Carregar apresentação
1
Metabolismo e eliminação de drogas
Arquivo Metabolismo e eliminação de drogas Dúvidas Site Aula

2
B- Explique a razão da correção mencionada acima
Questão 01 – Valor = 1,0 pontos A- Descreva o gráfico acima (note que o coeficiente de lipossolubilidade foi corrigido pelo peso molecular). B- Explique a razão da correção mencionada acima C- Interprete o gráfico em relação aos medicamentos com quadrados pretos D- Ofereça uma explicação para o resultado obtido com a fenitoína (phenytoin).
. B- Explique a razão da correção mencionada acima. C- Interprete o gráfico em relação aos medicamentos com quadrados pretos. D- Ofereça uma explicação para o resultado obtido com a fenitoína (phenytoin).")
3
Aqueous humour levels after dosing with pilocarpine and fluorometholone in ointment and aqueous solution ● Pilocarpine Solution ○ Pilocarpine ointment ▲Fluorometholone Solution ∆ Fluorometholone Oitment Physicochemical Principles of Pharmacy – Fourth edition – capitulo 9 – fig. 9.36

4
Scanning electron micrographs showing the crystal habit of (a) Form 1 and (b) Form 2 of paracetamol grown from supersaturated IMS a b Physicochemical Principles of Pharmacy – Fourth edition – capitulo 1 – fig. 1.11

5
Comparison of serum levels obtained with suspensions of chloramphenicol palmitate after oral administration of a dose equivalent to 1.5g of chloramphenicol Physicochemical Principles of Pharmacy – Fourth edition – capitulo 1 – fig. 1.13

6
Serum Levels obtained after oral administration of suspension containing 250mg ampicilin as the anhydrate and as the trihydrate Physicochemical Principles of Pharmacy – Fourth edition – capitulo 1 – fig. 1.14

7
Galantamine pharmacokinetics in dogs given intranasal formulation (filled diamonds), oral solution (filled triangles), and oral tablet (filled squares). The data are shown for galantamine measured in (A) plasma; (B) the CSF; and (C) as the ratio of drug measured in CSF to plasma Proteins and Peptides Phamacokinetic, Pharmacodynamic and Metabolic Outcomes – Pag. 176 – Fig. 1

8
Plasma (black) and breast milk (gray) concentrations of bupropion after 100-mg oral doses every 6hr
Milk/plasma Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

9
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig
10
Mean AUC, maximum Plasma Concentration, and Terminal Half-life of Erythropoietin in End-Stage Renal Desease Patients followig Intravenous and Subcutaneous Administration Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 21.15

11
An example of quantitiative whole body autoradiography (QWBA) in rat after administration of C-14-labeled material. The figure shows the distribuition of radioactivity at various time points postdose. The image was generated by taking a sliced section of the whole body of rat and exposing it to a phosphorimaging film Drug Metabolism in drug design and development – Wiley Interscience – Fig 9.2

12
1 – Diminuição da ativade farmacológica
Consequências do Metabolismo de Medicamentos 1 – Diminuição da ativade farmacológica 2 – Aumento da atividade farmacológica 3 – Aumento da toxicidade (carcinogênese, mutagênese, citotoxicidade) 4 – Alteração da atividade farmacológica Foye’s Principles of Medicinal Chemistry – Chapter 8 – pag. 202
 4 – Alteração da atividade farmacológica. Foye’s Principles of Medicinal Chemistry – Chapter 8 – pag")
13
Reação de Biotransformação e Farmacológica do metabólito ativo - I
Exemplo Droga ativa para Metabólito Inativo Anfetamina Fenobarbital Deaminação Hidroxilação Fenilacetona Hidroxifenobarbital Droga ativa para Metabólito Ativo Codeína Procainamida Fenilbutazona Desmetilação Acetilação Hidroxilação Morfina Oxifenilbutazona

14
Reação de Biotransformação e Farmacológica do metabólito ativo - II
Exemplo Droga inativa para Metabólito Ativo Hetacilina Sulfasalazina Hidrólise Azoredução Ampicilina Sulfapiridina+àcido 5 amino salicílico Droga ativa para Intermediário Reativo Acetaminofeno Benzopireno Hidroxilação aromática Intermediário reativo (necrose hepática) Intermediário reativo (carcinogênico)
 Intermediário reativo (carcinogênico)")
15
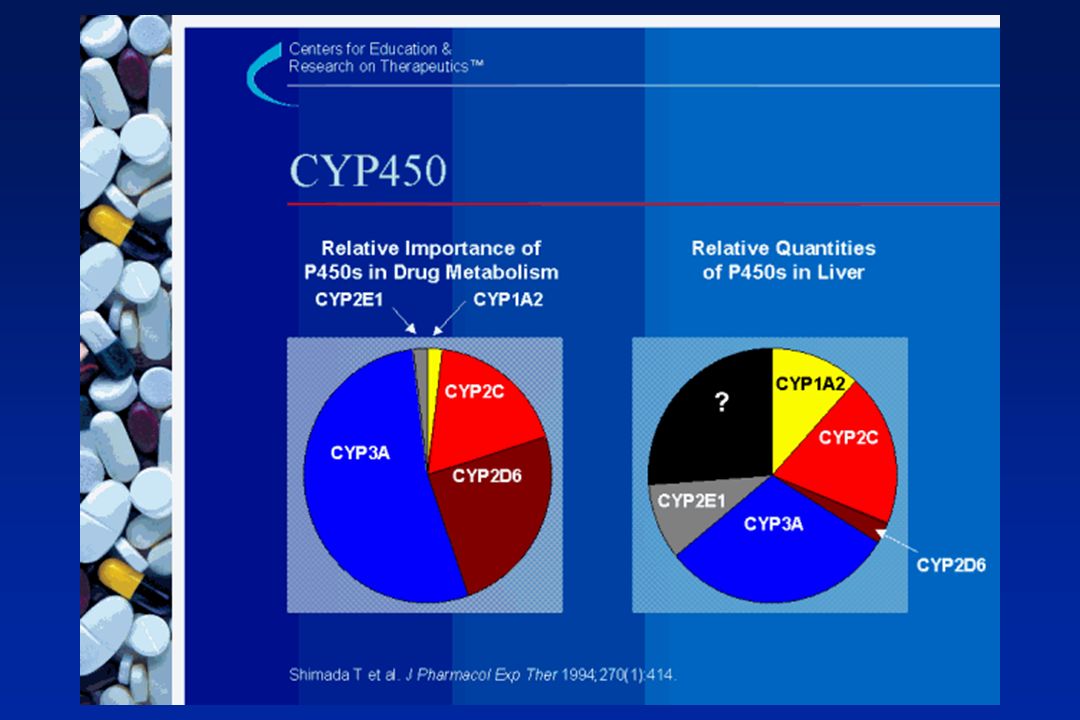
Percent of clinically important drugs metabolized by human CYP450 isoforms

