Carregar apresentação
A apresentação está carregando. Por favor, espere

1
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Carlos A. Gadia, MD Dan Marino Center Miami Children’s Hospital

2
STATEMENT OF POTENTIAL CONFLICTS OF INTEREST
Dr. Carlos Gadia has been a speaker and participated in Medical Advisory Boards for: Elly Lilly Novartis Shire

3
Transtornos do Espectro Autista Tratamento
Intervencão multidisciplinar Terapias de linguagem e comunicacão Técnicas de mudanças de comportamento Programas educativos ou de trabalho

4
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Objetivo do uso de medicações é permitir a criança beneficiar-se das terapias que está recebendo e não de substituí-las. Selecione os sintomas que se quer mudar: Comportamentos Obsesivo-compulsivos/Estereotipias Falta de atenção Comportamentos agressivos/auto-mutilantes Transtornos de sono

5
AUTISMO: Uso e Abuso de Medicações
Exagerar os efeitos da medicação Não estamos tratando autismo Não considerar o custo-benefício para a criança e para a família Uso isolado 6

6
AUTISMO: Uso e Abuso de Medicações
USO CORRETO: Tratamento de sintomas específicos Curta duração de tratamento Possível uso em subgrupos específicos Abrir janelas de oportunidade Permitir maximizar as intervenções sociais-comunicativas-cognitivas-educacionais 6

7
Estudos Duplo-cegos Controlados por Placebo em Autismo/TEA
Anti-psicóticos (n=531) Haloperidol: 4 estudos Risperidona: 4 estudos Aripiprazole: 2 estudo Olanzepina: 1 estudo Fluoxetina: 2 estudos (n=61) Fluvoxamina: 2 estudos (n=64) Clonidina: 2 estudos (n=15) Clomipramina: 2 estudos (n=15) Buspirona: 1 estudo Metilfenidato: 1 estudo (n=10) Naltrexone: 15 estudos (n= 180) Fenfluramina: 14 estudos (n= 165) Piridoxina (Vitamina B-6): 5 estudos (n= 130) Secretina: 13 estudos (N >500)
 Haloperidol: 4 estudos. Risperidona: 4 estudos. Aripiprazole: 2 estudo. Olanzepina: 1 estudo. Fluoxetina: 2 estudos (n=61) Fluvoxamina: 2 estudos (n=64) Clonidina: 2 estudos (n=15) Clomipramina: 2 estudos (n=15) Buspirona: 1 estudo. Metilfenidato: 1 estudo (n=10) Naltrexone: 15 estudos (n= 180) Fenfluramina: 14 estudos (n= 165) Piridoxina (Vitamina B-6): 5 estudos (n= 130) Secretina: 13 estudos (N >500)")
8
Tratamento Farmacológico: Escolha o Sintoma-Alvo
Falta de Atenção Impulsividade Instabilidade Afetiva Agitação - Agressividade COC Ansiedade Dist. de Sono 8

9
“Dez Mais” Problemas de Comportamento de acordo com Pais e Professores em TEA (n=487)
Pais Professores Facilmente frustrado % % 2. Facilmente distraido 60% % 3. Falta de Atenção 54% % 4. Teimosia % % 5. Dificuldade de Concentração 49% % 6. Hiperatividade % % 7. Repetição Compulssiva 41% % 8. Auto-isolamento 36% % 9. Hipersensibilidade 32% % 10. Estereotipia de Mãos 31% % Lecavalier (2006) J Aut Dev Disord Usando 66-itens Nisonger Child Behavior Rating Form
 J Aut Dev Disord. Usando 66-itens Nisonger Child Behavior Rating Form.")
10
TIPOLOGIA E FARMACOLOGIA
Comportamentos agressivos Comportamentos auto-mutilantes Irritabilidade NEUROLÉPTICOS Haloperidol Risperidona* Olanzepina Quetiapina Ziprasidona Aripiprazole* *Aprovados pelo FDA para uso em crianças autistas

11
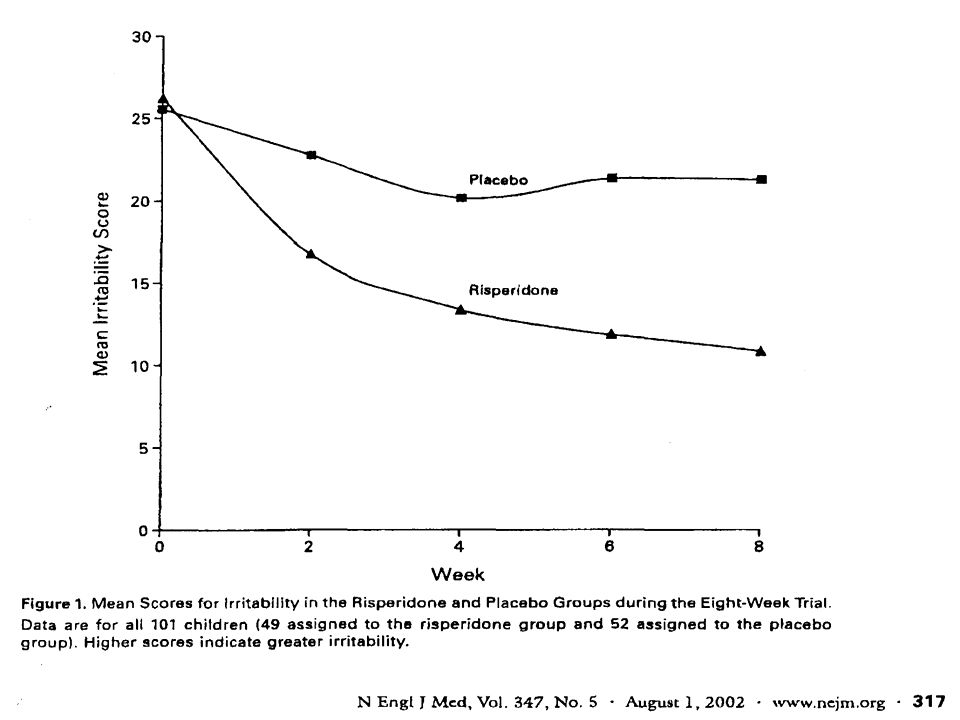
NEJM 347(5): , Aug 1, 2002
: , Aug 1, 2002")
12
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Estudo de Risperidona (RUPP) Fase 1: 8 semanas, duplo-cIego, randomizado, controlado por placebo Fase 2: 4 meses, estudo aberto de extensão: Grupo de crianças sem reposta tratados com placebo Grupo de crianças com resposta tratados com Risperidona Fase 3: 2 meses, descontinuação controlada por placebo 101 crianças: 82 M, 19 F Risperidona = 49 Placebo = 52 Idade média: 8.8 a ( 5 to 17) Sem diferenças significativas intra-grupos em outras medições RUPP Autism Netmork N Engl J Med ; 347:
 Fase 1: 8 semanas, duplo-cIego, randomizado, controlado por placebo. Fase 2: 4 meses, estudo aberto de extensão: Grupo de crianças sem reposta tratados com placebo. Grupo de crianças com resposta tratados com Risperidona. Fase 3: 2 meses, descontinuação controlada por placebo. 101 crianças: 82 M, 19 F. Risperidona = 49 Placebo = 52. Idade média: 8.8 a ( 5 to 17) Sem diferenças significativas intra-grupos em outras medições. RUPP Autism Netmork N Engl J Med ; 347:")
15
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Estudo de Risperidona - Protocolo II (RUPP Autism Network) Fase 2: 4 meses, estudo aberto de extensão para Grupo de crianças sem resposta tratados com placebo Grupo de crianças com resposta tratados com Risperidona Fase 3: 2 meses, descontinuação controlada por placebo Melhora nas medidas de irritabilidade se mantiveram Efeito colateral mais importante: ganho de peso 5.6kg ± 3.9kg > 2 primeiros meses (1.4 kg/mês ± 0.88 kg/mes)
 Fase 2: 4 meses, estudo aberto de extensão para. Grupo de crianças sem resposta tratados com placebo. Grupo de crianças com resposta tratados com Risperidona. Fase 3: 2 meses, descontinuação controlada por placebo. Melhora nas medidas de irritabilidade se mantiveram. Efeito colateral mais importante: ganho de peso 5.6kg ± 3.9kg. > 2 primeiros meses (1.4 kg/mês ± 0.88 kg/mes)")
17
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Risperidona RUPP 2005 Estudo de Extensão Recorrencia dos Sintomas após Discontinuação RUPP Autism Network (2005): Am J Psychiatry 162:1361-9
: Am J Psychiatry 162:")
18
Risperidona em Autismo
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA Risperidona em Autismo Sólida evidencia de melhora de comportamento agressivo, irritabilidade e comportamentos auto-mutilantes e mudanças de humor em estudos DCPC Bem tolerada e efetiva por até 6 meses Necessário monitorar movimentos involuntários, ganho de peso e síndrome metabólica

