Carregar apresentação
A apresentação está carregando. Por favor, espere

1
IMPORTÂNCIA DA ATEROSCLEROSE EXTRACARDÍACA PARA O CARDIOLOGISTA
Marcos A. Marino Coordenador do Depto de Hemodinâmica, Cardiologia e Radiologia Vascular Intervencionista Hospital Madre Tereza Belo Horizonte – Minas Gerais

2
DOENÇA ATEROSCLERÓTICA
Aterotrombose Sistêmica 19 milhões de mortes/ano Territórios: Coronariano, Cerebrovascular, Doença Arterial Periférica, Renal.

3
ATEROSCLEROSE EXTRACARDÍACA
Aterosclerose Renal Aterosclerose Periférica Aterosclerose Carotídea Aterosclerose Aórtica (Aneurisma e Obstrução)
")
4
DOENÇA ATEROTROMBÓTICA NOS EUA
Annual Incidence (Millions) Prevalence (Millions) Mortality/Yr (%) Stroke 0.731 4.62 282 TIA 0.503 4.94 6.35 ACS 2.36* 12.62† 452‡ PAD --- 8-127 48,259§ Despite the improvement in the diagnosis and treatment of vascular disease (stroke, MI, and PAD), the incidence of these conditions still remains high. Each year about 730,000 Americans have a new or recurrent stroke, and 28% die from stroke each year, making stroke the third leading cause of death.1,2 In the United States, 4.6 million people have survived a stroke (2.3 million men and 2.3 million women), but 20% require help caring for themselves.2 Latest data from the Mayo Clinic reports that approximately 500,000 TIAs have occurred in the United States in And, according to a recent survey of 10,112 people conducted by the National Stroke Association and Roper Search Worldwide, 4.9 million of all adults age 18 and older (2.9%) have been diagnosed with TIA. Of those surveyed adults 65 years of age and older, 8.5% (or 2.6 million) reported that they had been diagnosed with a TIA.3,4 The average risk for death following a TIA is approximately 6.3%/year.5 MI is the largest single cause of death in the United States. An estimated 1.1 million Americans will have a new or recurrent MI this year, and more than 45% who experience a coronary attack will die within 1 year. Another 550,000 cases of angina will occur each year. Today, an estimated 12.6 million Americans have a history of MI, stable/unstable angina, or both and are at risk for developing subsequent ischemic events.2,4,6 The prevalence of PAD is thought to be even higher than that of MI and stroke. It is estimated that PAD affects approximately 8 to 12 million Americans.7 The mortality rate for established PAD is estimated to be approximately 4% per year.8 Patients with critical limb ischemia who have the lowest ankle-brachial index have an annual mortality of 25%.9 1. Broderick J, Brott T, Kothari R, et al. The greater Cincinnati/Northern Kentucky stroke study: preliminary first-ever and total incidence rates of stroke among blacks. Stroke. 1998;29: 2.American Heart Association Heart and Stroke Statistical Update. Dallas, Tex: American Heart Association; 2001. 3.Brown et al. American Stroke Association. 25th Int. Stroke Conference 4.National Stroke Assocation Press Release, April 25, 2000. 5.Dennis M, Bamford J, Sandercock P, Warlow C. Prognosis of transient ischemic attacks in the Oxfordshire Community Stroke Project. Stroke. 1990;21: 6.National Hospital Discharge Survey National Center for Health Statistics/Centers for Disease Control and Prevention. Series 13, No September 2001. 7.Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286: 8.Dormandy JA, Murray GD. The fate of the claudicant: a prospective study of 1969 claudicants. Eur J Vasc Surg. 1991;5: 9.Hiatt WR. Medical treatment of peripheral arterial disease and claudication. N Engl J Med. 2001;344: TIA = transient ischemic attack; ACS = acute coronary syndrome; PAD = peripheral arterial disease. *Includes unspecified angina pectoris; †includes history of MI or stable/unstable angina pectoris or both; ‡CHD defined as MI or fatal CHD; §patients with critical limb ischemia, who have lowest ABI values, have an annual mortality rate of 25%. 1. Broderick J, et al. Stroke. 1998;29: ; 2. American Heart Association Heart and Stroke Statistical Update; 3. Brown et al. Amer. Stroke Assoc. 25th Int. Stroke Conference. 2000; 4. National Stroke Association Press Release. April 25, 2000; 5. Dennis M, et al. Stroke. 1990;21: ; 6. National Hospital Discharge Survey National Center for Health Statistics/Centers for Disease Control and Prevention. Series 13, No.151. September 2001; 7. Hirsch AT, et al. JAMA. 2001;286: ; 8. Dormandy JA, et al. Eur J Vasc Surg. 1991;5: ; 9. Hiatt WR. N Engl J Med. 2001;344:
