorragia alveolar e membrana hialina em estudos experimentais

18
Melhorando a oxigenação e prevenindo o dano pulmonar
Uma nova era do manejo respiratório começou em 1990 Hickling et al relataram que um baixo volume corrente permitiu uma diminuição na taxa de mortalidade na ordem de 60% de pacientes com SDRA Observou-se que os melhores resultados na ventilação de pacientes com SDRA, foram submetidos além de um baixo volume corrente, a uma pressão de platô

19
Melhorando a oxigenação e prevenindo o dano pulmonar
O grande problema em relação a variação pressórica diz respeito a pressão transpulmonar e não a pressão nas vias aéreas

20
Melhorando a oxigenação e prevenindo o dano pulmonar
A maneira mais usual de melhorar a oxigenação é com o uso da PEEP, com a intenção de recrutar o tecido de pulmão previamente não funcionante Selecionar o correto nível da PEEP para um paciente com SDRA é difícil porque a severidade do dano pode variar em cada pulmão

21
Melhorando a oxigenação e prevenindo o dano pulmonar
A PEEP pode recrutar áreas atelectásicas e também áreas normalmente ventiladas sobredistenção 30% pacientes com dano pulmonar não se beneficiam com a PEEP A postura supina recruta geralmente as regiões do pulmão mais próximas do ápice

22
Melhorando a oxigenação e prevenindo o dano pulmonar
Danos pulmonares como a pneumonia são menos beneficiados da PEEP do que aqueles com causas não pulmonares (sepse, traumas) Distinção relacionada pela morfologia Causas pulmonaresdistensão alveolar Causas não pulmonaresedema intersticial e colapso alveolar
 Distinção relacionada pela morfologia. Causas pulmonaresdistensão alveolar. Causas não pulmonaresedema intersticial e colapso alveolar.")
24
Interromper a ventilação mecânica
O processo de interromper a VM deve ser realizado o mais rápido possível, e esse desmame toma grande parte da equipe em cuidados intensivos Cerca 25% terão complicações podendo ser necessária uma ventilação de suporte

25
Após a desconexão do VM aumento da frequência respiratória, queda do volume corrente, respirações superficiais, esforço respiratório aumentando 4 vezes o normal, uso da musculatura acessória, estress e cardiovascular

26
O nível de oxigênio deve ser satisfatório antes de tentar interromper a VM
Um dado de confiança é a relação da frequência respiratória e do volume corrente (uma taxa de 100 é o melhor discriminante entre os pacientes que serão extubados com sucesso ou não)
")
27
Desmame 4 métodos de desmame
Respiração espontânea diversas vezes ao dia com tube-T Ventilações mandatórias intermitentes e de pressão, com diminuição gradual reduzindo também o número de freqüências mandatórias, até um nível mínimo suportável Experimentação diária com tube-T

28
Extubação Manter a ventilação espontânea sem desconforto

29
Conclusão Desde a última revisão do autor, houve ganho na compreensão da fisiopatologia ventila tória associada a um sucesso ruim no desmame, e ações mais eficazes no sucesso deste Maiores conhecimentos em relação aos ajustes do ventilador e como estes influenciam na sobrevivência dos pacientes com SDRA

30
Conclusão Pouco progresso em determinar o melhor ventilador a ser usado para diminuir a fatiga muscular. Desafio para novas pesquisas identificar elementos do nosso conhecimento atual que possam ser incorporados no manejo dos pacientes para obtenção de melhores resultados