19
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
l Aripiprazole em Autismo 14-semanas estudo aberto ( 6 semanas de ajuste de dose; 8 semanas de manutenção) 25 jovens (5-17 anos; média 8.6 anos) QI (média 84) Sem outras medicações ABC Irritabilidade > 18 Dose final mg/dia (média 7.8 mg/d) Ganho de peso médio 2.3 kg ( -1.5 a +3.5 kg) 22/25 (88%) “melhor” ou muito melhor” com redução > 25% no ABC-I Stigler et al. J Child Adolesc Psychopharmacology, (3):265-74
 25 jovens (5-17 anos; média 8.6 anos) QI (média 84) Sem outras medicações. ABC Irritabilidade > 18. Dose final mg/dia (média 7.8 mg/d) Ganho de peso médio 2.3 kg ( -1.5 a +3.5 kg) 22/25 (88%) melhor ou muito melhor com redução > 25% no ABC-I. Stigler et al. J Child Adolesc Psychopharmacology, (3):")
20
AUTISTIC SPECTRUM DISORDERS PHARMACOTERAPY
Aripiprazole em Autismo A Placebo-Controlled, Fixed-Dose Study of Aripiprazole in Children and Adolescents With Irritability Associated With Autistic Disorder RONALD N. MARCUS, M.D., RANDALL OWEN, M.D., LISA KAMEN, M.H.A., GEORGE MANOS, PH.D., ROBERT D. MCQUADE, PH.D.,WILLIAM H. CARSON, M.D., AND MICHAEL G. AMAN, PH.D

21
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
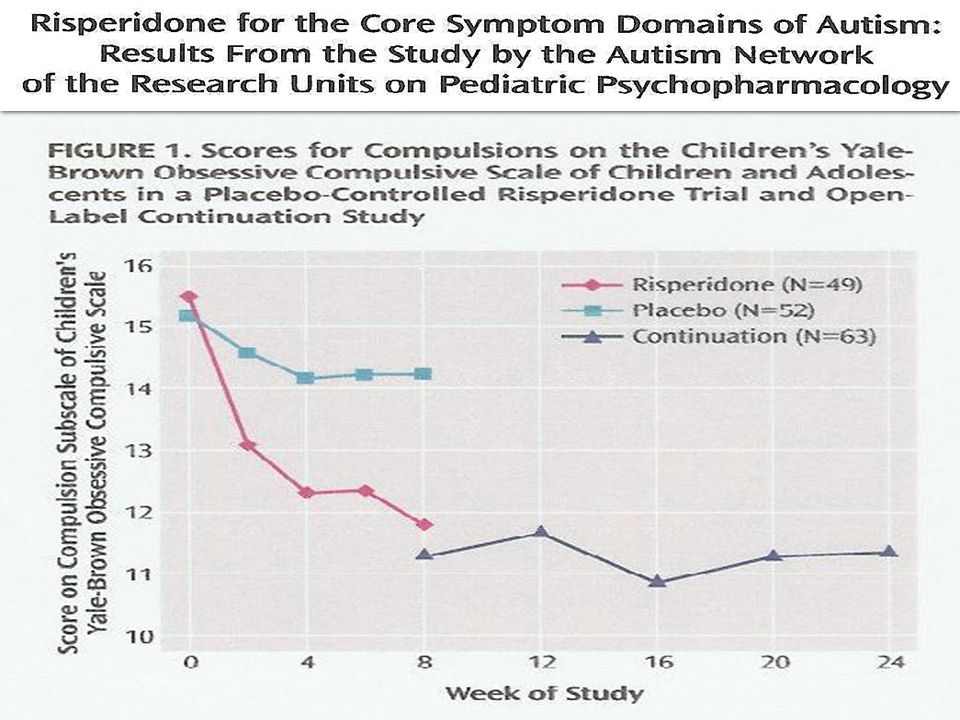
Aripiprazole em Autismo Estudo DCPC: 218 autistas (idade média 10 anos) 8 semanas de dose fixa de aripiprazole (5, 10, 15 mg) Medida primária de eficácia : ABC-I ; Pela 8a semana os 3 grupos (5, 10, 15mg) separaram de placebo Medidas secondárias: - Estereotipias/Hiperatividade: 8a semana os 3 grupos separaram de placebo - Letargia/Isolamento Social: sem diferença x placebo - Children’s Yale-Brown OC : grupo de 15mg melhor que placebo pela 8a. semana Efeitos colaterais (> 10% e 2x > placebo) - Sedação, sintomas extrapiramidais - Ganho de peso: 1.5 kg x 0.4kg placebo (40% < estudo comparavel com risperidona) Marcus R et al.Journal of the American Academy of Child and Adolescent Psychiatry 2009; 48:
 8 semanas de dose fixa de aripiprazole (5, 10, 15 mg) Medida primária de eficácia : ABC-I ; Pela 8a semana os 3 grupos (5, 10, 15mg) separaram de placebo. Medidas secondárias: - Estereotipias/Hiperatividade: 8a semana os 3 grupos separaram de placebo. - Letargia/Isolamento Social: sem diferença x placebo. - Children’s Yale-Brown OC : grupo de 15mg melhor que placebo pela 8a. semana. Efeitos colaterais (> 10% e 2x > placebo) - Sedação, sintomas extrapiramidais. - Ganho de peso: 1.5 kg x 0.4kg placebo (40% < estudo comparavel com risperidona) Marcus R et al.Journal of the American Academy of Child and Adolescent Psychiatry 2009; 48:")
22
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Aripiprazole em Autismo Estudo DCPC: 98 autistas (idade média 9 anos) 8 semanas de doses flexíveis de aripiprazole: começando com 2mg e aumentando até 15 mg se necessário (dose média 8.5mg) Medidas primárias de eficácia : ABC-I e CGI A partir da 1a semana o grupo com medicação separou de placebo Efeitos colaterais (> 5% e 2x > placebo) - Sedação, sintomas extrapiramidais - Ganho de peso: 1.9 kg x 0.5kg placebo (20% < estudo comparavel com risperidona) Owen, R. et al. Pediatrics 2009;124:
 8 semanas de doses flexíveis de aripiprazole: começando com 2mg e. aumentando até 15 mg se necessário (dose média 8.5mg) Medidas primárias de eficácia : ABC-I e CGI. A partir da 1a semana o grupo com medicação separou de placebo. Efeitos colaterais (> 5% e 2x > placebo) - Sedação, sintomas extrapiramidais. - Ganho de peso: 1.9 kg x 0.5kg placebo (20% < estudo comparavel com risperidona) Owen, R. et al. Pediatrics 2009;124:")
23
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Efeitos Colaterais Ganho de Peso Efeitos Colaterais Sérios Risperidona Sim Hepatotoxicidade ↑ prolactina Quetiapina Sim Convulsões ↑ QTc Olanzapina Sim ↑ triglicerídios ↑ Risco Diabetes tipo2 Ziprasidona Não ↑ QTc