16
Isoformas de citocromo P450
CYP 1A2 CYP3A CYP2C9 CYP2C19 CYP2D6

17
Nomenclatura do citocromo CYP2D6
CYP –citocromo P450 2 - família genética D – subfamília genética 6 – gene específico

19
Polymorphic Distribution
A trait that has differential expression in >1% of the population Number of Subjects PM EM URM Increasing Metabolic Capacity

20
Examples of biotransformation reactions leading to a preferred marketed drug
Drug Metabolism in drug design and development – Wiley Interscience – Fig 1.1

21
Examples of biotransformation reactions leading to a preferred marketed drug
Desloratadine Drug Metabolism in drug design and development – Wiley Interscience – Fig 1.1

22
Examples of biotransformation reactions leading to a preferred marketed drug
Drug Metabolism in drug design and development – Wiley Interscience – Fig 1.1

23
Examples of biotransformation reactions leading to a preferred marketed drug
Drug Metabolism in drug design and development – Wiley Interscience – Fig 1.1

24
(a) Fractions of drug metabolized by various enzyme systems
(a) Fractions of drug that are P450 substrates metabolized by individual P450s Drug Metabolism in drug design and development – Wiley Interscience – Fig 2.1
 Fractions of drug that are P450 substrates metabolized by individual P450s. Drug Metabolism in drug design and development – Wiley Interscience – Fig 2.1.")
25
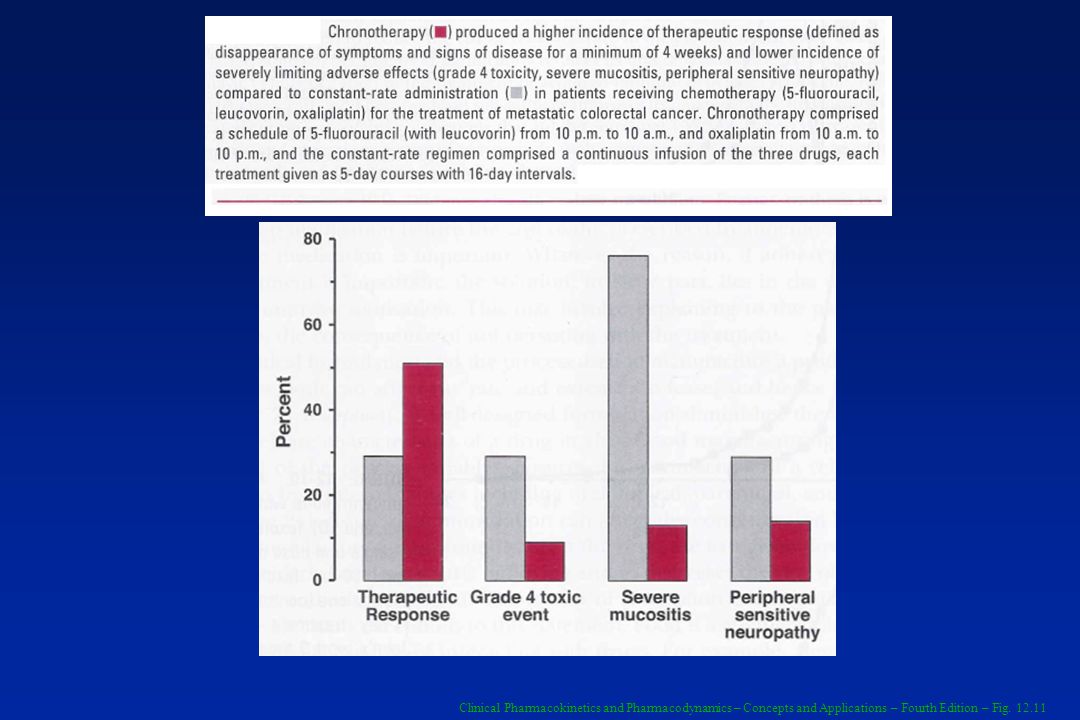
The much smaller intrapair variability in plateau plasma concentration of nortriptyline between nine identical twins than between 12fraternal twins indicates that genetics plays a major role in nortriptyline pharmacokinetics Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 13.1

26
The plateau plasma concentration of nortriptyline varies widely in 263 patients receiving a regime of 25 mg nortriptyline orally 3 times daily Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 12.2

27
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 13.2

28
The daily dose of warfarin required to produced a similar degree of anticoagulation in 200 adult patients varies widely Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 12.1

29
There is considerable interindividual pharmacodynamics variability in response to oral anticoagulant warfarin as demonstrated by the substantial spread in the unbound concentration of the active S-isomer associated with a similar degree of anticoagulation in a group of 97 patients on maintenance tehrapy Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 12.4

30
Genetic plays a significant role in the maintenance dose requirement of warfarin used in the treatment of various cardiovascular diseases Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 13.4

31
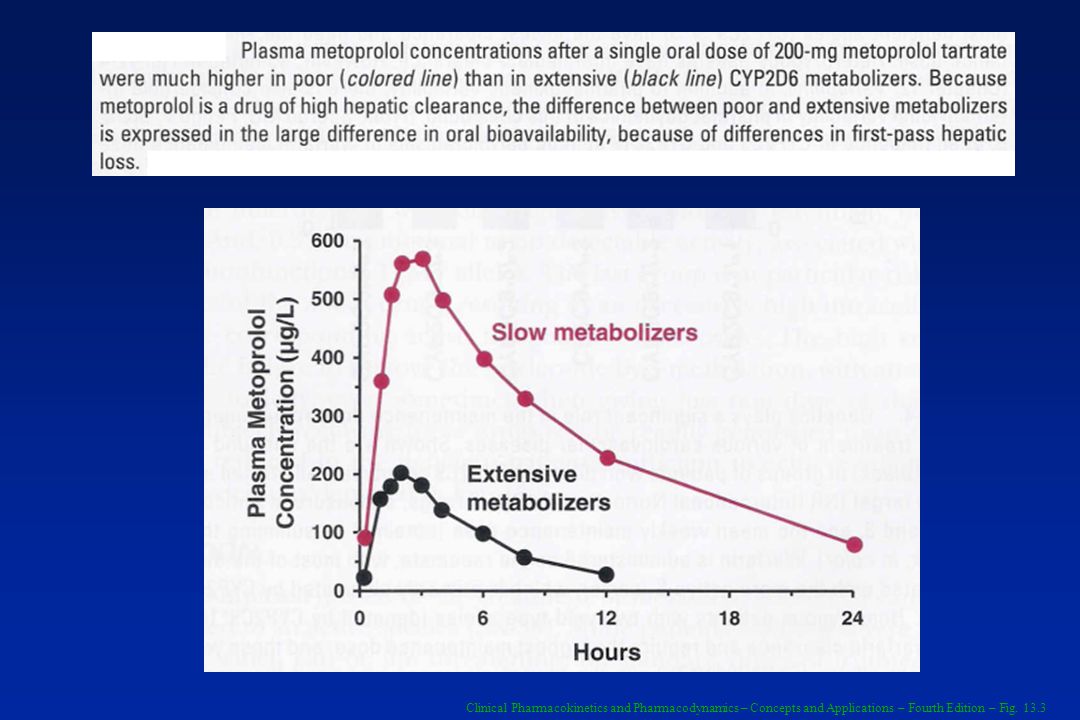
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 13.3
32
The bimodal distribution of the 6-hr plasma isoniazid concentration in 483 subjects after 9.8 mg/kg isoniazid orally results from acetylation polymorphism Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 13.6