31
Referências do artigo:
Tobin MJ. Mechanical ventilation. N Engl J Med 1994;330: [Free Full Text] Esteban A, Anzueto A, Alia I, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med 2000;161: [Free Full Text] Sassoon CSH. Intermittent mandatory ventilation. In: Tobin JM, ed. Principles and practice of mechanical ventilation. New York: McGraw-Hill, 1994: Marini JJ, Smith TC, Lamb VJ. External work output and force generation during synchronized intermittent mechanical ventilation: effect of machine assistance on breathing effort. Am Rev Respir Dis 1988;138: [ISI][Medline] Brochard L. Pressure support ventilation. In: Tobin MJ, ed. Principles and practice of mechanical ventilation. New York: McGraw-Hill, 1994: Jubran A, Van de Graaff WB, Tobin MJ. Variability of patient-ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995;152: [Abstract] Jubran A, Tobin JM. Pathophysiologic basis of acute respiratory distress in patients who fail a trial of weaning from mechanical ventilation. Am J Respir Crit Care Med 1997;155: [Abstract] Reid WD, Huang J, Bryson S, Walker DC, Belcastro AN. Diaphragm injury and myofibrillar structure induced by resistive loading. J Appl Physiol 1994;76: [Free Full Text] Leung P, Jubran A, Tobin MJ. Comparison of assisted ventilator modes on triggering, patient effort, and dyspnea. Am J Respir Crit Care Med 1997;155: [Abstract] Anzueto A, Peters JI, Tobin JM, et al. Effects of prolonged controlled mechanical ventilation on diaphragmatic function in healthy adult baboons. Crit Care Med 1997;25: [CrossRef][ISI][Medline] Parthasarathy S, Jubran A, Tobin MJ. Cycling of inspiratory and expiratory muscle groups with the ventilator in airflow limitation. Am J Respir Crit Care Med 1998;158: [Erratum, Am J Respir Crit Care Med 1999;159:1023.] [Free Full Text] Simon PM, Zurob AS, Wies WM, Leiter JC, Hubmayr RD. Entrainment of respiration in humans by periodic lung inflations: effect of state and CO2. Am J Respir Crit Care Med 1999;160: [Free Full Text] Parthasarathy S, Jubran A, Tobin MJ. Assessment of neural inspiratory time in ventilator-supported patients. Am J Respir Crit Care Med 2000;162: [Free Full Text] Sassoon CSH, Gruer SE. Characteristics of the ventilator pressure- and flow-trigger variables. Intensive Care Med 1995;21: [CrossRef][ISI][Medline] Marini JJ, Capps JS, Culver BH. The inspiratory work of breathing during assisted mechanical ventilation. Chest 1985;87: [Free Full Text]

32
Giannouli E, Webster K, Roberts D, Younes M
Giannouli E, Webster K, Roberts D, Younes M. Response of ventilator-dependent patients to different levels of pressure support and proportional assist. Am J Respir Crit Care Med 1999;159: [Free Full Text] Sinderby C, Navalesi P, Beck J, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med 1999;5: [CrossRef][ISI][Medline] Puddy A, Younes M. Effect of inspiratory flow rate on respiratory output in normal subjects. Am Rev Respir Dis 1992;146: [ISI][Medline] Laghi F, Karamchandani K, Tobin MJ. Influence of ventilator settings in determining respiratory frequency during mechanical ventilation. Am J Respir Crit Care Med 1999;160: [Free Full Text] Pierson DJ. Barotrauma and bronchopleural fistula. In: Tobin MJ, ed. Principles and practice of mechanical ventilation. New York: McGraw-Hill, 1994: Webb HH, Tierney DF. Experimental pulmonary edema due to intermittent positive pressure ventilation with high inflation pressures: protection by positive end-expiratory pressure. Am Rev Respir Dis 1974;110: [ISI][Medline] Dreyfuss D, Saumon G. Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med 1998;157: [Free Full Text] Puybasset L, Cluzel P, Chao N, Slutsky AS, Coriat P, Rouby JJ. A computed tomography scan assessment of regional lung volume in acute lung injury. Am J Respir Crit Care Med 1998;158: [Free Full Text] Gattinoni L, Pesenti A, Bombino M, et al. Relationships between lung computed tomographic density, gas exchange, and PEEP in acute respiratory failure. Anesthesiology 1988;69: [ISI][Medline] Rouby JJ, Lherm T, Martin de Lassale E, et al. Histologic aspects of pulmonary barotrauma in critically ill patients with acute respiratory failure. Intensive Care Med 1993;19: [CrossRef][ISI][Medline] Hickling KG, Henderson SJ, Jackson R. Low mortality associated with low volume pressure limited ventilation with permissive hypercapnia in severe adult respiratory distress syndrome. Intensive Care Med 1990;16: [CrossRef][ISI][Medline] Amato MB, Barbas CS, Medeiros DM, et al. Beneficial effects of the "open lung approach" with low distending pressures in acute respiratory distress syndrome: a prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med 1995;152: [Abstract] Amato MBP, Barbas CSV, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 1998;338: [Free Full Text] The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342: [Free Full Text] Stewart TE, Meade MO, Cook DJ, et al. Evaluation of a ventilation strategy to prevent barotrauma in patients at high risk for acute respiratory distress syndrome. N Engl J Med 1998;338: [Free Full Text]