24
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Antipsicóticos Atípicos Utilizados em uma variedade de problemas em crianças Importante selecionar comportamentos específicos para avaliar resposta/eficácia risco de SEP, mas ganho de peso é possível; ↑ risco de DM-tipo 2 Sómente para problemas comportamentais severos e com a dose efetiva mas baixa possível Mais estudos são necessários: mono x politerapia combinada a terapias comportamentais

25
TIPOLOGIA E FARMACOLOGIA
Anti-Depressivos Clomipramina Fluoxetina Fluvoxamina Sertralina Citalopram/Escitalopram Estabilizadores de ânimo Depressão Ansiedade Comportamentos Repetitivos Mudança de ânimo Comportamentos Auto-mutilantes

26
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Estudos Controlados de SSRIs em TEA Medicação Amostra Design Resultados Efeitos Colaterais Fluoxetina crianças plac-cont comp. repetitivos sem diferenças Fluoxetina adultos plac-cont ansiedade não descritos Fluvoxamina adultos d-c/plac-cont agressão náusea/sedação comp. repetitivos Fluvoxamina crianças d-c/plac-cont sem diferença insônia com placebo agressividade 1 Hollander et al. Neuropsychopharmacol, 2005 2 Buchsbaum et al. Int J Neuropsychopharmacol, 2001 3 McDougle et al. Arch Gen Psych, 1996 4 McDougle et al. J Autism Dev Disord, 2000

27
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Lack of Efficacy of Citalopram in Children With Autism Spectrum Disorders and High Levels of Repetitive Behavior Bryan H. King, MD; Eric Hollander, MD; Linmarie Sikich, MD; James T. McCracken, MD; Lawrence Scahill, MSN, PhD; Joel D. Bregman, MD; Craig L. Donnelly, MD; Evdokia Anagnostou, MD;Kimberly Dukes, PhD; Lisa Sullivan, PhD; Deborah Hirtz, MD; Ann Wagner, PhD; Louise Ritz, MBA; for the STAART Psychopharmacology Network Arch Gen Psychiatry 2009;66: Percentage of children with a rating of much improved or very much improved on the Clinical Global Impressions, Improvement subscale during the 12-week trial The mean scores on the Children's Yale-Brown Obsessive Compulsive Scales modified for pervasive developmental disorders (CYBOCS-PDD) over time
 over time.")
28
TIPOLOGIA E FARMACOLOGIA
Estimulantes do SNC Metilfenidato D-metilfenidato Sais de Anfetaminas Agonistas Alfa-Adrenérgicos Clonidina Guanfacina Atomoxetina Hiperatividade Impulsividade Desatenção