33
Displayed semilogatithmically are the plasma concentrations of methylprednisolone (●) and its water-soluble hemisuccinate ester (●) following an i.v. bolus injection of 80 mg of the ester; mean of 11 subjects Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 20.2

34
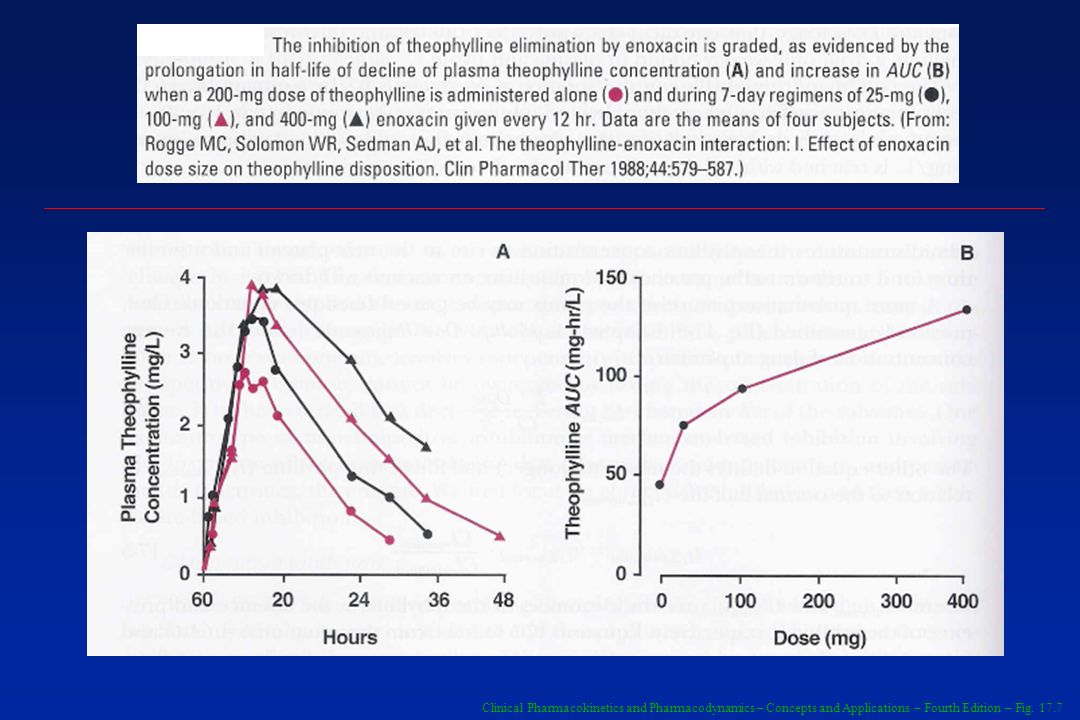
Enoxacin inhibits theophylline elimination
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 17.6

35
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 17.7
36
Citocromo P4503A Responsável pelo metabolismo de:
Maioria dos bloqueadores de canais de cálcio Maioria dos benzodiazepínicos Maioria dos inibidores de protease do HIV Maioria das estatinas Ciclosporina Maioria dos anti-histamínicos não sedativos Presente no TGI e fígado

37
Inibidores de CYP3A Cetoconazole Fluconazole Itraconazole Cimetidina
Claritromicina Eritromicina Suco de toronja

38
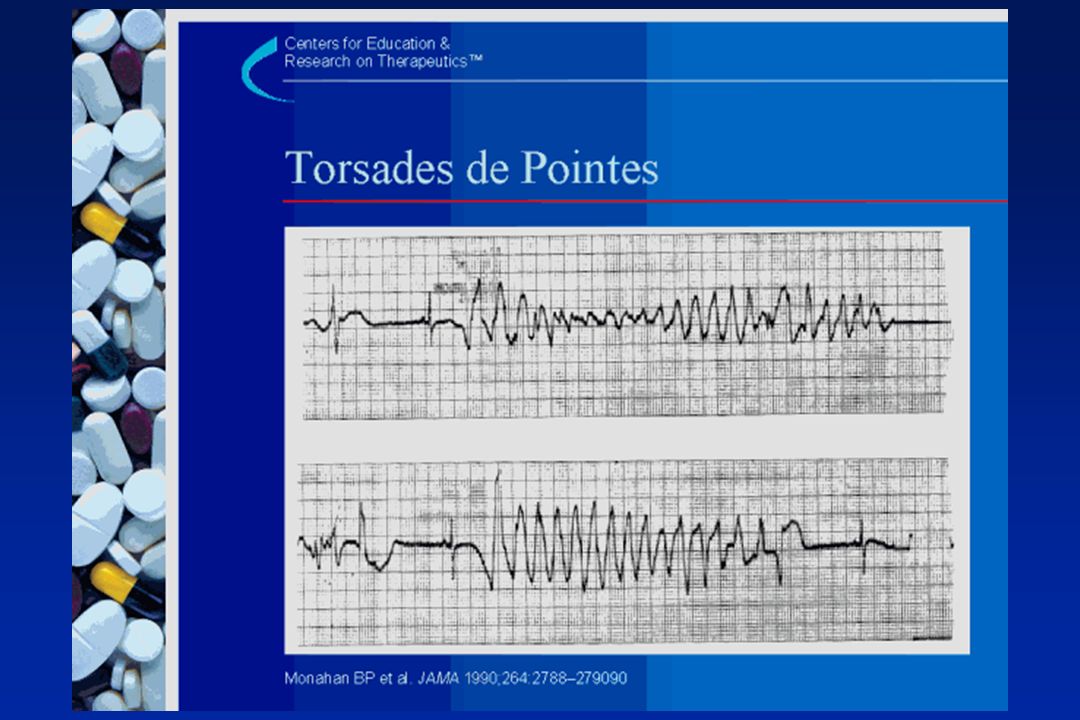
Arritmia ventricular (Torsades de Pointes) devido a associação de medicamentos
Mulher de 39 anos Terfenadina 60mg 2x/dia e cefaclor 250mg 3x/dia Auto-medicação com cetoconazol 200mg 2x/dia para candidíase vaginal Palpitações, síncope, torsades de pointes (QTc 655 msec)
")
40
Indutores de CYP3A Carbamazepina Rifampicina Rifabutina Ritonavir
Hypericum perforatum