33
Brochard L, Roudot-Thoraval F, Roupie E, et al
Brochard L, Roudot-Thoraval F, Roupie E, et al. Tidal volume reduction for prevention of ventilator-induced lung injury in acute respiratory distress syndrome. Am J Respir Crit Care Med 1998;158: [Free Full Text] Brower RG, Shanholtz CB, Fessler HE, et al. Prospective, randomized, controlled clinical trial comparing traditional versus reduced tidal volume ventilation in acute respiratory distress syndrome patients. Crit Care Med 1999;27: [CrossRef][ISI][Medline] Tobin MJ. Culmination of an era in research on the acute respiratory distress syndrome. N Engl J Med 2000;342: [Free Full Text] Brochard L. Respiratory pressure-volume curves. In: Tobin MJ, ed. Principles and practice of intensive care monitoring. New York: McGraw-Hill, 1998: Roupie E, Dambrosio M, Servillo G, et al. Titration of tidal volume and induced hypercapnia in acute respiratory distress syndrome. Am J Respir Crit Care Med 1995;152: [Abstract] Richecoeur J, Lu Q, Vieira SR, et al. Expiratory washout versus optimization of mechanical ventilation during permissive hypercapnia in patients with severe acute respiratory distress syndrome. Am J Respir Crit Care Med 1999;160:77-85. [Free Full Text] Feihl F, Perret C. Permissive hypercapnia: how permissive should we be? Am J Respir Crit Care Med 1994;150: [ISI][Medline] Feihl F, Eckert P, Brimioulle S, et al. Permissive hypercapnia impairs pulmonary gas exchange in the acute respiratory distress syndrome. Am J Respir Crit Care Med 2000;162: [Free Full Text] Mead J, Collier C. Relation of volume history of lungs to respiratory mechanics in anesthetized dogs. J Appl Physiol 1959;14: [Free Full Text] Pelosi P, Cadringher P, Bottino N, et al. Sigh in acute respiratory distress syndrome. Am J Respir Crit Care Med 1999;159: [Free Full Text] Dambrosio M, Roupie E, Mollett JJ, et al. Effects of positive end-expiratory pressure and different tidal volumes on alveolar recruitment and hyperinflation. Anesthesiology 1997;87: [ISI][Medline] Vieira SR, Puybasset L, Lu Q, et al. A scanographic assessment of pulmonary morphology in acute lung injury: significance of the lower inflection point detected on the lung pressure-volume curve. Am J Respir Crit Care Med 1999;159: [Free Full Text] Vieira SR, Puybasset L, Richecoeur J, et al. A lung computed tomographic assessment of positive end-expiratory pressure-induced lung overdistension. Am J Respir Crit Care Med 1998;158: [Free Full Text] Horton WG, Cheney FW. Variability of effect of positive end expiratory pressure. Arch Surg 1975;110: [Abstract] Kanarek DJ, Shannon DC. Adverse effect of positive end-expiratory pressure on pulmonary perfusion and arterial oxygenation. Am Rev Respir Dis 1975;112: [ISI][Medline]

