Carregar apresentação
A apresentação está carregando. Por favor, espere

1
C AUSALITY A SSESSMENT OF R EPORTED A DVERSE D RUG R EACTIONS Ana Filipa Macedo Faculty of Health Sciences Portugal

2
Safety is a relative concept No drug which is pharmacologically effective is entirely without hazard Efficacy Safety Quality

3
2000 b.C. – HAMMURABI CODE: “The Doctor who causes death should loose his hands” 500 b.C. – HIPÓCRATES: “Primum non nocere” H ISTORICAL P ERSPECTIVE 200 – GALENO: “Drugs have a main action and a secondary action ”

4
P ERSPECTIVA H ISTÓRICA … 1937 – Sulfanilamide in Dietilenoglicol / Renal Impairment 1961 – Thalidomide / Phocomelia - 10 000 Victims 1971 – Dietilstilbestrol / Vaginal Carcinoma in the daughters, 10 to 20 years after exposition

5
I NTERNATIONAL P HARMACOVIGILANCE S YSTEMS PREMARKETING INVESTIGATION Long Latency ADR Chronic ADR Rare ADR Interactions Risk Groups Limitations POSTMARKETING INVESTIGATION PHARMACOVIGILANCE

6
A DVERSE D RUG R EACTION “a response to a drug which is noxious and unintended, and which occurs at dose normally used in humans for the prophylaxis, diagnosis or therapy of disease, or for a modification of physiological function.” W.H.O 1972

7
E PIDEMIOLOGY OF A DVERSE D RUG R EACTIONS 4 th to 6 th cause of death in U.S.A.,1994 5% of Hospital Admissions 11% of Hospital Patients Doubles costs, length of stay and mortality risk 50% are potentially preventable Less than 1% are reported Medication Error (Preventable) Preventable ADRs ADRs not Preventable Quality Problems Adverse Effects
 Preventable ADRs ADRs not Preventable Quality Problems Adverse Effects")
8
SAFETY MONITORING Identification of a Problem Problem Characterization Benefit – Risk Evaluation Risk Management Communication Decision P HARMACOVIGILANCE

9
I MPUTATION Drug Exposition Reported Adverse Effect “Drug Safety is a field where can be smoke without fire” Waller, P. Dynamic Process

10
D IFFICULT... Complex Nature of Adverse Events Individual Clinical Variability Retrospective Spontaneous Report

11
G LOBAL I NTROSPECTION “ Clinical Judgement of Experts” Subjective Problems of reproducibility Not calibrated

12
D ECISIONAL A LGORITHMS “Systematic Strategies of Decision in Uncertainty Conditions” Explicit Reproducible Simple Possible Automation Improve Reporting

13
1. AD-ADRIAN 2. Aust-Australian 3. By-Bayesiano 4. B-Blanc 5. Ca-Castle 6. Co-Cornelli 7. CPMP- Syst. ABO 8. D-Dangoumau 9. Em-Emanueli 10. Ev-Evreux 11. HM-Hoskins & Maninno 12. HS-Hsu-Stoll 13. I-Irey 14. Ja-Jain 15. Jo-Jones 16. KL-Karch & Lasagna 17. Ki-Kitaguchi 18. Kr-Kramer 19. La-Lagier 20. Lu-Loupi 21. MV-V Maria 22. WHO 23. R-RUCAM 24. Ru-Ruskin 25. St-Stephens 26. Sk-Stricker 27. T-Taiwan 28. V-Venulet 29. W-Weber 30. Wi - Wiholm D ECISIONAL A LGORITHMS