29
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Estudos com Neuro-estimulantes em TEA Não deixar passar outras possíveis explicações para “sintomas tipo TDAH” Dificuldades de Comunicação Agitação Ansiedade Comportamentos agressivos causados por dificuldades em tolerar transições Estudos mais antigos com Neuro-estimulantes em TEA Anfetaminas: pouco efetivas e pobremente toleradas – Aumento de Estereotipiea – Agressividade Dificuldades para interpretar resultados – Variabilidade Diagnóstica – Crianças muito jovens (idades entre 3-6 anos) – Objetivos pouco claros Campbell et al (1972) J Autism Child Schizophr 2: Campbell et al (1976) Curr Therap Res 19:70-86
 – Objetivos pouco claros. Campbell et al (1972) J Autism Child Schizophr 2: Campbell et al (1976) Curr Therap Res 19:")
30
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Estudos com Neuro-estimulantes em TEA RUPP Autism Network Study of Methylphenidate in Children with PDD+Hyperactivity RUPP Autism Network (2005): Arch Gen Psychiatry 62: Autistas (5-14 anos) e “ sintomas significativos de TDAH ” Período de 7 dias para testar a dose (n=72) 4 semanas: DC crossover; 3 doses de Metifenidato (3x/dia) e placebo (n=66) Baixa ~ mg/kg/dose Media ~ 0.25 mg/kg/dose Alta ~ 0.5 mg/kg/dose ABC Hyperactivity during Continuation in Responders (n=35) Crossover Open-Label Continuation 40 Mean ABC Hyperactivity Subscale Scores 35 30 25 20 15 10 5 Baseline Crossover Phase - Best Week 4 Week 8 Do Parent Teacher Crossover: Parent ABC Hyperactivity 35 30 p = .03 Effect = 0.4 p = .003 Effect = 0.3p < .0001 Effect = 0.5 25 20 15 10 5 Baseline Placebo Low Medium High Mixed Effects Linear Model: Statistically Significant Main Effect of Dose (F = 6.10; p = .0006)
: Arch Gen Psychiatry 62: Autistas (5-14 anos) e sintomas significativos de TDAH Período de 7 dias para testar a dose (n=72) 4 semanas: DC crossover; 3 doses de Metifenidato (3x/dia) e placebo (n=66) Baixa ~ mg/kg/dose. Media ~ 0.25 mg/kg/dose. Alta ~ 0.5 mg/kg/dose. ABC Hyperactivity during Continuation in Responders (n=35) Crossover. Open-Label Continuation. 40. Mean ABC Hyperactivity Subscale Scores Baseline Crossover Phase - Best. Week 4 Week 8. Do. Parent Teacher. Crossover: Parent ABC Hyperactivity p = .03. Effect = 0.4. p = Effect = 0.3p < Effect = Baseline Placebo Low Medium High. Mixed Effects Linear Model: Statistically Significant Main Effect of Dose (F = 6.10; p = .0006)")
31
DCPC crossover:16 crianças com TEA (5-15 anos)
Atomoxetine for hyperactivity in autism spectrum disorders: placebo-controlled crossover pilot trial. Arnold LE, Aman MG, Cook AM, Witwer AN, Hall KL, Thompson S, J Am Acad Child Adolesc Psychiatry Oct;45(10): DCPC crossover:16 crianças com TEA (5-15 anos) 6 semanas(1 semana washout); 2x/dia com doses de até 1.4 mg/kg/d por 3 semanas (dose média 44.2 mg/d) Melhora significativa na escala ABC-H, mas não em atenção 1/16 interrompeu devido a agressividade Resposta positiva: 57% (pais); 43% (professores) - Menor do que em população típica - Similar a neuro-estimulantes no estudo RUPP Menos efeitos colaterais comparando-se com estudos com neuro-estimulantes mas todas as crianças com queixas GI
: DCPC crossover:16 crianças com TEA (5-15 anos) 6 semanas(1 semana washout); 2x/dia com doses de até 1.4 mg/kg/d. por 3 semanas (dose média 44.2 mg/d) Melhora significativa na escala ABC-H, mas não em atenção. 1/16 interrompeu devido a agressividade. Resposta positiva: 57% (pais); 43% (professores) - Menor do que em população típica. - Similar a neuro-estimulantes no estudo RUPP. Menos efeitos colaterais comparando-se com estudos com. neuro-estimulantes mas todas as crianças com queixas GI.")
32
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Agonistas Alfa-Adrenérgicos: Clonidina & Guanfacina Open-Label Guanfacine in Children with PDD Estudo aberto, prospectivo x 8 semanas 27 crianças com TID (5-15 anos) Metilfenidato inefetivo ou não tolerado ↑ de 0.5 mg q4 dias, até um max de 3.5mg/dia ÷ 3x/dia 12/25 (48%) com boa resposta (CGI) Scahill et al. J Child Adolesc Psychopharmacol.16(5): Hiperatividade Impulsividade Falta de Atenção Clonidine treatment of hyperactive and impulsive children with autistic disorder 6 semanas DCPC cross-over: 8 crianças ( 5-13 anos) dose: mg/dia 33% menos irritabilidade no ABC (professor) nenhuma diferença (médicos) Melhora em hiperatividade e estereotipias 4/6 recorrencia em estudo de follow-upJaselskis CA, Cook EH Jr, Fletcher KE, Leventhal BL. J Clin Psychopharmacol.12(5):322-7,1992
 Metilfenidato inefetivo ou não tolerado. ↑ de 0.5 mg q4 dias, até um max de 3.5mg/dia ÷ 3x/dia. 12/25 (48%) com boa resposta (CGI) Scahill et al. J Child Adolesc Psychopharmacol.16(5): Hiperatividade. Impulsividade. Falta de Atenção. Clonidine treatment of hyperactive and impulsive. children with autistic disorder. 6 semanas DCPC cross-over: 8 crianças ( 5-13 anos) dose: mg/dia. 33% menos irritabilidade no ABC (professor) nenhuma diferença (médicos) Melhora em hiperatividade e estereotipias. 4/6 recorrencia em estudo de follow-upJaselskis CA, Cook EH Jr, Fletcher KE, Leventhal BL. J Clin Psychopharmacol.12(5):322-7,1992.")
33
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Agonistas Alfa-Adrenérgicos: Clonidina & Guanfacina A double-blind, placebo-controlled study of the efficacy of transdermal clonidine in autism Placebo X clonidina em 7 autistas (5-33 anos) Melhora significativa: Clinician and Parent global scales Nenhuma melhora: Conners (pais) Fankhauser MP et al. J ClinPsychiatry: 53(3):77-82, 1992. Hiperatividade Impulsividade Falta de Atenção
 Melhora significativa: Clinician and Parent global scales. Nenhuma melhora: Conners (pais) Fankhauser MP et al. J ClinPsychiatry: 53(3):77-82, Hiperatividade. Impulsividade. Falta de Atenção.")
34
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Distúrbios Do Sono Insonia e distúrbios do ritmo circadiano são muito comuns nos TEA Muito pouca pesquisa em relação a tratamento Medicações comumente usadas: alfa-agonistas, trazodone, antipsicóticos atípicos, benzodiazepínicos Melatonina