 Prevalence (Millions) Mortality/Yr (%) Stroke TIA ACS. 2.36* 12.62† 452‡ PAD ,259§ Despite the improvement in the diagnosis and treatment of vascular disease (stroke, MI, and PAD), the incidence of these conditions still remains high. Each year about 730,000 Americans have a new or recurrent stroke, and 28% die from stroke each year, making stroke the third leading cause of death.1,2 In the United States, 4.6 million people have survived a stroke (2.3 million men and 2.3 million women), but 20% require help caring for themselves.2 Latest data from the Mayo Clinic reports that approximately 500,000 TIAs have occurred in the United States in And, according to a recent survey of 10,112 people conducted by the National Stroke Association and Roper Search Worldwide, 4.9 million of all adults age 18 and older (2.9%) have been diagnosed with TIA. Of those surveyed adults 65 years of age and older, 8.5% (or 2.6 million) reported that they had been diagnosed with a TIA.3,4 The average risk for death following a TIA is approximately 6.3%/year.5. MI is the largest single cause of death in the United States. An estimated 1.1 million Americans will have a new or recurrent MI this year, and more than 45% who experience a coronary attack will die within 1 year. Another 550,000 cases of angina will occur each year. Today, an estimated 12.6 million Americans have a history of MI, stable/unstable angina, or both and are at risk for developing subsequent ischemic events.2,4,6. The prevalence of PAD is thought to be even higher than that of MI and stroke. It is estimated that PAD affects approximately 8 to 12 million Americans.7 The mortality rate for established PAD is estimated to be approximately 4% per year.8 Patients with critical limb ischemia who have the lowest ankle-brachial index have an annual mortality of 25% Broderick J, Brott T, Kothari R, et al. The greater Cincinnati/Northern Kentucky stroke study: preliminary first-ever and total incidence rates of stroke among blacks. Stroke. 1998;29: American Heart Association Heart and Stroke Statistical Update. Dallas, Tex: American Heart Association; Brown et al. American Stroke Association. 25th Int. Stroke Conference National Stroke Assocation Press Release, April 25, Dennis M, Bamford J, Sandercock P, Warlow C. Prognosis of transient ischemic attacks in the Oxfordshire Community Stroke Project. Stroke. 1990;21: National Hospital Discharge Survey National Center for Health Statistics/Centers for Disease Control and Prevention. Series 13, No September Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286: Dormandy JA, Murray GD. The fate of the claudicant: a prospective study of 1969 claudicants. Eur J Vasc Surg. 1991;5: Hiatt WR. Medical treatment of peripheral arterial disease and claudication. N Engl J Med. 2001;344: TIA = transient ischemic attack; ACS = acute coronary syndrome; PAD = peripheral arterial disease. *Includes unspecified angina pectoris; †includes history of MI or stable/unstable angina pectoris or both; ‡CHD defined as MI or fatal CHD; §patients with critical limb ischemia, who have lowest ABI values, have an annual mortality rate of 25%. 1. Broderick J, et al. Stroke. 1998;29: ; 2. American Heart Association Heart and Stroke Statistical Update; 3. Brown et al. Amer. Stroke Assoc. 25th Int. Stroke Conference. 2000; 4. National Stroke Association Press Release. April 25, 2000; 5. Dennis M, et al. Stroke. 1990;21: ; 6. National Hospital Discharge Survey National Center for Health Statistics/Centers for Disease Control and Prevention. Series 13, No.151. September 2001; 7. Hirsch AT, et al. JAMA. 2001;286: ; 8. Dormandy JA, et al. Eur J Vasc Surg. 1991;5: ; 9. Hiatt WR. N Engl J Med. 2001;344:")
5
ESTATÍSTICA DO HOSPITAL MADRE TERESA
Janeiro/2002 – Dezembro/2005 Total de Procedimentos = 3438 ATC coronária: 3207 (93,3%) Intervenção Extra-cardíaca: 231 (6,7%) Carótidas: 85 (2,47%) Renal: 72 (2,09) DAP: 74 (2,15%)
 Intervenção Extra-cardíaca: 231 (6,7%) Carótidas: 85 (2,47%) Renal: 72 (2,09) DAP: 74 (2,15%)")
6
DOENÇA ATEROSCLERÓTICA PERIFÉRICA (DAP)
A DAP é uma doença comum: Ocorre em ~1/3 dos pacientes (Idade acima de 70 anos, Idade acima de 50 anos, tabagista) Forte associação entre DAP, Coronoriopatias e Valvulopatias Risco de IM, AVC. Progressivo em ~25% dos pacientes com Claudicação Intermitente Conseqüências: Diminuição da Qualidade de Vida Amputação de Membros Mortalidade Prematura
 Forte associação entre DAP, Coronoriopatias e Valvulopatias. Risco de IM, AVC. Progressivo em ~25% dos pacientes com Claudicação Intermitente. Conseqüências: Diminuição da Qualidade de Vida. Amputação de Membros. Mortalidade Prematura.")
7
Prevalência de DAP de Grandes Vasos
25 20 15 10 5 Men Women Large-Vessel PAD, % <60 75+ Age Group, y Criqui MH, et al. Circulation. 1985;71:

8
Seqüelas em Pacientes com DAP e Diabetes
60 Diabetes (n=58) 51.7 No Diabetes (n=78) 50 41.4 40 25.6 Percentage of Patients (%) 30 20 11.5 10 Amputation Death Jude EB et al. Diabetes Care. 2001;24:
 No Diabetes (n=78) Percentage of Patients (%) Amputation. Death. Jude EB et al. Diabetes Care. 2001;24:")
9
DAP e Mortalidade* Survival Year 1.00 Normal Subjects 0.75
Asymptomatic LV-PAD† Survival 0.50 Symptomatic LV-PAD† 0.25 Severe Symptomatic LV-PAD† 0.00 2 4 6 8 10 12 Year * Kaplan-Meier survival curves based on mortality from all causes. † Large-vessel PAD. Adapted from Criqui MH et al. N Engl J Med. 1992;326:

10
Índice Tornozelo-Braço
Pressão na Artéria Dorsal do Pé ou Artéria Tibial Posterior ABI= Pressão na Artéria Braquial “Normal”

11
Usando o Índice Tornozelo-Braço
> 0, Normal 0,71 – 0,90 Dano Modesto 0,41 – 0,70 Dano Moderado 0,00 – 0,40 Dano Severo 150 mm Hg Right Arm Pressure 160 mm Hg Left Arm Pressure Right ABI 80/160 = 0.50 Left ABI 120/160 = 0.75 Pressure 40 mm Hg PT 80 mm Hg DP Pressure 120 mm Hg PT 80 mm Hg DP PT, posterior tibial; DP, dorsalis pedis. Newman AB, et al. Circulation. 1993;88:

12
Myocardial Infarctions
Índice Tornozelo-Braquial como um Marcador Para Aterosclerose Myocardial Infarctions Percent With Percent With Strokes N=5084 participants >65 years 5 10 15 20 25 >1.0 to <1.5 >0.9 to <1.0 >0.8 to <0.9 <0.8 RR = 2.7 RR = 2.0 RR = 1.3 2 4 6 8 RR = 1.0 RR = 3.6 RR = 2.6 Newman AB, et al. Circulation. 1993;88:

13
Estudo CAPRIE Índice Tornozelo-Braço Preditor de Eventos Isqüêmicos
ABI – Inverse Relationship with 3-Year Risk of Cardiovascular Events and Deaths 10.2% Relative Risk Increase per 0.1 decrease in ABI (P = 0.041) Dormandy JA. Cerebrovasc Dis. 1999;9 (Suppl 1):1–128.
 Dormandy JA. Cerebrovasc Dis. 1999;9 (Suppl 1):1–128.")
14
Claudicação Intermitente - História Natural em 5 Anos
Population >55 years of age Intermittent claudication 5% 5-year peripheral vascular outcomes Other cardiovascular outcomes Stable claudication 50% Worsening claudication 16% Surgery or tissue loss ≥25% Major amputation < 4% 5-year nonfatal CV events (MI, stroke, etc) 20% 5-year mortality 30% Cardiovascular cause 75% Adapted from Weitz JI, et al. Circulation. 1996;94:
 20% 5-year. mortality. 30% Cardiovascular. cause. 75% Adapted from Weitz JI, et al. Circulation. 1996;94:")
15
Algoritmo para Terapêutica da Claudicação Intermitente
Diagnóstico Confirmatório de Claudicação Intermitente Intervenção Aortoilíaca Sintomas Persistentes/Limitantes Terapia Antiplaquetária Modificação dos fatores de risco para Aterosclerose Agressivo (supervisionado) Programa de Caminhada Cuidado com os Pés Reavaliar Sintomas Persistentes ou Piores
 Programa de Caminhada. Cuidado com os Pés. Reavaliar. Sintomas Persistentes ou Piores.")
16
Algoritmo para Terapêutica da Claudicação Intermitente
Sintomas Persistentes ou Piores Doença Aorto-ilíaca? Doença Infra-inguinal? Clinical Trial: Stent Farmacológico, Braquiterapia Revascularização Cirúrgica Angiogenesis Clinical Trial Pharmacotherapy Clinical Trial Considerar Terapia Endovascular

17
Terapia Endovascular de Escolha
TERAPIA RECOMENDADA NA ESTENOSE/OCLUSÃO DA ARTÉRIA ILÍACA Terapia Endovascular de Escolha <3cm <3cm Type A Terapia Endovascular, mas os dados são insuficientes. 3-10 cm 3-5cm 3-5cm Types B/C Tratamento Cirúrgico de Escolha Type D TASC, J Vasc Surg 2000;31:S1-S296

18
Estratificação da Lesão
Recomendações TASC Estratificação da Lesão Percutânea Tipo A Tipo D Tipo C Tipo B TASC Recommendations: Lesion Stratification The treatment of choice for TASC Type A lesions is an endovascular or percutaneous procedure. For TASC Type D lesions, the treatment of choice is surgery. According to the Consensus Working Group, more evidence is needed to make a firm recommendation about the best treatment for Type B and Type C lesions. It is noted, however, that the practice of vascular surgery is changing rapidly, and that percutaneous interventions are increasingly being done instead of surgery. Management of Peripheral Arterial Disease (PAD). The TASC Working Group. J Vasc Surg. 2000;31:S1-S288. Cirurgia STRIVE TM The TASC Working Group. J Vasc Surg. 2000;31:S1-S288.
. The TASC Working Group. J Vasc Surg. 2000;31:S1-S288. Cirurgia. STRIVE. TM. The TASC Working Group. J Vasc Surg. 2000;31:S1-S288.")
19
DOENÇA FÊMORO-POPLÍTEA
Falta de dispositivos apropriados Durabilidade ? Resultados atuais inferiores aos da cirurgia de revascularização

20
Primary Patency at 1, 3, 5, Years
DURABILIDADE DA INTERVENÇÃO ENDOVASCULAR PARA A DOENÇA ILÍACA E FÊMORO-POPLÍTEA Primary Patency at 1, 3, 5, Years TASC, J Vasc Surg 2000;31:S1-S296

21
44% dos pacientes não melhoraram ou pioraram após a intervenção!
IMPACTO CLÍNICO DA ANGIOPLASTIA FÊMORO-POPLÍTEA 44% dos pacientes não melhoraram ou pioraram após a intervenção! Gray BH, et al. J Vasc Surg 1997;25:74-83

25
CONTUDO, A BASE DA TERAPÊUTICA É….
Exercícios Cilostazol Agentes Antiplaquetários Clopidogrel Identificação de Doenças Ateroscleróticas associadas Identificação de Fatores de Risco

26
ESTENOSE DE ARTÉRIA RENAL
Doença progressiva Tremendos custos para a sociedade Programa de Hemodiálise Americano > $25 bilhões/ano em 2010 Efeitos na qualidade de vida

27
Aumento da Prevalência de EAR
Início da HAS ≤ 30 anos ou ≥ 55 anos HAS Não-controlada/ Maligna (≥ 2 medicamentos) Sopro abdominal Discrepância entre os rins (>1,5 cm) Azotemia com IECA Azotemia com aterosclerose conhecida Edema Pulmonar Doença arterial periférica
 Sopro abdominal. Discrepância entre os rins (>1,5 cm) Azotemia com IECA. Azotemia com aterosclerose conhecida. Edema Pulmonar. Doença arterial periférica.")
28
EAR - PREDITOR INDEPENDENTE DE MORTALIDADE

29
MRA Renal Alta-qualidade

30
INDICAÇÕES PARA ANGIOGRAFIA
Resultados indeterminados ou conflitantes nos testes não invasivos; Teste angiográfico para indicadores predeterminados evidenciados durante a caracterização cardíaca ou angiografia periférica.