34
Gattinoni L, Pelosi P, Suter PM, Pedoto A, Vercesi P, Lissoni A
Gattinoni L, Pelosi P, Suter PM, Pedoto A, Vercesi P, Lissoni A. Acute respiratory distress syndrome caused by pulmonary and extrapulmonary disease: different syndromes? Am J Respir Crit Care Med 1998;158:3-11. [Free Full Text] Lu Q, Vieira SR, Richecoeur J, et al. A simple automated method for measuring pressure-volume curves during mechanical ventilation. Am J Respir Crit Care Med 1999;159: [Free Full Text] Argiras EP, Blakeley CR, Dunnill MS, Otremski S, Sykes MK. High PEEP decreases hyaline membrane formation in surfactant deficient lungs. Br J Anaesth 1987;59: [Free Full Text] Tremblay L, Valenza F, Ribeiro SP, Li J, Slutsky AS. Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J Clin Invest 1997;99: [Free Full Text] Mead J, Takishima T, Leith D. Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol 1970;28: [Free Full Text] Hickling KG. The pressure-volume curve is greatly modified by recruitment: a mathematical model of ARDS lungs. Am J Respir Crit Care Med 1998;158: [Free Full Text] Martynowicz MA, Minor TA, Walters BJ, Hubmayr RD. Regional expansion of oleic acid-injured lungs. Am J Respir Crit Care Med 1999;160: [Free Full Text] Lichtwarck-Aschoff M, Mols G, Hedlund AJ, et al. Compliance is nonlinear over tidal volume irrespective of positive end-expiratory pressure level in surfactant-depleted piglets. Am J Respir Crit Care Med 2000;162: [Free Full Text] Carney DE, Bredenberg CE, Schiller HJ, et al. The mechanism of lung volume change during mechanical ventilation. Am J Respir Crit Care Med 1999;160: [Free Full Text] Harris RS, Hess DR, Venegas JG. An objective analysis of the pressure-volume curve in the acute respiratory distress syndrome. Am J Respir Crit Care Med 2000;161: [Free Full Text] Pelosi P, Tubiolo D, Mascheroni D, et al. Effects of the prone position on respiratory mechanics and gas exchange during acute lung injury. Am J Respir Crit Care Med 1998;157: [Free Full Text] Gattinoni L, Pelosi P, Vitale G, Pesenti A, D'Andrea L, Mascheroni D. Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure. Anesthesiology 1991;74:15-23. [ISI][Medline] Mutoh T, Guest RJ, Lamm WJ, Albert RK. Prone position alters the effect of volume overload on regional pleural pressures and improves hypoxemia in pigs in vivo. Am Rev Respir Dis 1992;146: [ISI][Medline] Mure M, Domino KB, Lindahl SG, Hlastala MP, Altemeier WA, Glenny RW. Regional ventilation-perfusion distribution is more uniform in the prone position. J Appl Physiol 2000;88: [Free Full Text] Albert RK, Hubmayr RD. The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med 2000;161: [Free Full Text]

35
Brochard L, Rauss A, Benito S, et al
Brochard L, Rauss A, Benito S, et al. Comparison of three methods of gradual withdrawing from ventilatory support during weaning from mechanical ventilation. Am J Respir Crit Care Med 1994;150: [Abstract] Esteban A, Frutos F, Tobin MJ, et al. A comparison of four methods of weaning patients from mechanical ventilation. N Engl J Med 1995;332: [Free Full Text] Tobin MJ, Perez W, Guenther SM, et al. The pattern of breathing during successful and unsuccessful trials of weaning from mechanical ventilation. Am Rev Respir Dis 1986;134: [ISI][Medline] Tobin MJ, Chadha TS, Jenouri G, Birch SJ, Gazeroglu HB, Sackner MA. Breaking patterns. 1. Normal subjects. Chest 1983;84: [Free Full Text] Jubran A, Mathru M, Dries D, Tobin MJ. Continuous recordings of mixed venous oxygen saturation during weaning from mechanical ventilation and the ramifications thereof. Am J Respir Crit Care Med 1998;158: [Free Full Text] Jubran A, Tobin MJ. Passive mechanics of lung and chest wall in patients who failed or succeeded in trials of weaning. Am J Respir Crit Care Med 1997;155: [Abstract] Lemaire F, Teboul JL, Cinotti L, et al. Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology 1988;69: [ISI][Medline] Stroetz RW, Hubmayr RD. Tidal volume maintenance during weaning with pressure support. Am J Respir Crit Care Med 1995;152: [Abstract] Ely EW, Baker AM, Dunagan DP, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 1996;335: [Free Full Text] Coplin WM, Pierson DJ, Cooley KD, Newell DW, Rubenfeld GD. Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J Respir Crit Care Med 2000;161: [Free Full Text] Tobin MJ, Alex CG. Discontinuation of mechanical ventilation. In: Tobin MJ, ed. Principles and practice of mechanical ventilation. New York: McGraw-Hill, 1994: Yang KL, Tobin MJ. A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med 1991;324: [Abstract] Jaeschke RZ, Meade MO, Guyatt GH, Keenan SP, Cook DJ. How to use diagnostic test articles in the intensive care unit: diagnosing weanability using f/Vt. Crit Care Med 1997;25: [CrossRef][ISI][Medline] Sassoon CSH, Mahutte CK. Airway occlusion pressure and breathing pattern as predictors of weaning outcome. Am Rev Respir Dis 1993;148: [ISI][Medline] Epstein SK. Etiology of extubation failure and the predictive value of the rapid shallow breathing index. Am J Respir Crit Care Med 1995;152: [Abstract]