35
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Distúrbios Do Sono Melatonina: Dois estudos abertos com criancas autistas 15 crianças Asperger: 3mg (liberação imediata) 30 min antes de deitar x 2 semanas; período de latencia diminuiu em todas durante 2 semanas de tratamento Paavonen et al. J Child Adolesc Psychopharmacol 2003 Combinação de liberação imediata + liberação lenta (3 a 6 mg): melhora em diários de sono/questionários; retorno aos padrões prévios 1 mês após retirada Giannotti et al. J Autism Dev Dis 2006 Níveis de excreção urinária de 6 sulfatoximelatonina mais baixos em crianças com TEA e com correlação negativa com medidas de comunicação social. Tordjman et al al. Biol Psychiatry 2005
 30 min antes de deitar x 2 semanas; período de latencia diminuiu em todas durante 2 semanas de tratamento. Paavonen et al. J Child Adolesc Psychopharmacol Combinação de liberação imediata + liberação lenta (3 a 6 mg): melhora em diários de sono/questionários; retorno aos padrões prévios 1 mês após retirada. Giannotti et al. J Autism Dev Dis Níveis de excreção urinária de 6 sulfatoximelatonina mais baixos em crianças com TEA e com correlação negativa com medidas de comunicação social. Tordjman et al al. Biol Psychiatry")
36
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Descargas Epileptiformes com/sem Convulsões Antiepilépticos/Estabilizadores de ânimo Ácido Valpróico Lamotrogina Topiramato Carbamazepina Gabapentina Imuno-Moduladores ACTH (4-9)Analogos (ORG-2766) Prednisona /ACTH Imunoglobulina EV
Analogos (ORG-2766) Prednisona /ACTH. Imunoglobulina EV.")
37
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Antiepiléticos como Moduladores de Humor ACIDO VALPROICO: Hellings et al. J Child Adolesc Psychopharmacology, 2005: DCPC 8 semanas 30 pacientes com TID (6-32 anos) com agressividade significativa dose 20 mg/kg/dia, nível médio 77.7 Sem diferenças significtivas no ABC (Irritabilidade ou Agressão) Aumento significativo do apetite Hollander et al. Int J Neuropsychophrmacol, 2006 DCPC, 8 semanas 13 pacientes com TEA (idade média 9 anos) Dose média: mg/dia Melhora em comportamentos repetitivos (CY-BOCS)
 com agressividade significativa. dose 20 mg/kg/dia, nível médio Sem diferenças significtivas no ABC (Irritabilidade ou Agressão) Aumento significativo do apetite. Hollander et al. Int J Neuropsychophrmacol, DCPC, 8 semanas. 13 pacientes com TEA (idade média 9 anos) Dose média: mg/dia. Melhora em comportamentos repetitivos (CY-BOCS)")
38
TRANSTORNOS DO ESPECTRO AUTISTA FARMACOTERAPIA
Antiepiléticos como Moduladores de Humor LAMOTRIGINA Belsito et al. J Aut Dev Disord, 2001 DCPC: 18 semanas, 8 semanas aumento progressivo até 5 mg/kg/dia manutenção por 4 semanas, 2 semanas retirada, 4 semanas sem medicação 28 rianças (3-11 anos) Sem diferenças significativas (ABC Irritabilidade) Sem diferenças significativas em efeitos colaterais LEVETIRACETAN Wasserman et al. Int Clin Psychopharmacology, 2006 DCPC: 20 crianças com TEA (idade média 8.7 anos) Dose média: 863 mg/dia Sem diferença comparado com placebo (ABC-Irritabilidade, pais) in Aumento de irritabilidade (professores) Nenhuma análise estatistica de efeitos colaterais
 Sem diferenças significativas (ABC Irritabilidade) Sem diferenças significativas em efeitos colaterais. LEVETIRACETAN. Wasserman et al. Int Clin Psychopharmacology, DCPC: 20 crianças com TEA (idade média 8.7 anos) Dose média: 863 mg/dia. Sem diferença comparado com placebo (ABC-Irritabilidade, pais) in. Aumento de irritabilidade (professores) Nenhuma análise estatistica de efeitos colaterais.")
39
Outras Medicações Estudadas em Autismo
NÃO EFETIVAS Naltrexone: Sistema Endógeno Opioide envolvido em auto-agressão ? Níveis elevados de beta-endorfinas em alguns adultos autistas CAM mantidos pela necessidade de atenuar sensação dolorosa ?? Efeitos modestos em hiperatividade Nenhum efeito em sintomas sociais ou auto-mutilantes Secretina: não demonstrou diferenças significativas comparado com placebo em 5 estudos DCPC NÃO COMPROVADAMENTE EFETIVAS MAS MERECEDORAS DE MAIS ESTUDOS – Agentes Colinérgicos (Donepezil, etc) – Agentes Glutamatérgicos (Memantina, etc)
 – Agentes Glutamatérgicos (Memantina, etc)")
40
INTERVENÇÕES FARMACOLÓGICAS É este o futuro?
Farmacogenômica da Risperidona Autistas Controles Using BRB-ArrayTools, a total of 136 genes were identified as being differentially expressed between children with autism on risperidone (four left columns) compared to control children matched for age, sex, and race (right four columns). A supervised cluster analysis of the 136 genes (Y axis) showed complete separation of children with autism on risperidone compared to controls. Hendren and Sharp
 compared to control children matched for age, sex, and race (right four columns). A supervised cluster analysis of the 136 genes (Y axis) showed complete separation of children with autism on risperidone compared to controls. Hendren and Sharp.")
41
INTERVENÇÕES FARMACOLÓGICAS É este o futuro?
INTRANASAL OXYTOCIN IMPROVES EMOTION RECOGNITION FOR YOUTH WITH AUTISM SPECTRUM DISORDERS Guastella AJ et al. Biol Psychiatry, Nov 2009 DCPC 16 pacientes com TEA (12-19 anos) Reading the Mind in the Eyes Task (avalia habilidade de “ler emoções” examinando o olhar em expressões faciais afetivas sutis) Dose única, 18 or 24 IU, 45 minutos antes do teste
 Reading the Mind in the Eyes Task. (avalia habilidade de ler emoções examinando o olhar em expressões faciais afetivas sutis) Dose única, 18 or 24 IU, 45 minutos antes do teste.")
42
Oxytocin Enhances Amygdala-Dependent, Socially -Reinforced
Oxytocin Enhances Amygdala-Dependent, Socially -Reinforced Learning and Emotional Empathy in Humans Hullerman et all.The Journal of Neuroscience, April 7, 2010 Figure 2. RALT. A, Letters “A” and “B” flanked either a female or a male facial display in social trials and a black circle in nonsocial trials. Subjects judged whether three-digit numerical items presented repeatedly on a computer screen belonged to either category “A” or “B”; visual feedback immediately followed each judgment. Neutral faces changed to happy for correct responses or to angry for incorrect responses in the social condition (S). Black circles changed to green for correct responses or to red for incorrect responses in the nonsocial condition (NS). Bi, Percentage correct responses for the nonsocial condition did not differ between male subjects treated with OT (n24) or placebo (PLC, n24). Bii, Oxytocin increased overall performance up to % above chance level in male subjects, compared to % above chance for placebo controls in the social condition (*p0.05). Biii, Reaction times for the nonsocial condition did not differ between male subjects treated with oxytocin or placebo. Biv, Reaction times for the social condition did not differ between male subjects treated with oxytocin or placebo. Ci, Percentage correct responses did not differ between two UW patients and controls (CTRL, n16) for the nonsocial condition. Cii, Percentage correct responses decreased in UW patients compared to controls for the social condition (see Results section for Z scores). Ciii, Reaction times did not differ between UW patients and controls for the nonsocial condition. Civ, Reaction times were increased for UW patients compared with controls for the social condition. Significance threshold *p0.05 indicates differences between groups. Error bars indicate SEM.
. Black circles changed to green for correct responses or to red for incorrect responses in the nonsocial condition (NS). Bi, Percentage correct responses for the nonsocial condition did not differ between male subjects treated with OT (n24) or placebo (PLC, n24). Bii, Oxytocin increased overall performance up to % above chance level in male subjects, compared to % above chance for placebo controls in the social condition (*p0.05). Biii, Reaction times for the nonsocial condition did not differ between male subjects treated with oxytocin or placebo. Biv, Reaction times for the social condition did not differ between male subjects treated with oxytocin or placebo. Ci, Percentage correct responses did not differ between two UW patients and controls (CTRL, n16) for the nonsocial condition. Cii, Percentage correct responses decreased in UW patients compared to controls for the social condition (see Results section for Z scores). Ciii, Reaction times did not differ between UW patients and controls for the nonsocial condition. Civ, Reaction times were increased for UW patients compared with controls for the social condition. Significance threshold *p0.05 indicates differences between groups. Error bars indicate SEM.")
43
PROMOTING SOCIAL BEHAVIOR WITH OXYTOCIN IN HIGH-FUNCTIONING AUTISM SPECTRUM DISORDERS Andari E et al. Proc Natl Acad Sci, Feb 2010

44
A pilot open label, single dose trial of
Fenobam in adults with fragile X syndrome Berry-Kravis et al. J Med Genet 2009 Conclusions: Clinically significant adverse effects were not identified in this study of single dose fenobam across the range of dosages utilised. The positive effects seen in animal models of FXS treated with fenobam or other mGluR5 antagonists, the apparent lack of clinically significant adverse effects, and the potential beneficial clinical effects seen in this pilot trial support further study of the compound in adults with FXS.