41
Efeito de um indutor de metabolismo (Rifampicina 600mg/dia por 3 dias) na administração de warfarina (1.5 mg/kg) 20 Concentração de Warfarina (mg/L) 10 4 Dose única 2 1 40 Tempo de Protrombina (sec) 30 Rifampicina 20 14 Faixa Normal 12 Dias O'Reilly RA. Interaction of sodium warfarin and rifampin. Studies in man. Ann Intern Med Sep;81(3):
 Dose única Tempo de Protrombina (sec) 30. Rifampicina Faixa Normal Dias. O Reilly RA. Interaction of sodium warfarin and rifampin. Studies in man. Ann Intern Med Sep;81(3):")
42
Administration of phenobarbital (60 mg daily) to a patient receiving dicumarol chronically (75 mg daily) reduce, through induction, the plasma concentration of the anticoagulant (●) and prothrombin time (○), a measure of its effect on the concentration of the vitamin Kl-dependent clotting factors. The time course of the events is largely controlled by the kinetics of phenobarbital, half-life 4 days Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

43
Warfarin-phenylbutazone interaction
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

44
Efeito da administração do dissulfiram no metabolismo da clorzoxazona
100 Após dissulfiram (500mg v.o. 10h antes) 10 Concentração de clozoxaona (mg/L) 1 Antes dissulfiram 0.1 Horas Clin. Pharmacol, 1993
 10. Concentração de clozoxaona (mg/L) 1. Antes dissulfiram Horas. Clin. Pharmacol,")
45
Indução causada pelo pentobarbital Concentração de Alprenolol (mg/L)
0.1 Oral antes Concentração de Alprenolol (mg/L) 0.01 Oral depois i.v. antes i.v. depois 0.001 Horas Clin. Pharmacol. Ther., 1977
 Oral depois. i.v. antes. i.v. depois Horas. Clin. Pharmacol. Ther.,")
46
Efeito da cimetidina (400mg 6/6h 4d) na biodisponibilidade do labetolol
AUC CL F 80 60 40 20 -20 Oral I.V. % de alteração N.S. J. Clin. Pharmacol, 1984

47
Impact of Route of Administration of Diltiazem on the Extent of inhibition of Oral Lovastatin
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 17.6

48
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

49
Cilastatin markedly increases the urinary excretion of the antibiotic impenem by inhibiting the dehydropeptidase in the kidney responsible for its metabolism Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

50
Clarithomycin irreversibly inactivates CYP3A, the enzyme responsible for the metabolism of midazolam
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

51
Rifampin, administered intravenously, increases the systemic exposure of orally administered atorvastatin, and shortens its half-life. Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

52
Plasma concentration vs
Plasma concentration vs. time profiles of halofantrine (a) and N-desbutylhalofantrine (b) upon oral administration of a single dose of 500 mg halofantrine hydrochloride alone (■) or together with 50 mg fluconazole (▲) to 15 adult male volunteers. The data are the means ± SD Effect of fluconazole on the pharmacokinetics of halofantrine in healthy volunteers - Journal of Clinical Pharmacy and Therapeutics (2009) 34, 677–682 – Fig 1
 and N-desbutylhalofantrine (b) upon oral administration of a single dose of 500 mg halofantrine hydrochloride alone (■) or together with 50 mg fluconazole (▲) to 15 adult male volunteers. The data are the means ± SD. Effect of fluconazole on the pharmacokinetics of halofantrine in healthy volunteers - Journal of Clinical Pharmacy and Therapeutics (2009) 34, 677–682 – Fig 1.")
53
Mean plasma concentration of desipramine after a 50-mg oral dose given alone (●) and after 8 daily doses (60 mg each) of fluoxetine (●). Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

54
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 20.3

55
Alteração da hidroxilação de enantiômeros da mefenitoína
1200 1000 500 100 50 10 1200 1000 500 100 50 10 R-mefenitoína R- mefenitoína Concentração Plasmática (mg/mL) T ½ = 76h Concentração Plasmática (mg/mL) S- mefenitoína S- mefenitoína T ½ = 2.13h A B Tempo (dias) Tempo (dias)
 T ½ = 76h. Concentração Plasmática (mg/mL) S- mefenitoína. S- mefenitoína. T ½ = 2.13h A. B. Tempo (dias) Tempo (dias)")
56
Subjects received morphine sulfate orally (11
Subjects received morphine sulfate orally (11.7 mg, colored lines) and intravenously (5 mg, black lines) on separate occasions. Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 20.7
 and intravenously (5 mg, black lines) on separate occasions. Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig")
57
Two situation following constant-rate drug infusion are depicted
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 20.8

58
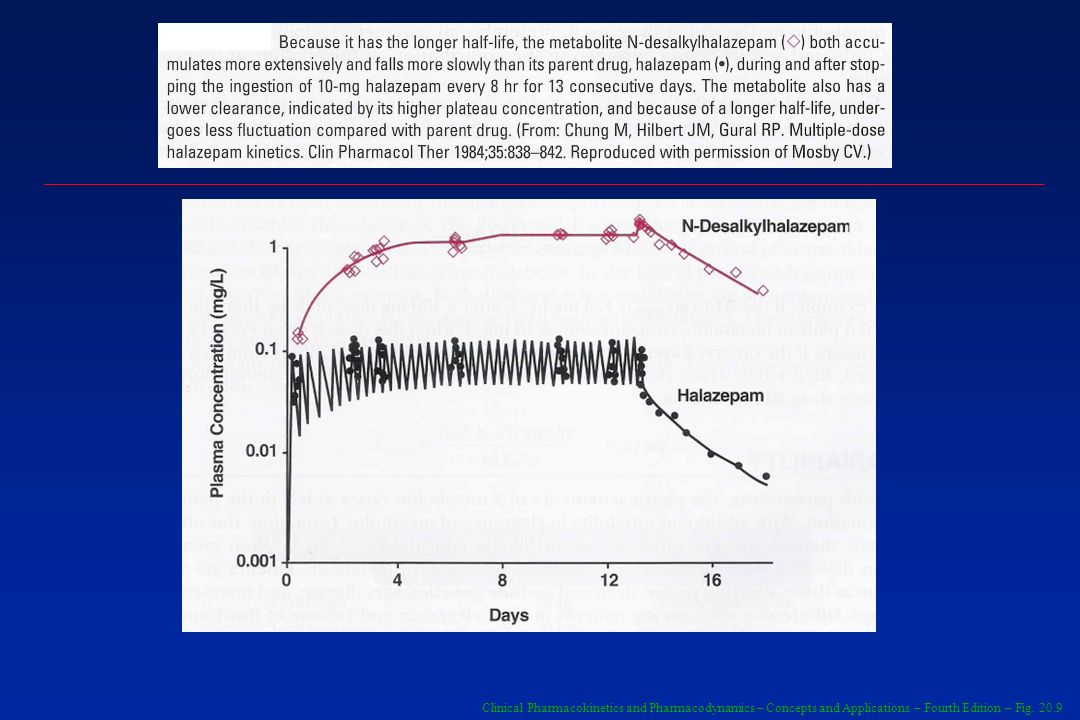
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 20.9
59
Classification of human P450s based on major substrate class
Drug Metabolism in drug design and development – Wiley Interscience – Table 2.1