36
Jacob B, Chatila W, Manthous CA
Jacob B, Chatila W, Manthous CA. The unassisted respiratory rate/tidal volume ratio accurately predicts weaning outcome in postoperative patients. Crit Care Med 1997;25: [CrossRef][ISI][Medline] Vallverdu I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med 1998;158: [Free Full Text] Maldonado A, Bauer TT, Ferrer M, et al. Capnometric recirculation gas tonometry and weaning from mechanical ventilation. Am J Respir Crit Care Med 2000;161: [Free Full Text] Tobin MJ Donald F Egan Scientific Lecture: weaning from mechanical ventilation: what have we learned? Respir Care 2000;45: [Medline] Brochard L, Rua F, Lorino H, Lemaire F, Harf A. Inspiratory pressure support compensates for the additional work of breathing caused by the endotracheal tube. Anesthesiology 1991;75: [ISI][Medline] Straus C, Louis B, Isabey D, Lemaire F, Harf A, Brochard L. Contribution of the endotracheal tube and the upper airway to breathing workload. Am J Respir Crit Care Med 1998;157:23-30. [Free Full Text] Laghi F, D'Alfonso N, Tobin MJ. Pattern of recovery from diaphragmatic fatigue over 24 hours. J Appl Physiol 1995;79: [Free Full Text] Esteban A, Alia I, Tobin MJ, et al. Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Am J Respir Crit Care Med 1999;159: [Free Full Text] Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997;112: [Free Full Text] Nava S, Ambrosino N, Clini E, et al. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease: a randomized, controlled trial. Ann Intern Med 1998;128: [Free Full Text] Hillberg RE, Johnson DC. Noninvasive ventilation. N Engl J Med 1997;337: [Free Full Text] Leach CL, Greenspan JS, Rubenstein SD, et al. Partial liquid ventilation with perflubron in premature infants with severe respiratory distress syndrome. N Engl J Med 1996;335: [Free Full Text]