45
Mechanism-based approaches to treating fragile X. Gül Dölen et al
Mechanism-based approaches to treating fragile X. Gül Dölen et al. Pharmacology and Therapeutics, 2010 in press Studies in Progress: A Randomized, Double-blind, Placebo-controlled, Pharmacokinetic, Safety and Tolerability, and Exploratory Efficacy and Pharmacodynamic Effects Study of RO in Adult Patients With Fragile X Syndrome (Roche) A Multi-Centre, Randomized, Double-Blind, Placebo Controlled, Two-Period, Crossover Proof-of-Concept Study in Male Patients With Fragile X Syndrome to Assess the Efficacy, Safety and Tolerability of Multiple Oral Doses of AFQ056 (Novartis) Study Finished (no published results): A Single-Dose, Randomized, Double-Blind, Placebo-Controlled, Dose-Escalation Study in Healthy, Normal Volunteers to Assess the Safety, Tolerability and Pharmacokinetics of STX107
 A Multi-Centre, Randomized, Double-Blind, Placebo Controlled, Two-Period, Crossover Proof-of-Concept Study in Male Patients With Fragile X Syndrome to Assess the Efficacy, Safety and Tolerability of Multiple Oral Doses of AFQ056 (Novartis) Study Finished (no published results): A Single-Dose, Randomized, Double-Blind, Placebo-Controlled, Dose-Escalation Study in Healthy, Normal Volunteers to Assess the Safety, Tolerability and Pharmacokinetics of STX107.")
46
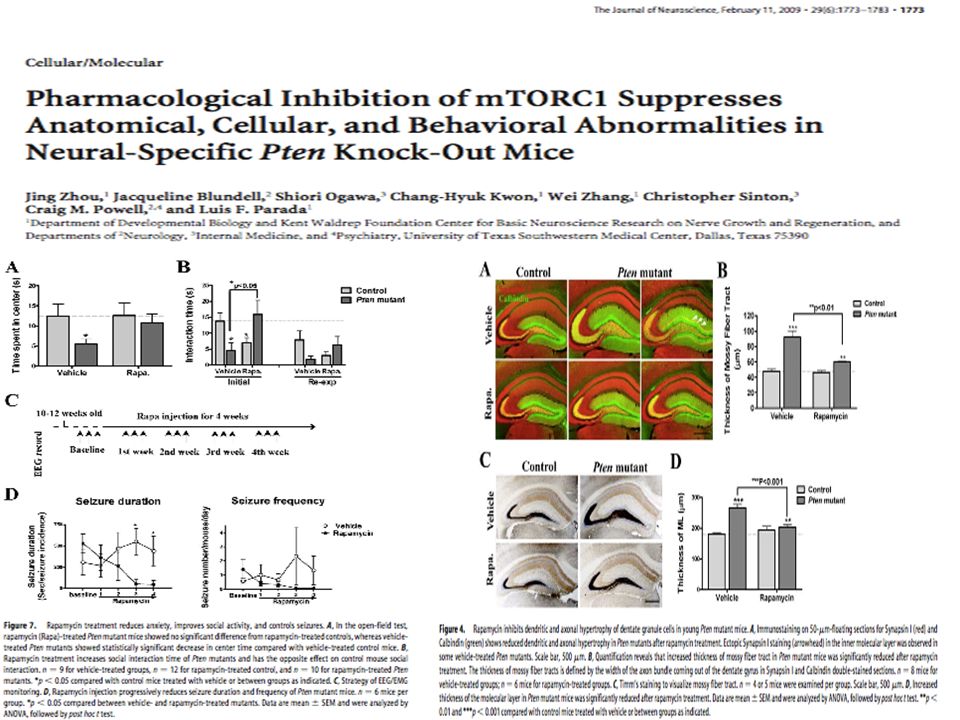
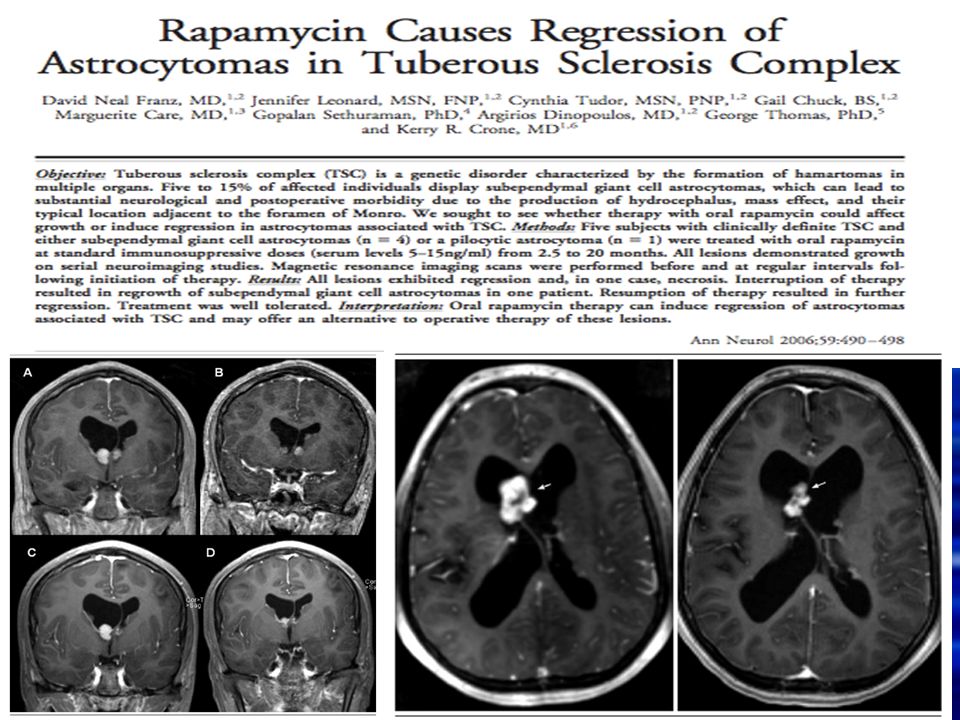
mTOR signaling: At the crossroads of plasticity, memory and disease Hoefer C & Klann E. Trends in Neurosiences, 2009 Franz et al. Ann Neurol 2006