31
INCIDÊNCIA DE EAR AO CATETERISMO

32
INCIDÊNCIA DE EAR AO CATETERISMO

33
Rer. Renal: Substrato Típico...

39
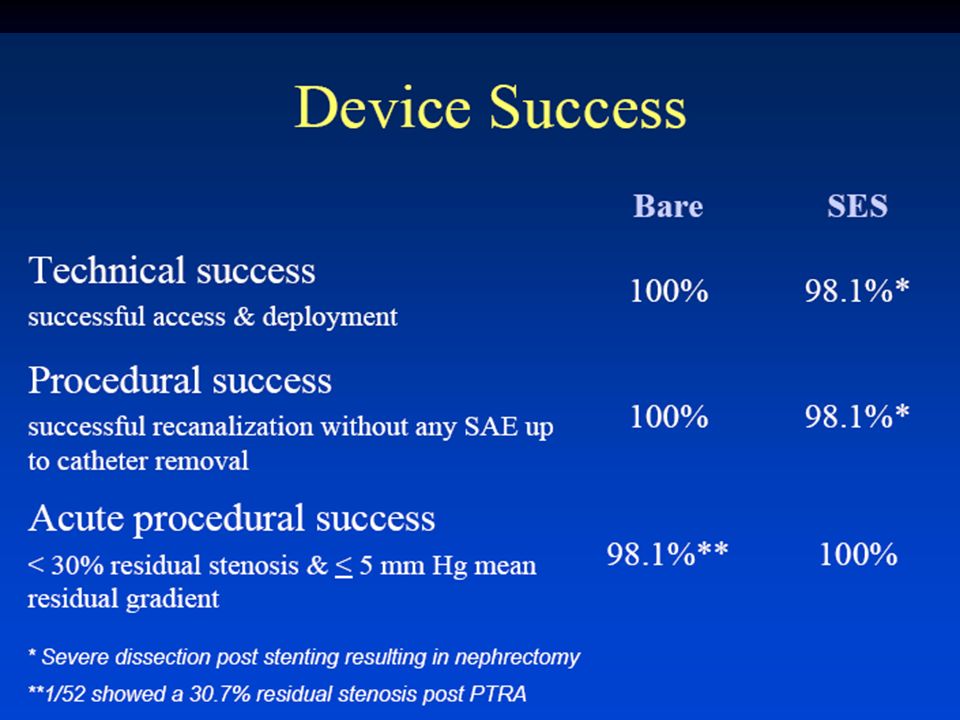
Stent de AR – Sucesso Técnico

40
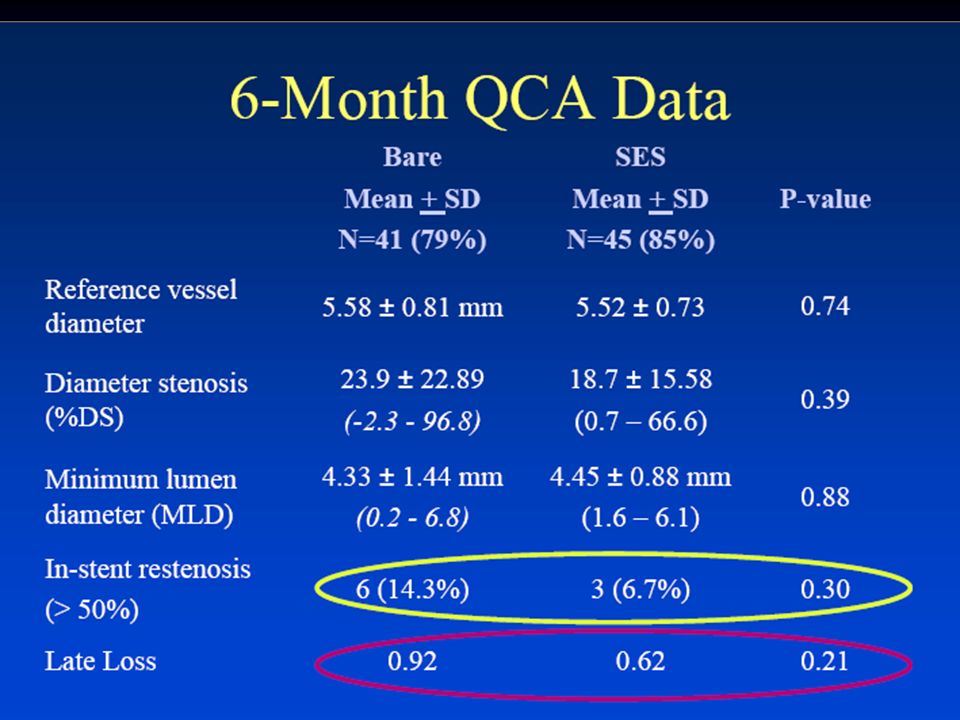
Stent de AR – Reestenose

41
SOBREVIVÊNCIA BASEADO NOS NÍVEIS DE CREATINA SÉRICA

42
Síndromes de Distúrbio Cardíaco Mortalidade (?)