37
This article has been cited by other articles:
Hughes-Davies, T., Arah, O. A., Kahn, J. M., Rubenfeld, G. D. (2006). Hospital volume and outcomes of mechanical ventilation.. NEJM 355: [Full Text] Crimi, E., Zhang, H., Han, R. N. N., Sorbo, L. D., Ranieri, V.M., Slutsky, A. S. (2006). Ischemia and Reperfusion Increases Susceptibility to Ventilator-induced Lung Injury in Rats. Am. J. Respir. Crit. Care Med. 174: [Abstract] [Full Text] Moerer, O., Fischer, S., Hartelt, M., Kuvaki, B., Quintel, M., Neumann, P. (2006). Influence of Two Different Interfaces for Noninvasive Ventilation Compared to Invasive Ventilation on the Mechanical Properties and Performance of a Respiratory System: A Lung Model Study. Chest 129: [Abstract] [Full Text] L'Her, E., Deye, N., Lellouche, F., Taille, S., Demoule, A., Fraticelli, A., Mancebo, J., Brochard, L. (2005). Physiologic Effects of Noninvasive Ventilation during Acute Lung Injury. Am. J. Respir. Crit. Care Med. 172: [Abstract] [Full Text] Doerr, C. H., Gajic, O., Berrios, J. C., Caples, S., Abdel, M., Lymp, J. F., Hubmayr, R. D. (2005). Hypercapnic Acidosis Impairs Plasma Membrane Wound Resealing in Ventilator-injured Lungs. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Jubran, A., Grant, B. J. B., Laghi, F., Parthasarathy, S., Tobin, M. J. (2005). Weaning Prediction: Esophageal Pressure Monitoring Complements Readiness Testing. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Eutamene, H., Theodorou, V., Schmidlin, F., Tondereau, V., Garcia-Villar, R., Salvador-Cartier, C., Chovet, M., Bertrand, C., Bueno, L. (2005). LPS-induced lung inflammation is linked to increased epithelial permeability: role of MLCK. Eur Respir J 25: [Abstract] [Full Text] Burleson, B. S., Maki, E. D. (2005). Acute Respiratory Distress Syndrome. Journal of Pharmacy Practice 18: [Abstract] Kornecki, A., Tsuchida, S., Ondiveeran, H. K., Engelberts, D., Frndova, H., Tanswell, A. K., Post, M., McKerlie, C., Belik, J., Fox-Robichaud, A., Kavanagh, B. P. (2005). Lung Development and Susceptibility to Ventilator-induced Lung Injury. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Jackson, W L Jr, Gallagher, C, Myhand, R C, Waselenko, J K (2005). Medical management of patients with multiple organ dysfunction arising from acute radiation syndrome. Br. J. Radiol. Supplement_27: [Abstract] [Full Text] Tobin, M. J. (2004). Of Principles and Protocols and Weaning. Am. J. Respir. Crit. Care Med. 169: [Full Text] Prinianakis, G., Delmastro, M., Carlucci, A., Ceriana, P., Nava, S. (2004). Effect of varying the pressurisation rate during noninvasive pressure support ventilation. Eur Respir J 23: [Abstract] [Full Text] Magder, S. (2004). Clinical Usefulness of Respiratory Variations in Arterial Pressure. Am. J. Respir. Crit. Care Med. 169: [Full Text] Allen, G., Bates, J. H. T. (2004). Dynamic mechanical consequences of deep inflation in mice depend on type and degree of lung injury. J. Appl. Physiol. 96: [Abstract] [Full Text] Sinderby, C. (2003). Ventilatory Assist Driven by Patient Demand. Am. J. Respir. Crit. Care Med. 168: [Full Text]