60
Localization of UGT enzymes in the endoplasmic reticulum.
The active site is located on the inside of the ER with a single transmembrane domain and a 25 a.a. COO- cytosolic tail. UDPGA is transported into the ER and is trans-stimulated by UDPGlcNAC. Once the glucuronides are formed, they must be transported out of the ER by a separate transport protein (depicted by flipping through the membrane) Drug Metabolism in drug design and development – Wiley Interscience – Fig 3.2
 Drug Metabolism in drug design and development – Wiley Interscience – Fig 3.2.")
61
Common SULT substrate. Arrows indicate site of sulfonation for each
Drug Metabolism in drug design and development – Wiley Interscience – Fig 3.6

62
Examples of CYP substrates and inhibitors used in clinical DDI studies
Drug Metabolism in drug design and development – Wiley Interscience – Table 5.4

63
Frequency of Genetic Polymorphisms Producing Slow Metabolism in Some Drug-Metabolizing Enzymes and Representative Substrates Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 13-1

64
Some Genetic Polymorphisms in Pharmacodynamics
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 13-2

65
MEDICAMENTOS QUE SÃO METABOLIZADOS POR ISOFORMAS DO CITOCROMO P450
Clozapina Ciclobenzaprina Imipramina Naproxeno Teofilina Bupropiona Ciclofosfamida Efavirez Metadona Inibidores de Bomba de Próton: Omeprazole Lansoprazole Pantoprazole Rabeprazole Anti-epilépticos: Diazepam Fenitoína Fenobarbital Amitriptilina Clomipramina Ciclofosfamida Progesterona AINEs: Diclofenaco Ibuprofeno Piroxicam Hipoglicemiantes orais: Tolbutamida Glipizida Antagonistas de Angiotensina II: Irbesartan Losartan Celecoxib Fluvastatina Naproxeno Fenitoína Sulfametoxazole Tamoxifeno Tolbutamida Warfarina Betabloqueadores: S-metoprolol Timolol Antidepressivos: Amitriptilina Clomipramina Desipramina Imipramina Paroxetina Antipsicóticos: Haloperidol Risperidona Codeína Dextrometorfano Flecainida Ondansetrona Tamoxifeno Tramadol Venlafaxina Paracetamol Etanol Antibióticos macrolídeos: Claritromicina, eritromicina, Anti-arrítmico: Quinidina Benzodiazepínicos: alprazolam, diazepam, midazolam, triazolam Imunomoduladores: Ciclosporina, Tacrolimus HIV inibidores de protease: indinavir, ritonavir, saquinavir Anti-histamínicos: astemizole, clorfeniramina Bloqueadores de canais de cãlcio: amlodipina, diltiazem, felodipina, nifedipina, nisoldipina, nitrendipina, verapamil Estatinas: atorvastatina, cerivastatina, lovastatina Bisórpma Gleevec, Haloperidol Metadona, Quinina Sildenafil Tamoxifeno Vincristina

66
INIBIDORES DE CITOCROMO P450
1A2 2B6 2C8 2C19 2C9 2D6 2E1 3A4,5,7 Cimetidina Fluoroquinolonas Fluvoxamina Ticlopidina Ticlopidina Gemfibrozila Montelukast Fluoxetina Fluvoxamina Cetoconazol Lansoprazol Omeprazol Ticlopidina Amiodarona Fluconazol Isoniazida Amiodarona Bupropriona Clorfeniramina Cimetidina Clomipramina Fluoxetina Haloperidol Metadona Paroxetina Quinidina Ritonavir Disulfiram Inbidores de Protease: Indinavir Nelfinavir Ritonavir Amiodarone Cimetidina Claritromicina Diltiazem Eritromicina Fluvoxamina Itraconazol Cetoconazol Verapamil

67
INDUTORES DE CITOCROMO P450
1A2 2B6 2C8 2C19 2C9 2D6 2E1 3A4,5,7 Tabaco Fenobarbital Fenitoína Rifampicina Rifampicina Secobarbital N/A Etanol Isoniazida Carbamazepina Fenobarbital Fenitoína Rifabutina Rifampicina Hypericum perfuratum Troglitazona

68
Changes in the activity of CYP3A4 per milligram of protein in the duodenum of pediatric patients as a function of their age Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

69
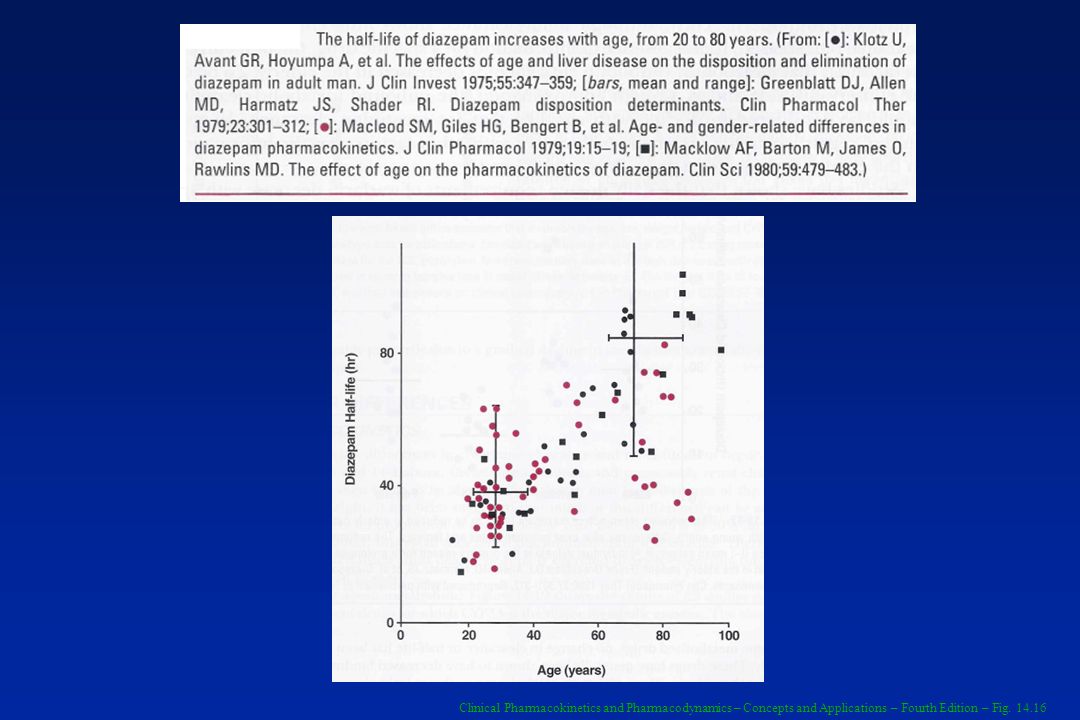
Half-life od diazepam is shortest in the infant and logest in the newborn and the aged
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