14
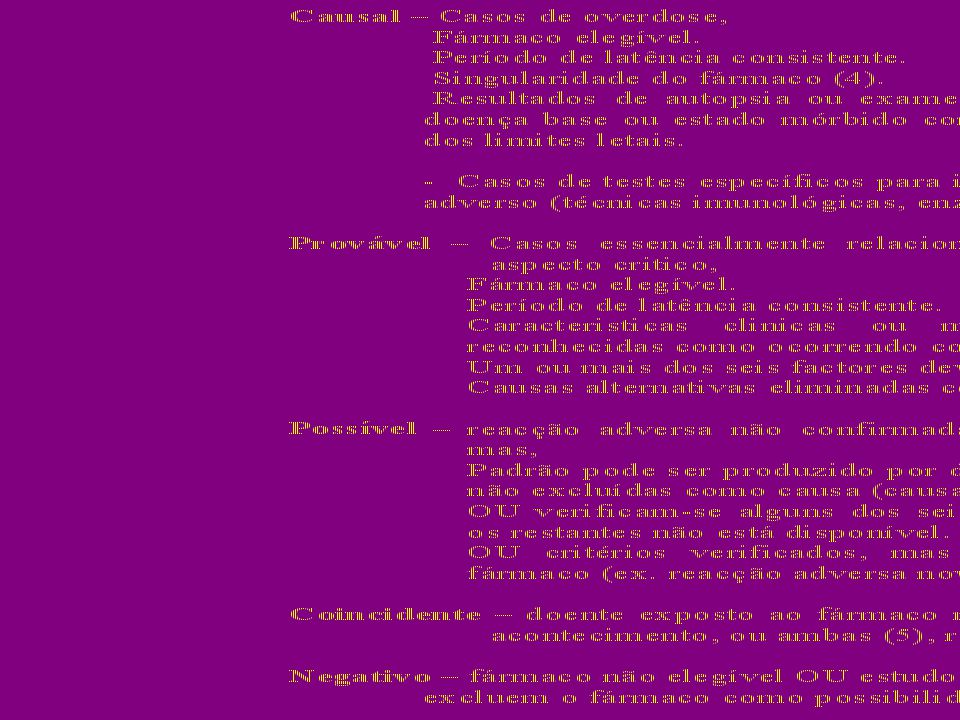
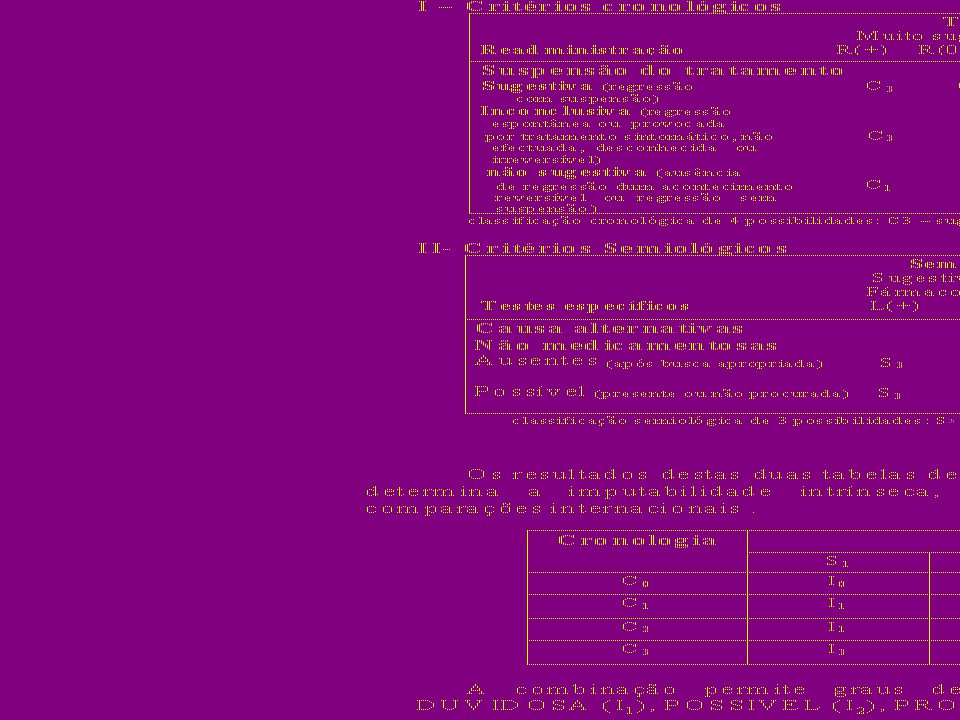
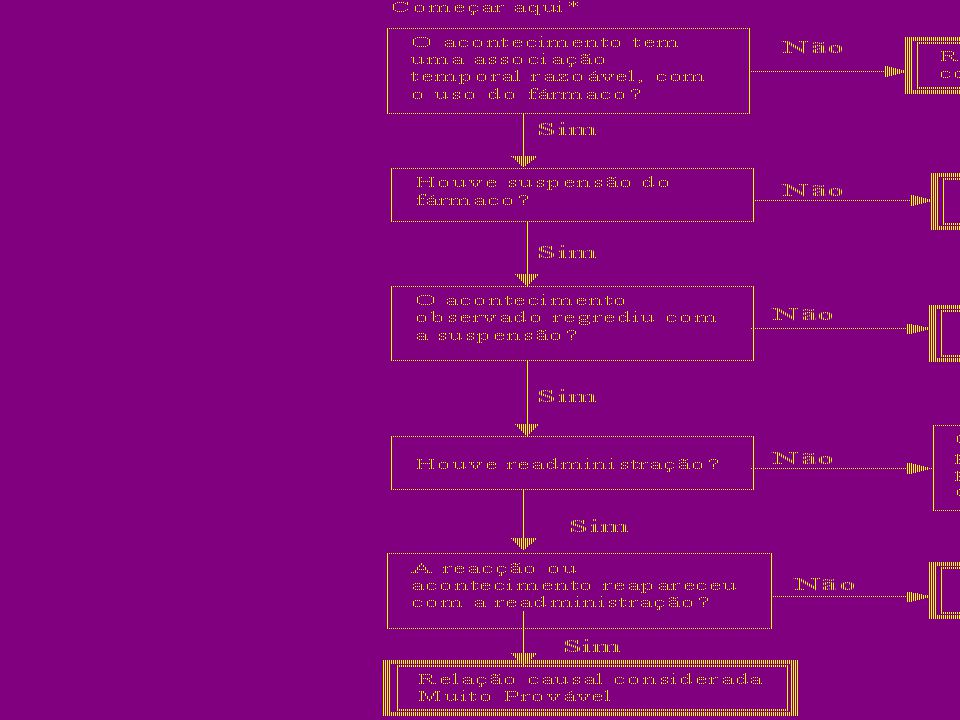
1.Challenge 2.Dechallenge 3.Rechallenge 4.Bibliographic Description Etiologic Alternatives C RITERIA