. Hospital volume and outcomes of mechanical ventilation.. NEJM 355: [Full Text] Crimi, E., Zhang, H., Han, R. N. N., Sorbo, L. D., Ranieri, V.M., Slutsky, A. S. (2006). Ischemia and Reperfusion Increases Susceptibility to Ventilator-induced Lung Injury in Rats. Am. J. Respir. Crit. Care Med. 174: [Abstract] [Full Text] Moerer, O., Fischer, S., Hartelt, M., Kuvaki, B., Quintel, M., Neumann, P. (2006). Influence of Two Different Interfaces for Noninvasive Ventilation Compared to Invasive Ventilation on the Mechanical Properties and Performance of a Respiratory System: A Lung Model Study. Chest 129: [Abstract] [Full Text] L Her, E., Deye, N., Lellouche, F., Taille, S., Demoule, A., Fraticelli, A., Mancebo, J., Brochard, L. (2005). Physiologic Effects of Noninvasive Ventilation during Acute Lung Injury. Am. J. Respir. Crit. Care Med. 172: [Abstract] [Full Text] Doerr, C. H., Gajic, O., Berrios, J. C., Caples, S., Abdel, M., Lymp, J. F., Hubmayr, R. D. (2005). Hypercapnic Acidosis Impairs Plasma Membrane Wound Resealing in Ventilator-injured Lungs. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Jubran, A., Grant, B. J. B., Laghi, F., Parthasarathy, S., Tobin, M. J. (2005). Weaning Prediction: Esophageal Pressure Monitoring Complements Readiness Testing. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Eutamene, H., Theodorou, V., Schmidlin, F., Tondereau, V., Garcia-Villar, R., Salvador-Cartier, C., Chovet, M., Bertrand, C., Bueno, L. (2005). LPS-induced lung inflammation is linked to increased epithelial permeability: role of MLCK. Eur Respir J 25: [Abstract] [Full Text] Burleson, B. S., Maki, E. D. (2005). Acute Respiratory Distress Syndrome. Journal of Pharmacy Practice 18: [Abstract] Kornecki, A., Tsuchida, S., Ondiveeran, H. K., Engelberts, D., Frndova, H., Tanswell, A. K., Post, M., McKerlie, C., Belik, J., Fox-Robichaud, A., Kavanagh, B. P. (2005). Lung Development and Susceptibility to Ventilator-induced Lung Injury. Am. J. Respir. Crit. Care Med. 171: [Abstract] [Full Text] Jackson, W L Jr, Gallagher, C, Myhand, R C, Waselenko, J K (2005). Medical management of patients with multiple organ dysfunction arising from acute radiation syndrome. Br. J. Radiol. Supplement_27: [Abstract] [Full Text] Tobin, M. J. (2004). Of Principles and Protocols and Weaning. Am. J. Respir. Crit. Care Med. 169: [Full Text] Prinianakis, G., Delmastro, M., Carlucci, A., Ceriana, P., Nava, S. (2004). Effect of varying the pressurisation rate during noninvasive pressure support ventilation. Eur Respir J 23: [Abstract] [Full Text] Magder, S. (2004). Clinical Usefulness of Respiratory Variations in Arterial Pressure. Am. J. Respir. Crit. Care Med. 169: [Full Text] Allen, G., Bates, J. H. T. (2004). Dynamic mechanical consequences of deep inflation in mice depend on type and degree of lung injury. J. Appl. Physiol. 96: [Abstract] [Full Text] Sinderby, C. (2003). Ventilatory Assist Driven by Patient Demand. Am. J. Respir. Crit. Care Med. 168: [Full Text]")
38
Terragni, P.P., Rosboch, G.L., Lisi, A., Viale, A.G., Ranieri, V.M. (2003). How respiratory system mechanics may help in minimising ventilator-induced lung injury in ARDS patients. Eur Respir J 22: 15S-21s [Abstract] [Full Text] de Chazal, I., Hubmayr, R. D. (2003). Novel aspects of pulmonary mechanics in intensive care. Br J Anaesth 91: [Full Text] Wainwright, M. S., Rossi, J., Schavocky, J., Crawford, S., Steinhorn, D., Velentza, A. V., Zasadzki, M., Shirinsky, V., Jia, Y., Haiech, J., Van Eldik, L. J., Watterson, D. M. (2003). Protein kinase involved in lung injury susceptibility: Evidence from enzyme isoform genetic knockout and in vivo inhibitor treatment. Proc. Natl. Acad. Sci. USA 100: [Abstract] [Full Text] Vitacca, M., Barbano, L., D'Anna, S., Porta, R., Bianchi, L., Ambrosino, N. (2002). Comparison of Five Bilevel Pressure Ventilators in Patients With Chronic Ventilatory Failure: A Physiologic Study. Chest 122: [Abstract] [Full Text] Parthasarathy, S., Tobin, M. J. (2002). Effect of Ventilator Mode on Sleep Quality in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 166: [Abstract] [Full Text] Derdak, S., Mehta, S., Stewart, T. E., Smith, T., Rogers, M., Buchman, T. G., Carlin, B., Lowson, S., Granton, J., the Multicenter Oscillatory Ventilation, (2002). High-Frequency Oscillatory Ventilation for Acute Respiratory Distress Syndrome in Adults: A Randomized, Controlled Trial. Am. J. Respir. Crit. Care Med. 166: [Abstract] [Full Text] Tung, A., Morgan, S. E. (2002). Modeling the Effect of Progressive Endotracheal Tube Occlusion on Tidal Volume in Pressure-Control Mode. Anesth. Analg. 