70
Creatinine clearances of neonates on Day 1 and Day 6 after birth
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 14.8

71
Creatinine clearance, corrected (colored circles) and uncorrected (open circles) for body surface area, plotted versus conceptional age Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 14.9

72
Mean changes in CYP2D6 (A) and CYP3A4 (B) activity (relative to adult values during the first year after birth, with both in vitro enzyme activity and liver weight taken into account). Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

73
The plateau plasma drug concentrations of two antiepileptic drugs, carvamazepine (A) and valproic acid (B). Are measured after chronic oral medication in children Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

74
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig
75
The minimum alveolar concentration (%) of desflurane required for general anesthesia varies with age
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 14.5

76
Comparison of the Pharmacokinetics of Selected Drugs in Healthy Subjects with that in Patients with Hepatic Cirrhosis Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 15.1

77
Child-Pugh Score for Assessing the Prognosis of Chronic Liver Disease (Mainly Cirrhosis)
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 15.2

78
Relationship between amprenavir AUC and the Child-Pugh score
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 15.2

79
Activities of the conjugating enzymes, glucuronyltransferase, sultransferase, acetyltransferaase, and glutathione transferase in normal (black) and abnormal (colored) human livers vary widely Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 15.3

80
Meia-vida (h) do clordiazepóxido
Normal Cirrose Normal Cirrose 2.2 o 102 56 50 40 30 20 10 1.0 0.8 0.6 0.4 0.2 0.0 Meia-vida (h) do clordiazepóxido Clerance do clordiazepóxico (ml/min/kg) Clin. Pharmacol, 1979
 do clordiazepóxido. Clerance do clordiazepóxico (ml/min/kg) Clin. Pharmacol,")
82
Comparação esquemática entre um capilar cerebral e um capilar periférico (Kandel et al., 2000).
Role of drug efflux transporters in the brain for drug disposition and treatment of brain diseases W. Lo¨scher, H. Potschka / Progress in Neurobiology 76 (2005) 22–76
 22–76.")
83
Características da Barreira Hemato-Encefálica
Targeted nanoparticles for drug delivery through the blood–brain barrier for Alzheimer’s disease C. Roney et al. / Journal of Controlled Release 108 (2005) 193–214
 193–214.")
84
Localização esquemática das proteínas responsáveis por efluxo de medicamentos nas células endoteliais dos capilares cerebrais responsáveis pela barreira hemato-encefálica Role of drug efflux transporters in the brain for drug disposition and treatment of brain diseases W. Lo¨scher, H. Potschka / Progress in Neurobiology 76 (2005) 22–76
 22–76.")
85
Mecanismos de Transporte na Barreira Hemato-Encefálica
Targeted nanoparticles for drug delivery through the blood–brain barrier for Alzheimer’s disease C. Roney et al. / Journal of Controlled Release 108 (2005) 193–214
 193–214.")
86
mdr 1a/1b genetic double knockout
Concentrations (nCig) of [14C]-Amprenavir in CD-1 Mice Pretreated with GF and in FVB mdr la/lb Double Knockout Mice GF chemical knockout mdr 1a/1b genetic double knockout Tissue Vehicle GF Ratio (+/+) (-/-) Ratio Blood 46.3 ± ± ± ± Brain 3.33 ± 0.6a ± ± ± CSF 23.3 ± ± ± NV ND Testes 15.2 ± ± ± ± Muscle 33.0 ± ± ± ± Note: Data are the average from 3-4 animals ± the standard deviation. NV = Not visible. ND = not determined. Limit of Quantitation (LOQ): nCi/g. “Sections had > 40% of pixels below quantification limit (BQL). Pharmaceutical Research, Vol. 16 No 8,1999
 of [14C]-Amprenavir in CD-1 Mice Pretreated with GF and in FVB mdr la/lb Double Knockout Mice. GF chemical knockout. mdr 1a/1b genetic double knockout. Tissue Vehicle GF Ratio (+/+) (-/-) Ratio. Blood 46.3 ± ± ± ± Brain 3.33 ± 0.6a 43.8 ± ± ± CSF 23.3 ± ± ± 6.8 NV ND. Testes 15.2 ± ± ± ± Muscle 33.0 ± ± ± ± Note: Data are the average from 3-4 animals ± the standard deviation. NV = Not visible. ND = not determined. Limit of Quantitation (LOQ): nCi/g. Sections had > 40% of pixels below quantification limit (BQL). Pharmaceutical Research, Vol. 16 No 8,1999.")
87
The effect of elacridar (GF120918) on the oral bioavailability of topotecan.
Use of P-glycoprotein and BCRP inhibitors to improve oral bioavailability and CNS penetration of anticancer drugs TRENDS in Pharmacological Sciences Vol.27 No.1 January 2006