49
Já fiz meu diagnóstico pela internet.
Estou aqui para uma segunda opinião.

50
and the effects of IGF-1 treatment
Changes in organismal physiology in MeCP2 mutant mice and the effects of IGF-1 treatment Changes in organismal physiology in MeCP2 mutant mice and the effects of IGF-1 treatment. (A) Lifespan as measured by Kaplan-Meier survival curves, showing the proportion of mice that survived (y axis) at each day after birth (x axis) for nontreated (KO) and treated (KO-T) mice. MeCP2 knockout mice treated with (1–3)IGF-1 daily from P15 onward exhibited a significantly longer life expectancy that their littermates (KO, n = 26 mice; KO-T, n = 21 mice; P < , log rank test). (B) Locomotor function, measured by placing animals in cages equipped with infrared beams to quantify nocturnal movement. The y axis shows the number of beam crossings over 10 h in mice aged 8–9 weeks. Compared to wild-type (WT), MeCP2 knockout mice (KO) showed significantly less activity. However, KO mice treated with (1–3)IGF-1 from P15 onward (KO-T) were more active than vehicle-treated KO animals (WT, ± beam crossings, n = 17 mice; KO, ± 6893 crossings, n = 17 mice; KO-T, ± crossings, n = 39 mice; WT vs. KO P < ; KO vs. KO-T P < 0.001, 2-tailed t test). ***: P < (C) Breathing variability, assessed by measuring breaths per minute with an oximeter and quantifying the change from one measurement interval (15 seconds) to the next. Comparisons are between 8-week-old mice. MeCP2 KO mice showed increased breathing variability (larger changes per interval) than wild-type littermates (WT, 6.0 ± 0.6 breaths/minute, 630 measurements, n = 13 mice; KO, 15.4 ± 1.1 breaths/minute, 975 measurements, n = 17 mice; P < , Kolmogorov-Smirnov test). KO-T mice, treated from P15 for 6 weeks, showed decreased variability (smaller changes per interval) than KO (KO-T, 12.3 ± 0.8 breaths/minute, 1292 measurements, n = 24 mice; KO-T vs. KO P < 0.01, Kolmogorov-Smirnov test). (D) Pooled heart rate distributions observed across mice from different treatments (in beats per minute). Comparisons are between 8-week-old mice (WT, KO, and animals which received (1–3)IGF-1 treatment from P:15 for 6 weeks, KO-T). The KO distribution (pink) was left-shifted compared to the wild-type distribution (black), indicating a significant reduction in the distribution of heart rates (WT, n = samples, n = 5 mice; KO, samples, n = 5 mice; P < , Kolmogorov-Smirnov test). The KO-T distribution (green) was in-between the two curves (KO-T, samples, n = 9 mice; KO-T vs. KO P < , Kolmogorov-Smirnov test), indicating a partial rescue of the KO phenotype toward a more normal wild-type distribution. Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences
 Lifespan as measured by Kaplan-Meier survival curves, showing the proportion of mice that survived (y axis) at each day after birth (x axis) for nontreated (KO) and treated (KO-T) mice. MeCP2 knockout mice treated with (1–3)IGF-1 daily from P15 onward exhibited a significantly longer life expectancy that their littermates (KO, n = 26 mice; KO-T, n = 21 mice; P < , log rank test). (B) Locomotor function, measured by placing animals in cages equipped with infrared beams to quantify nocturnal movement. The y axis shows the number of beam crossings over 10 h in mice aged 8–9 weeks. Compared to wild-type (WT), MeCP2 knockout mice (KO) showed significantly less activity. However, KO mice treated with (1–3)IGF-1 from P15 onward (KO-T) were more active than vehicle-treated KO animals (WT, ± beam crossings, n = 17 mice; KO, ± 6893 crossings, n = 17 mice; KO-T, ± crossings, n = 39 mice; WT vs. KO P < ; KO vs. KO-T P < 0.001, 2-tailed t test). ***: P < (C) Breathing variability, assessed by measuring breaths per minute with an oximeter and quantifying the change from one measurement interval (15 seconds) to the next. Comparisons are between 8-week-old mice. MeCP2 KO mice showed increased breathing variability (larger changes per interval) than wild-type littermates (WT, 6.0 ± 0.6 breaths/minute, 630 measurements, n = 13 mice; KO, 15.4 ± 1.1 breaths/minute, 975 measurements, n = 17 mice; P < , Kolmogorov-Smirnov test). KO-T mice, treated from P15 for 6 weeks, showed decreased variability (smaller changes per interval) than KO (KO-T, 12.3 ± 0.8 breaths/minute, 1292 measurements, n = 24 mice; KO-T vs. KO P < 0.01, Kolmogorov-Smirnov test). (D) Pooled heart rate distributions observed across mice from different treatments (in beats per minute). Comparisons are between 8-week-old mice (WT, KO, and animals which received (1–3)IGF-1 treatment from P:15 for 6 weeks, KO-T). The KO distribution (pink) was left-shifted compared to the wild-type distribution (black), indicating a significant reduction in the distribution of heart rates (WT, n = samples, n = 5 mice; KO, samples, n = 5 mice; P < , Kolmogorov-Smirnov test). The KO-T distribution (green) was in-between the two curves (KO-T, samples, n = 9 mice; KO-T vs. KO P < , Kolmogorov-Smirnov test), indicating a partial rescue of the KO phenotype toward a more normal wild-type distribution. Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences.")
51
Changes in brain structure in MeCP2 mutant mice
and the effects of IGF-1 treatment Changes in brain structure in MeCP2 mutant mice and the effects of IGF-1 treatment. (A) Mean brain weight of P60 mice that were wild-type (WT), MeCP2 mutant (KO), or mutant treated with (1–3)IGF-1 (KO-T). MeCP2 mutant mice had reduced brain weight (WT, 0.41 ± 0.03 g, n = 10 mice; KO, 0.33 ± 0.02 g, n = 8 mice; P < , two-tailed t test), and brain weight was elevated following treatment with (1–3)IGF-1 from approximately P15 onward (KO-T, 0.36 ± 0.02 g, n = 10 mice; KO vs. KO-T P < 0.05, two-tailed t test). ***: P < ; *: P < (B) Immunostaining in motor cortex layer 5 for the synaptic scaffolding protein PSD-95 in wild-type mice (WT), untreated mutant mice (KO), and mutant mice treated with (1–3)IGF-1 (KO-T). (Scale bar: 25 μm.) (C) Quantitation of PSD-95 immunostaining depicting average labeling intensity normalized to wild-type intensity levels. Mutant animals (KO) exhibited significantly reduced levels of PSD-95 