Estenose de Artéria Renal em 2006 Tratamento efetivo por Stenting HAS Preservação Renal Síndromes de Distúrbio Cardíaco Mortalidade (?)
")
48
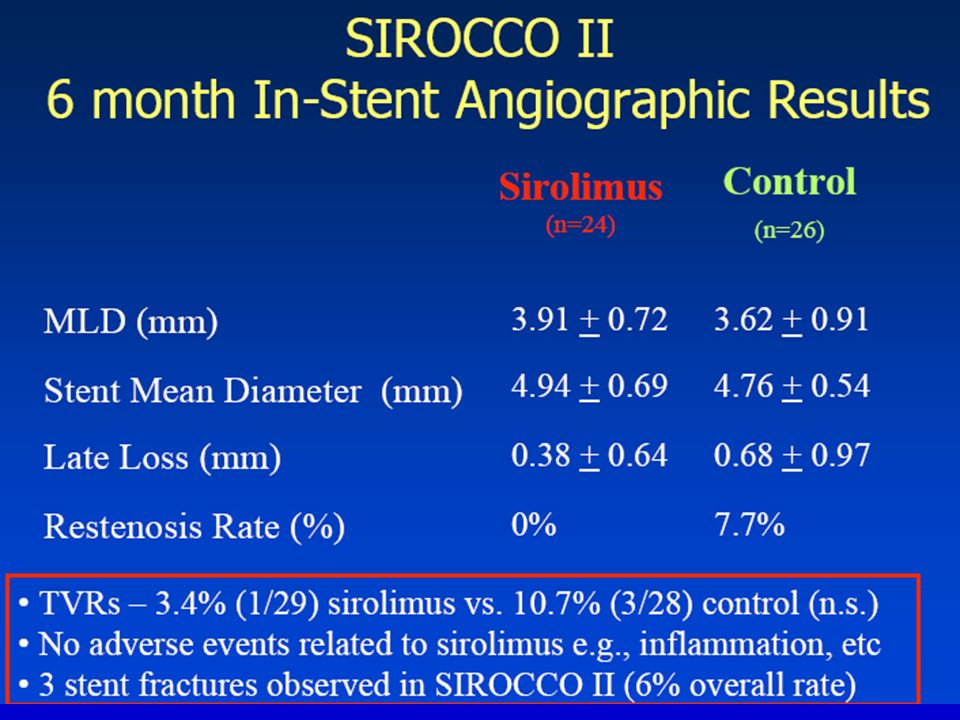
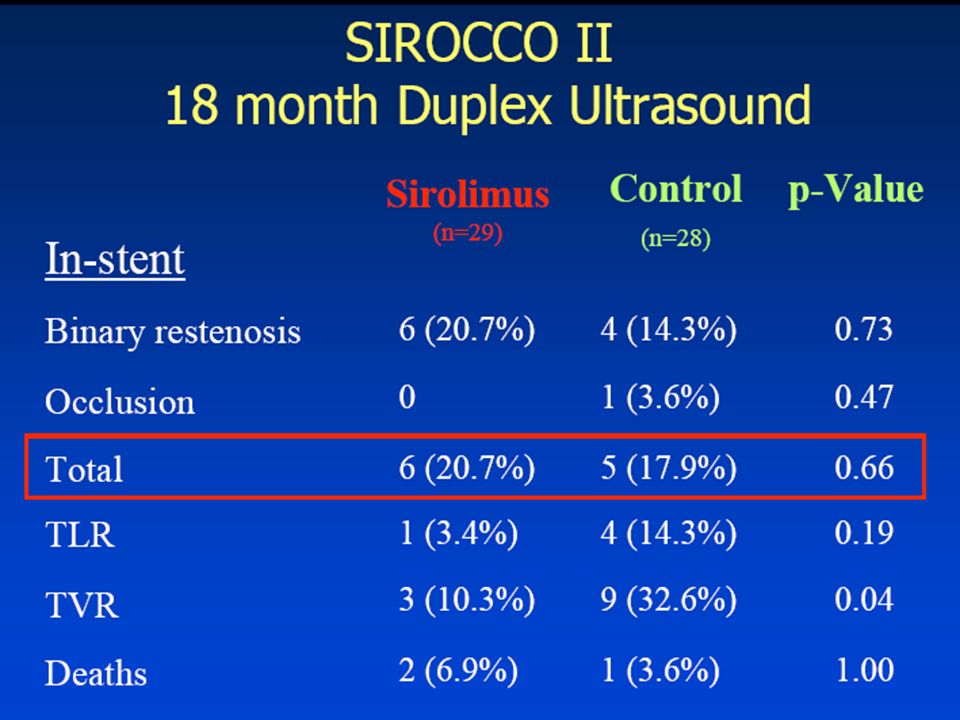
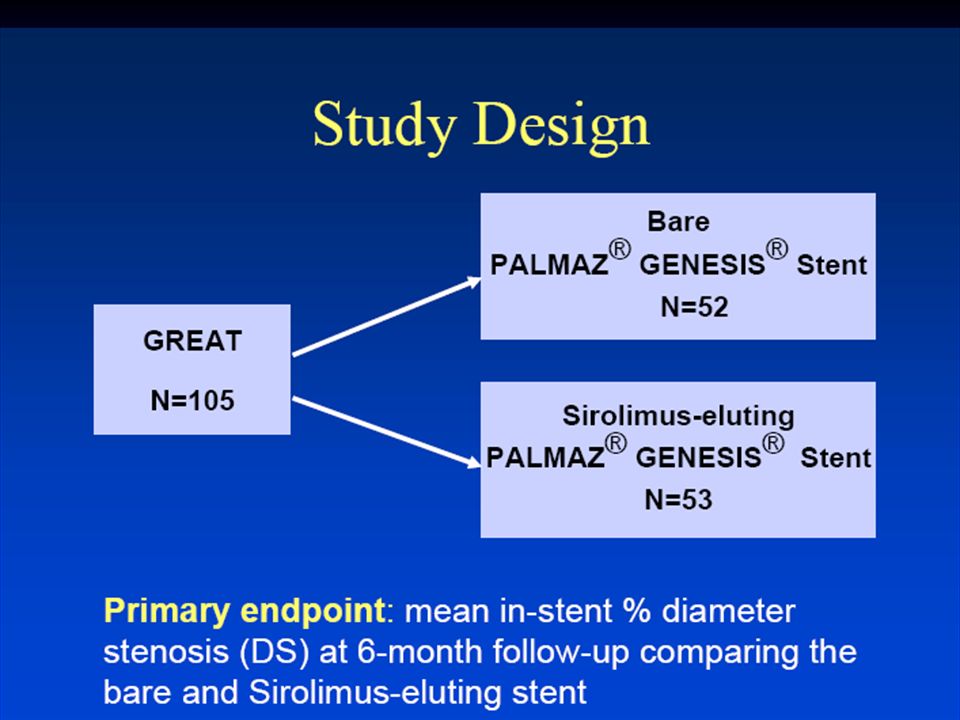
GREAT – Conclusões ... O Stent Farmacológico (SF) diminuiu a taxa reestenose de 14,7% para 6,7%; SF diminuiu o número de revascularizações de 7,7 % para 3,8% - reestenoses agudas foram incomuns; Mais pesquisas clínicas são necessárias com uma maior população de pacientes para investigar o efeito dos SF na evolução clínica.

Apresentações semelhantes







 Dr. Eric J. Topol N. Engl.>")
:679-84. Long-term Outcomes of Patients with Acute Myocardial Infarction Presenting to Hospitals.>")
>")







>")
 – Parte II>")

>")

>")