88
Opioid receptor subtype
Initial brain uptake clearances (Clup, mL·100g-1 ·min-1)of opioids during in situ perfusion in mice Compound Opioid receptor subtype Wild-type mice P-gp deficient mice P-gp effect Meperidine µ 185 ± ± ± 0.27 Fentanyl µ 184 ± ± 9* ± 0.27 Morphine µ ± ± 0.08** 1.24 ± 0.08 U κ ± ± 8.8a ± 0.25 Bremazocine κ ± ± 3.8*** 1.50 ± 0.21 Deltophin II δ ± ± ** 1.58 ± 0.36 Methadone µ ± ± 17*** 2.61 ± 0.55 Naltrindole δ ± ± 5.1a ± 0.93 SNC δ ± ± 15a ± 1.26 Loperamide µ ± ± 6*** 10.4 ±1.9 DPDPE δ ± ± *** 11.6 ± 6.4 C. Dagenais et al. / Biochemical Pharmacology 67 (2004) 269–276 – table 1 P-gp effect is defined as the ratio between Clup in mdr1a(/) P-gp deficient and wild-type mice. Data are presented as mean SD of four individual experiments at a single time point or from multiple time point experiments (N ¼ 4 per point at three time points) *P < 0:05; **P < 0:01; ***P < 0:001. aStatistical significance of differences in Vbrain between mdr1a(/) P-gp deficient and wild-type mice at individual time points is reported in Fig. 1.
of opioids during in situ perfusion in mice. Compound. Opioid receptor subtype. Wild-type mice. P-gp deficient mice. P-gp effect. Meperidine µ 185 ± ± ± Fentanyl µ 184 ± ± 9* 1.24 ± Morphine µ 1.04 ± ± 0.08** 1.24 ± U κ 39.2 ± ± 8.8a 1.34 ± Bremazocine κ 44.1 ± ± 3.8*** 1.50 ± Deltophin II δ ± ± ** 1.58 ± Methadone µ 41.7 ± ± 17*** 2.61 ± Naltrindole δ 12.5 ± ± 5.1a 4.44 ± SNC 121 δ 17.0 ± ± 15a 8.60 ± Loperamide µ 9.86 ± ± 6*** 10.4 ±1.9. DPDPE δ ± ± *** 11.6 ± 6.4. C. Dagenais et al. / Biochemical Pharmacology 67 (2004) 269–276 – table 1. P-gp effect is defined as the ratio between Clup in mdr1a(/) P-gp deficient and wild-type mice. Data are presented as mean SD of four individual experiments at a single time point or from multiple time point experiments (N ¼ 4 per point at three time points) *P < 0:05; **P < 0:01; ***P < 0:001. aStatistical significance of differences in Vbrain between mdr1a(/) P-gp deficient and wild-type mice at individual time points is reported in Fig. 1.")
89
Substratos para Glicoproteína P
Amiodarona Clorpromazina Claritromicina Ciclosporina Daunorubicina Dexametasona Digoxina Diltiazem Eritromicina Estradiol Etoposide Felodipina Fexofenadina Flufenazina Hidrocortisona Itraconazol Cetoconazol Lidocaína Loperamide Lovastatina Mifepristona Nelfinavir Nicardipina Nifedipina Ondansetron Paclitaxel Progesterona Prometazina Quinidina Reserpina Ritonavir Saquinavir Sirolimus Tacrolimus Tamoxifen Taniposide Testosterona Trifluoperazina Verapamil Vinblastina Vincristina

90
Indutores e Inibidores de Glicoproteína P
Rifampicina Ritonavir Hypericum perforatum Iohimbina Amiodarona Atorvastatina Clorpromazina Claritromicina Ciclosporina Diltiazem Eritromicina Felodipina Flufenazina Hidrocortisona Indinavir Itraconazol Cetoconazol Lidocaína Mifepristona Nelfinavir Nicardipina Nifedipina Progesterona Propranolol Quinidina Reserpina Ritonavir Saquinavir Tacrolimus Tamoxifeno Testosterona Trifluoperazina Verapamil

91
Efeito do suco de toronja na farmacocinética e farmacodinâmica da Felodipina
Estudo em dose única 150 140 130 120 110 24 20 16 12 8 4 Suco de Toronja Água Concentração Felodipina (nmol/L) Pressão Arterial Sentado (min Hg) 80 70 60 Horas após a Dose Horas após a Dose
 Pressão Arterial Sentado (min Hg) Horas após a Dose. Horas após a Dose.")
92
Efeito do Hypericum perforatum na farmacocinética do Indinavir
14 12 10 8 6 4 2 Administrado após Hypericum perforatum Concentração do Indinavir (μg/mL) Hora (h)
 Hora (h)")
93
A. Mean plasma concentrations with time of midazolam and (B) fexofenadine following a single oral dose of 4-mg midazolam and 180-mg fexofenadine, respectively, alone (control, black) and after 11-day treatment with 300-mg St. John’s wort 3 times daily (colored) Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

94
Cyclosporine inhibits the elimination of rosuvastatin, a drug primarily excreted unchanged in bile and urine Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

95
Plasma concentrations (mean ± SD) of felodipine after an oral dose during steady-state treatment with 5mg twice daily in healthy subjects (n = 12) and elderly hypertensive patients (n = 11) 15 10 5 Concetration (nmol/mL) Elderly Healthy Time (hours) Applied – Biopharmaceutics & Pharmacokinetics – fig. 20.2
 Elderly. Healthy Time (hours) Applied – Biopharmaceutics & Pharmacokinetics – fig")
96
Felodipina (5mg) via oral
Idade Palpitação 3/11 1/12 Rubor 9/11 1/12 Clearance mL/h 619 mL/h

98
Plasma concentration, normalized to dose, as a function of time following the oral administration of two tablets (●) and four tablets (●) of ultramicronized grinseofulvin (125 mg/tablet). Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig. 16.4

99
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig
100
Concentração Plasmática Salicilamida
Concentração plasmática de salicilamida após várias administração por via oral em distintas doses 30 20 10 2.5 Concentração Plasmática Salicilamida (mg/L) 2.0 1.0 0.5 Minutos
 Minutos.")
101
Typical Pharmacokinetics Parameters of Digoxin in the Absence and Presence of Quinidine
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 17.7

102
Saturable First-Pass Metabolism of Nicardipine Observed at Steady State Following oral Doses of 10 to 40 mg Every 8Hr Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Table 16.2

103
???????????????????????????????? Applied Clinical Pharmacokinetics – Larry Bauer – Eq; pag 19

105
Relationship between creatinine creatinine clearance and aminoglycoside elimination rate constant (ke) to estimate initial aminoglycoside elimination when no drug concentrations are available. The y-axis intercept (0.014h-1) is nonrenal elimination for aminoglycosides Applied Clinical Pharmacokinetics – Larry Bauer – Fig. 3-4

106
Relationship between creatinine clearance and digoxin clearance to estimate initial digoxin clearance when no drug concentrations are available Applied Clinical Pharmacokinetics – Larry Bauer – Fig. 3-3