compared to wild-type (WT) (relative KO/WT expression level, 0.43 ± 0.11; P < 0.01, two-tailed t test, comparing WT and KO levels). Treatment with (1–3)IGF-1 (KO-T) increased PSD-95 levels significantly (KO-T/WT expression level, 0.70 ± 0.02; P < 0.05, two-tailed t test, comparing KO and KO-T levels). **: P < 0.01; *: P < (D) Golgi staining of layer 5 pyramidal cells in adult motor cortex to enable specific, sparse labeling of neurons and spine morphology. (Scale bar: 25 μm.) (E) Imaging at higher magnification (100×) to enable clear identification of dendritic spines. (Scale bar: 1.25 μm.) (F) Spine density in adult (P60) animals is reduced in MeCP2 mutant mice and reversed by (1–3)IGF-1 treatment from P15 onward (WT, 1.98 ± 0.14 spines/μm, n = 110 spines, 6 cells, 2 mice; KO, 1.05 ± 0.22 spines/μm, n = 133 spines, 5 cells, 3 mice; KO-T, 1.68 ± 0.14 spines/μm, n = 142 spines, 7 cells, 3 mice; P < 0.05, two-tailed t test, comparing WT vs. KO and KO vs. KO-T). *: P < 0.05. Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences
 Mean brain weight of P60 mice that were wild-type (WT), MeCP2 mutant (KO), or mutant treated with (1–3)IGF-1 (KO-T). MeCP2 mutant mice had reduced brain weight (WT, 0.41 ± 0.03 g, n = 10 mice; KO, 0.33 ± 0.02 g, n = 8 mice; P < , two-tailed t test), and brain weight was elevated following treatment with (1–3)IGF-1 from approximately P15 onward (KO-T, 0.36 ± 0.02 g, n = 10 mice; KO vs. KO-T P < 0.05, two-tailed t test). ***: P < ; *: P < (B) Immunostaining in motor cortex layer 5 for the synaptic scaffolding protein PSD-95 in wild-type mice (WT), untreated mutant mice (KO), and mutant mice treated with (1–3)IGF-1 (KO-T). (Scale bar: 25 μm.) (C) Quantitation of PSD-95 immunostaining depicting average labeling intensity normalized to wild-type intensity levels. Mutant animals (KO) exhibited significantly reduced levels of PSD-95 compared to wild-type (WT) (relative KO/WT expression level, 0.43 ± 0.11; P < 0.01, two-tailed t test, comparing WT and KO levels). Treatment with (1–3)IGF-1 (KO-T) increased PSD-95 levels significantly (KO-T/WT expression level, 0.70 ± 0.02; P < 0.05, two-tailed t test, comparing KO and KO-T levels). **: P < 0.01; *: P < (D) Golgi staining of layer 5 pyramidal cells in adult motor cortex to enable specific, sparse labeling of neurons and spine morphology. (Scale bar: 25 μm.) (E) Imaging at higher magnification (100×) to enable clear identification of dendritic spines. (Scale bar: 1.25 μm.) (F) Spine density in adult (P60) animals is reduced in MeCP2 mutant mice and reversed by (1–3)IGF-1 treatment from P15 onward (WT, 1.98 ± 0.14 spines/μm, n = 110 spines, 6 cells, 2 mice; KO, 1.05 ± 0.22 spines/μm, n = 133 spines, 5 cells, 3 mice; KO-T, 1.68 ± 0.14 spines/μm, n = 142 spines, 7 cells, 3 mice; P < 0.05, two-tailed t test, comparing WT vs. KO and KO vs. KO-T). *: P < Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences.")
52
and the effects of IGF-1 treatment
Changes in synaptic transmission in MeCP2 mutant mice and the effects of IGF-1 treatment Changes in synaptic transmission in MeCP2 mutant mice and the effects of IGF-1 treatment. (A) Representative traces from intracellular recordings of spontaneous excitatory postsynaptic currents (EPSCs) in acute slices from P28–32 sensorimotor cortex. Traces are presented for wild type (WT), mutant (KO), or mutant treated with (1–3)IGF-1 from P13–15 onward (KO-T). (B) Distributions of observed EPSC amplitudes measured across multiple cells, indicating a significant decrease in the size of EPSCs in mutant animals (WT, n = 1543 events, 11 cells; KO, 717 events, 6 cells, P < Kolmogorov-Smirnov test). Treatment with (1–3)IGF-1 partially but significantly reversed this trend (KO-T, n = 1723 events, 7 cells; KO-T vs. KO P < Kolmogorov-Smirnov test). (C) Mean EPSC amplitude, as in (B), for cells in each group. EPSCs are smaller in KO animals but larger with treatment of (1–3)IGF-1 (WT 17.3 ± 2.9 pA, KO 6.8 ± 0.8 pA, KO-T 9.1 ± 0.6 pA; WT vs. KO P < 0.01, KO vs. KO-T P < 0.05, two-tailed t test). **: P < 0.01; *: P < 0.05. Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences
 Representative traces from intracellular recordings of spontaneous excitatory postsynaptic currents (EPSCs) in acute slices from P28–32 sensorimotor cortex. Traces are presented for wild type (WT), mutant (KO), or mutant treated with (1–3)IGF-1 from P13–15 onward (KO-T). (B) Distributions of observed EPSC amplitudes measured across multiple cells, indicating a significant decrease in the size of EPSCs in mutant animals (WT, n = 1543 events, 11 cells; KO, 717 events, 6 cells, P < Kolmogorov-Smirnov test). Treatment with (1–3)IGF-1 partially but significantly reversed this trend (KO-T, n = 1723 events, 7 cells; KO-T vs. KO P < Kolmogorov-Smirnov test). (C) Mean EPSC amplitude, as in (B), for cells in each group. EPSCs are smaller in KO animals but larger with treatment of (1–3)IGF-1 (WT 17.3 ± 2.9 pA, KO 6.8 ± 0.8 pA, KO-T 9.1 ± 0.6 pA; WT vs. KO P < 0.01, KO vs. KO-T P < 0.05, two-tailed t test). **: P < 0.01; *: P < Tropea D. et.al. PNAS 2009;106: ©2009 by National Academy of Sciences.")
53
De Vrii Fet al. Neurobiol Dis 2008
Rescue of behavioral phenotype and neuronal protrusion morphology in Fmr1 KO mice. De Vrii Fet al. Neurobiol Dis 2008 Fig. 1. Rescue of prepulse inhibition of startle in Fmr1 KO mice. Both wild type and Fmr1 KO mice were subjected to prepulse inhibition of startle procedures. Fmr1 KO mice displayed a dramatic impairment of PPI on day 1 (baseline levels). This reduction was rescued to wild type levels on day 2 by injection of 20 mg/kg MPEP 30 min prior to training. Interestingly, the wild types showed an equal improvement of PPI performance after injection of MPEP.
. This reduction was rescued to wild type levels on day 2 by injection of 20 mg/kg MPEP 30 min prior to training. Interestingly, the wild types showed an equal improvement of PPI performance after injection of MPEP.")
Apresentações semelhantes

 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")






. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")
 Dr. Eric J. Topol N. Engl.>")










