Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Circulando com o Sangue

2
Schema showing the interaction of risk factors for CKD progression with pathophysiological mechanisms that contribute to a vicious cycle of progressive nephron loss. Ang II – angiotensin II; FSGS – focal and segmental glomerulosclerosis; PGC – glomerular capillary hydraulic pressure; SNGFR – single nephron glomerular filtration rate; TIF – tubulointerstitial fibrosis.

3
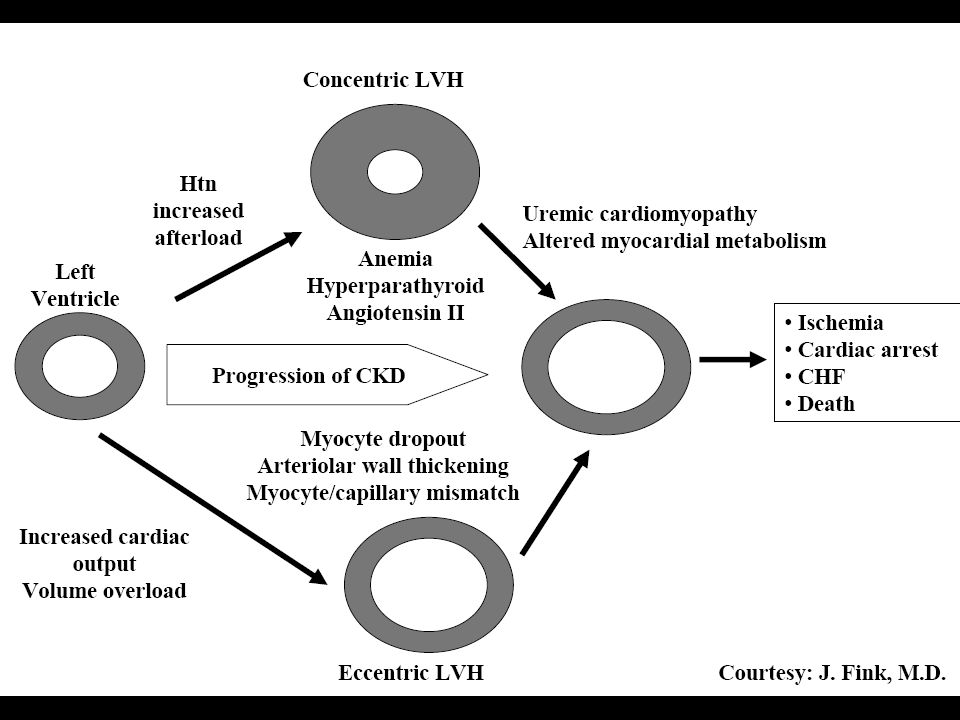
Doença Cardiovascular
IRC associada com aumento do risco CV e Doença CV é também associada com risco aumentado de IRC. Presença de IRC associada com cardiopatia aumenta o risco de morte e de IRCT. IRC e doença CV tem os mesmos fatores de risco: Obesidade, Síndrome Metabólica, DM, HAS, Dislipidemia, Tabagismo. Doença CV afeta diretamente a perfusão renal. Aterosclerose renal foi constatada em 39% de pacientes submetidos à angiografia coronária.

7
Estados de Hiperfiltração
Resposta hemodinâmica capilar à perda de nefrons e hiperglicemia crônica: Aumento da Pressão Hidráulica Capilar Glomerular Aumento da TFG de cada nefro (single) São fatores críticos no estabelecimento do circulo vicioso da perda de nefrons característica da IRC.
 São fatores críticos no estabelecimento do circulo vicioso da perda de nefrons característica da IRC.")
8
Estados de Hiperfiltração: Diminuição do Número de Nefrons
“Dote” de Nefrons Diminuído predispõe à IRC por aumentar a TFG no nefro isolado levando a redução da reserva renal. Baixo peso ao nascer é relacionado com reduzido número de nefrons e com risco para HAS e DM. Déficit Adquirido de Nefrons. Perda focal por extração, doença renal primária, doenças multisistêmicas, exposição a nefrotoxinas e também por adaptações hemodinâmicas nos nefrons remanescentes.

9
Estados de Hiperfiltração: Pressão Arterial
HAS leva a Hipertensão Glomerular que Acelera o Dano Glomerular. HAS é um risco preditivo de IRC. Aumento da PA Sistólica é risco independente. Efeito protetor com controle ótimo: (PA:125X75mmHg). Associação entre HAS e proteinúria: risco aumentado.
. Associação entre HAS e proteinúria: risco aumentado.")
10
Estados de Hiperfiltração: Obesidade e Síndrome Metabólica
Obesidade associada com HAS, proteinúria e doença renal progressiva com hipertensão e hiperfiltração glomerular. Obesidade pode causar glomerulopatia (GESF). Sindrome Metabólica / Resistência à Insulina (obesidade abdominal, dislipidemia, HAS e hiperglicemia de jejum) é risco para IRC proporcional ao número de traços presentes.
. Sindrome Metabólica / Resistência à Insulina (obesidade abdominal, dislipidemia, HAS e hiperglicemia de jejum) é risco para IRC proporcional ao número de traços presentes.")
11
Estados de Hiperfiltração: Alta Ingesta Proteica
Aumenta a TFG levando à alterações hemodinâmicas associadas com hiperfiltração glomerular e acelera a injúria glomerular. Associada com HAS + DM leva à microalbuminúria. Acelera o declínio da função renal. Redução na ingesta proteica tem efeito renoprotetor.