107
Relação entre os valores de CL/F da fenitoína e idade em pacientes controles
25 20 15 10 5 CL/F (ml h-1 kg-1) Idade (anos) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 32.3 – 0.25 x age (r = -0.28, P < 0.05) for elderly patients and CL/F = 1.39 – 0.02 x age (r = -0.05, NS) for controls. For results of analysis on comedication subgroups, see Section 3.3. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)
 Idade (anos) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 32.3 – 0.25 x age (r = -0.28, P < 0.05) for elderly patients and CL/F = 1.39 – 0.02 x age (r = -0.05, NS) for controls. For results of analysis on comedication subgroups, see Section 3.3. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)")
108
Relação entre os valores de CL/F da fenitoína e idade em pacientes controles
25 20 15 10 5 Controles CL/F (ml h-1 kg-1) Dose (mg kg-1 day-1) ( )patients on phenytoin monotherapy and ( ) patients comedicates with phenobarbital. The equations of the lines were CL/F = 15.0 – 0.09 x dose (r = -0.02, NS) for elderly patients and CL/F = x dose (r = -0.04, NS) for controls Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)
 Dose (mg kg-1 day-1) ( )patients on phenytoin monotherapy and ( ) patients comedicates with phenobarbital. The equations of the lines were CL/F = 15.0 – 0.09 x dose (r = -0.02, NS) for elderly patients and CL/F = x dose (r = -0.04, NS) for controls. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)")
109
Relação entre os valores de CL/F da fenitoína e idade em pacientes idosos
25 20 15 10 5 CL/F (ml h-1 kg-1) Idade (anos) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 32.3 – 0.25 x age (r = -0.28, P < 0.05) for elderly patients and CL/F = 1.39 – 0.02 x age (r = -0.05, NS) for controls. For results of analysis on comedication subgroups, see Section 3.3. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)
 Idade (anos) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 32.3 – 0.25 x age (r = -0.28, P < 0.05) for elderly patients and CL/F = 1.39 – 0.02 x age (r = -0.05, NS) for controls. For results of analysis on comedication subgroups, see Section 3.3. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)")
110
Relação entre os valores de CL/F da fenitoína e dose em pacientes idosos
25 20 15 10 5 CL/F (ml h-1 kg-1) Dose (mg kg-1 day-1) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 15.0 – 0.09 x dose (r = -0.02, NS) for elderly patients and CL/F = x dose (r = -0.04, NS) for controls Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)
 Dose (mg kg-1 day-1) ( ) pacientes em monoterapia e ( ) pacientes com terapia adicional de fenobarbital. The equations of the lines were CL/F = 15.0 – 0.09 x dose (r = -0.02, NS) for elderly patients and CL/F = x dose (r = -0.04, NS) for controls. Influence of aging on serum phenytoin concentrations: a pharmacokinetic analysis based on therapeutic drug monitoring data – Epilepsy Research 59 (2004)")
111
Concentration-time plot for gentamicin 120 mg given as a ½-hour infusion (squares with solid line) and as a 1-hour infusion (circles with dashed line) Applied Clinical Pharmacokinetics – Larry Bauer – Fig. 4.1

112
Schematic representation of a hemodialysis system in which drug is passively transferred across a semipermeable mambrane (---) from blood to dialysate Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

113
Concentration-time graph for tombramycin in a hemodialysis patients using estimated population pharmacokinetics parameters Applied Clinical Pharmacokinetics – Larry Bauer – Fig. 3-14

114
Fenobarbital em paciente renal terminal de 70kg Vu= 77L Clu = -
Fenobarbital em paciente renal terminal de 70kg Vu= 77L Clu = -.4 L/h k= 0.005/hr t1/2 = 137 h

115
Plasma dialysis clearance and unbound dialysis clearance with an adjustment for molecular size for 27 different drugs show considerable variability Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

116
Displayed is the fraction of drug in the body at the start of dialysis that is eliminated by 3 hr of dialysis treatment a function of unbound clearance (nodialysis elimination) and unbound volume of distribution Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

117
Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig
118
Relationship between systemic bioavailability (mean ± SD of five patients) and dwell time when teicoplanin is administered intraperioneally Clinical Pharmacokinetics and Pharmacodynamics – Concepts and Applications – Fourth Edition – Fig

119
a . Proponha um esquema terapêutico para o paciente. b . Justifique.
The first step in the conversion of the retroviral agent abacavir (ABC) to its active metabolite, carbovir triphosphate, is phosphorylation to ABC monophosphate by adenosine phosphotransferase. a . Proponha um esquema terapêutico para o paciente. b . Justifique. Prova Medicina Unicamp 2010 – Turma A
 to its active metabolite, carbovir triphosphate, is phosphorylation to ABC monophosphate by adenosine phosphotransferase. a . Proponha um esquema terapêutico para o paciente. b . Justifique. Prova Medicina Unicamp 2010 – Turma A.")
120
Amiodarone is an antiarrhythmic with predominantly class III (Vaughan ± William's classification) effects [1]. The major metabolite of amiodarone, N-desethylamiodarone (N-DEA), has been identified in humans as a consequence of hepatic and possibly intestinal mucosa N-dealkylation [2±4]. a. Descreva os gráficos utilizando parâmetros farmacocinéticos. b. Proponha uma explicação para o resultado observado. c. Proponha uma investigação para confirmar sua hipótese . d. Estime as potenciais consequências farmacodinâmicas, justificando-as em função de conceitos farmacocinéticos. Prova Medicina Unicamp 2010 – Turma A
![Amiodarone is an antiarrhythmic with predominantly class III (Vaughan ± William s classification) effects [1]. The major metabolite of amiodarone, N-desethylamiodarone (N-DEA), has been identified in humans as a consequence of hepatic and possibly intestinal mucosa N-dealkylation [2±4].](http://slideplayer.com.br/slide/81665/1/images/120/Amiodarone+is+an+antiarrhythmic+with+predominantly+class+III+%28Vaughan+%C2%B1+William+s+classification%29+effects+%5B1%5D.+The+major+metabolite+of+amiodarone%2C+N-desethylamiodarone+%28N-DEA%29%2C+has+been+identified+in+humans+as+a+consequence+of+hepatic+and+possibly+intestinal+mucosa+N-dealkylation+%5B2%C2%B14%5D..jpg "a. Descreva os gráficos utilizando parâmetros farmacocinéticos. b. Proponha uma explicação para o resultado observado. c. Proponha uma investigação para confirmar sua hipótese . d. Estime as potenciais consequências farmacodinâmicas, justificando-as em função de conceitos farmacocinéticos. Prova Medicina Unicamp 2010 – Turma A.")
121
However, dramatic reduction in half-life during dialysis does not guarantee that the procedure effectively removes drug during a single-sialysis treatment. Take, for example, phenobarbital in a 70-kg end-stage renal disease patient whose pharmacokinetic parameters are Vu = 77 L, Clu = 0.4 L/hr, k = hr-1, and t1/2 = 137 hr. Using a value of 150 mL/min (9 L/hr) for unbound dialysis clearance the half-life of phenobarbital is reduced to 5.7 hr during dialysis.
 for unbound dialysis clearance the half-life of phenobarbital is reduced to 5.7 hr during dialysis..")





 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")










. Nenhuns direitos reservados, excepto para fins comerciais. Por favor, não coloque.>")