95: [Abstract] [Full Text] Hubmayr, R. D. (2002). Perspective on Lung Injury and Recruitment: A Skeptical Look at the Opening and Collapse Story. Am. J. Respir. Crit. Care Med. 165: [Full Text] Ambrosino, N, Rossi, A (2002). Proportional assist ventilation (PAV): a significant advance or a futile struggle between logic and practice?. Thorax 57: [Abstract] [Full Text] Martinon-Torres, F., Rodriguez-Nunez, A., Martinon-Sanchez, J. M., Tobin, M. J. (2001). Advances in Mechanical Ventilation. NEJM 345: [Full Text]
![Terragni, P.P., Rosboch, G.L., Lisi, A., Viale, A.G., Ranieri, V.M. (2003). How respiratory system mechanics may help in minimising ventilator-induced lung injury in ARDS patients. Eur Respir J 22: 15S-21s [Abstract] [Full Text]](http://slideplayer.com.br/slide/63819/1/images/38/Terragni%2C+P.P.%2C+Rosboch%2C+G.L.%2C+Lisi%2C+A.%2C+Viale%2C+A.G.%2C+Ranieri%2C+V.M.+%282003%29.+How+respiratory+system+mechanics+may+help+in+minimising+ventilator-induced+lung+injury+in+ARDS+patients.+Eur+Respir+J+22%3A+15S-21s+%5BAbstract%5D+%5BFull+Text%5D.jpg "de Chazal, I., Hubmayr, R. D. (2003). Novel aspects of pulmonary mechanics in intensive care. Br J Anaesth 91: [Full Text] Wainwright, M. S., Rossi, J., Schavocky, J., Crawford, S., Steinhorn, D., Velentza, A. V., Zasadzki, M., Shirinsky, V., Jia, Y., Haiech, J., Van Eldik, L. J., Watterson, D. M. (2003). Protein kinase involved in lung injury susceptibility: Evidence from enzyme isoform genetic knockout and in vivo inhibitor treatment. Proc. Natl. Acad. Sci. USA 100: [Abstract] [Full Text] Vitacca, M., Barbano, L., D Anna, S., Porta, R., Bianchi, L., Ambrosino, N. (2002). Comparison of Five Bilevel Pressure Ventilators in Patients With Chronic Ventilatory Failure: A Physiologic Study. Chest 122: [Abstract] [Full Text] Parthasarathy, S., Tobin, M. J. (2002). Effect of Ventilator Mode on Sleep Quality in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 166: [Abstract] [Full Text] Derdak, S., Mehta, S., Stewart, T. E., Smith, T., Rogers, M., Buchman, T. G., Carlin, B., Lowson, S., Granton, J., the Multicenter Oscillatory Ventilation, (2002). High-Frequency Oscillatory Ventilation for Acute Respiratory Distress Syndrome in Adults: A Randomized, Controlled Trial. Am. J. Respir. Crit. Care Med. 166: [Abstract] [Full Text] Tung, A., Morgan, S. E. (2002). Modeling the Effect of Progressive Endotracheal Tube Occlusion on Tidal Volume in Pressure-Control Mode. Anesth. Analg. 95: [Abstract] [Full Text] Hubmayr, R. D. (2002). Perspective on Lung Injury and Recruitment: A Skeptical Look at the Opening and Collapse Story. Am. J. Respir. Crit. Care Med. 165: [Full Text] Ambrosino, N, Rossi, A (2002). Proportional assist ventilation (PAV): a significant advance or a futile struggle between logic and practice . Thorax 57: [Abstract] [Full Text] Martinon-Torres, F., Rodriguez-Nunez, A., Martinon-Sanchez, J. M., Tobin, M. J. (2001). Advances in Mechanical Ventilation. NEJM 345: [Full Text]")
39
Obrigada!!!!!!!!


 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")


