12
Lance D. Dworkin & Douglas G. Shemin
Lance D. Dworkin & Douglas G. Shemin

13
L. Gabriel Navar and L. Lee Hamm

14
L. Gabriel Navar and L. Lee Hamm

15
Marc A. Pohl

16
Physiology of Microvascular Fluid Exchange in the Lung
Ware L and Matthay M. N Engl J Med 2005;353: Figure 1. Physiology of Microvascular Fluid Exchange in the Lung. In the normal lung (Panel A), fluid moves continuously outward from the vascular to the interstitial space according to the net difference between hydrostatic and protein osmotic pressures, as well as to the permeability of the capillary membrane. The following Starling equation for filtration of fluid across a semipermeable membrane describes the factors that determine the amount of fluid leaving the vascular space: Q = K[(Pmv - Ppmv) - ({pi}mv - {pi}pmv)], where Q is the net transvascular flow of fluid, K is the membrane permeability, Pmv is the hydrostatic pressure in the microvessels, Ppmv is the hydrostatic pressure in the perimicrovascular interstitium, {pi}mv is the plasma protein osmotic pressure in the circulation, and {pi}pmv is the protein osmotic pressure in the perimicrovascular interstitium. When hydrostatic pressure increases in the microcirculation, the rate of transvascular fluid filtration rises (Panel B). When lung interstitial pressure exceeds pleural pressure, fluid moves across the visceral pleura, creating pleural effusions. Since the permeability of the capillary endothelium remains normal, the filtered edema fluid leaving the circulation has a low protein content. The removal of edema fluid from the air spaces of the lung depends on active transport of sodium and chloride across the alveolar epithelial barrier. The primary sites of sodium and chloride reabsorption are the epithelial ion channels located on the apical membrane of alveolar epithelial type I and II cells and distal airway epithelia. Sodium is actively extruded into the interstitial space by means of the Na+/K+-ATPase located on the basolateral membrane of type II cells. Water follows passively, probably through aquaporins, which are water channels that are found predominantly on alveolar epithelial type I cells.6 Noncardiogenic pulmonary edema (Panel C) occurs when the permeability of the microvascular membrane increases because of direct or indirect lung injury (including the acute respiratory distress syndrome), resulting in a marked increase in the amount of fluid and protein leaving the vascular space. Noncardiogenic pulmonary edema has a high protein content because the more permeable microvascular membrane has a reduced capacity to restrict the outward movement of larger molecules such as plasma proteins. The degree of alveolar flooding depends on the extent of interstitial edema, the presence or absence of injury to the alveolar epithelium, and the capacity of the alveolar epithelium to actively remove alveolar edema fluid. In edema due to acute lung injury, alveolar epithelial injury commonly causes a decrease in the capacity for the removal of alveolar fluid, delaying the resolution of pulmonary edema.6
, fluid moves continuously outward from the vascular to the interstitial space according to the net difference between hydrostatic and protein osmotic pressures, as well as to the permeability of the capillary membrane. The following Starling equation for filtration of fluid across a semipermeable membrane describes the factors that determine the amount of fluid leaving the vascular space: Q = K[(Pmv - Ppmv) - ({pi}mv - {pi}pmv)], where Q is the net transvascular flow of fluid, K is the membrane permeability, Pmv is the hydrostatic pressure in the microvessels, Ppmv is the hydrostatic pressure in the perimicrovascular interstitium, {pi}mv is the plasma protein osmotic pressure in the circulation, and {pi}pmv is the protein osmotic pressure in the perimicrovascular interstitium. When hydrostatic pressure increases in the microcirculation, the rate of transvascular fluid filtration rises (Panel B). When lung interstitial pressure exceeds pleural pressure, fluid moves across the visceral pleura, creating pleural effusions. Since the permeability of the capillary endothelium remains normal, the filtered edema fluid leaving the circulation has a low protein content. The removal of edema fluid from the air spaces of the lung depends on active transport of sodium and chloride across the alveolar epithelial barrier. The primary sites of sodium and chloride reabsorption are the epithelial ion channels located on the apical membrane of alveolar epithelial type I and II cells and distal airway epithelia. Sodium is actively extruded into the interstitial space by means of the Na+/K+-ATPase located on the basolateral membrane of type II cells. Water follows passively, probably through aquaporins, which are water channels that are found predominantly on alveolar epithelial type I cells.6 Noncardiogenic pulmonary edema (Panel C) occurs when the permeability of the microvascular membrane increases because of direct or indirect lung injury (including the acute respiratory distress syndrome), resulting in a marked increase in the amount of fluid and protein leaving the vascular space. Noncardiogenic pulmonary edema has a high protein content because the more permeable microvascular membrane has a reduced capacity to restrict the outward movement of larger molecules such as plasma proteins. The degree of alveolar flooding depends on the extent of interstitial edema, the presence or absence of injury to the alveolar epithelium, and the capacity of the alveolar epithelium to actively remove alveolar edema fluid. In edema due to acute lung injury, alveolar epithelial injury commonly causes a decrease in the capacity for the removal of alveolar fluid, delaying the resolution of pulmonary edema.6.")
Apresentações semelhantes
















>")