16
SIMNÃONÃO SEI PONTOS 1. Existem outras notificações conclusivas sobre esta reacção? +100 2. O acontecimento adverso manifestou-se depois da administração do fármaco suspeito? +20 3. A reacção adversa melhorou com suspensão do fármaco ou administração de um antagonista específico? +100 4. A reacção adversa reapareceu com readministração do fármaco? +20 5. Existem causas alternativas (diferentes do fármaco) capazes de provocar a reacção por si mesmas? +20 6. A reacção adversa reapareceu com administração dum placebo? +1 0 7. Foi detectado fármaco no sangue (ou outros fluidos) em concentrações tóxicas? +100 8. A reacção foi mais severa com aumento da dose e menos com a diminuição? +100 9. O doente apresentou uma reacção semelhante ao fármaco ou outros semelhantes em qualquer exposição anterior? +100 10.O acontecimento adverso foi confirmado por qualquer tipo de evidência objectiva? +100 PONTUAÇÃO TOTAL Naranjo et al (1981)
 capazes de provocar a reacção por si mesmas A reacção adversa reapareceu com administração dum placebo Foi detectado fármaco no sangue (ou outros fluidos) em concentrações tóxicas A reacção foi mais severa com aumento da dose e menos com a diminuição O doente apresentou uma reacção semelhante ao fármaco ou outros semelhantes em qualquer exposição anterior O acontecimento adverso foi confirmado por qualquer tipo de evidência objectiva PONTUAÇÃO TOTAL Naranjo et al (1981).")
19
L IMITATIONS Fixed Scoring Arbitrary Scoring Disagreement between algorithms None universally accepted as gold standard

20
C AUSALITY A SSESSMENT G LOBAL I NTROSPECTION S ELECTED A LGORITHMS 1. Aust-Australian 2. B-Blanc 3. Co-Cornelli 4. D-Dangoumau 5. Em-Emanueli 6. HS-Hsu-Stoll 7. I-Irey 8. Jo-Jones 9. KL-Karch & Lasagna 10. Ki-Kitaguchi 11. Kr-Kramer 12. N -Naranjo 13. St-Stephens 14. V-Venulet 15. W-Weber

21
R ESULTS Agreement between algorithms and GI was 43% in average 100% agreement was not found for any algorithm None of the adverse events was equally imputed by all the algorithms Sensitivity 93% and Specificity 7% in average

22
A reference method was not identified Decisional algorithms are not definite alternatives in the individual causality assessment of adverse drug reactions. C ONCLUSIONS

23
D ECISIONAL A LGORITHMS AND Q UANTITATIVE M ETHODS OF S IGNAL D ETECTION Bayesian Confidence Propagation Neural Network (BCPNN) Signal
 Signal")
24
R EFERENCES [1] MACEDO, A.F. [et al.] - Causality assessment of adverse drug reactions: comparison of the results obtained from published decisional algorithms and from the evaluations of an expert panel, according to different levels of imputability. J Clin Pharm Ther.2003. 28: 137-143. [2] STAHL, M. [et al.] – Introducing triage logic as a new strategy for the detection of signals in the WHO Drug Monitoring Database. Pharmacoepidemiol Drug Safe. 2004; 13: 355-363.
![R EFERENCES [1] MACEDO, A.F.](http://images.slideplayer.com.br/10/2674923/slides/slide_24.jpg "[et al.] - Causality assessment of adverse drug reactions: comparison of the results obtained from published decisional algorithms and from the evaluations of an expert panel, according to different levels of imputability. J Clin Pharm Ther : [2] STAHL, M. [et al.] – Introducing triage logic as a new strategy for the detection of signals in the WHO Drug Monitoring Database. Pharmacoepidemiol Drug Safe. 2004; 13:")
Apresentações semelhantes







 2.Comparação.>")











