Carregar apresentação
A apresentação está carregando. Por favor, espere

1
FIBROSE PULMONAR IDIOPATICA ASPECTOS ANATOMOPATOLOGICOS
Dra Larissa Cardoso Marinho Unidade de Anatomia Patologica HUB- UnB

2
PNEUMONIA INTERSTICIAL USUAL
DIAGNOSTICO – PROCESSO DINAMICO CLINICO X RADIOLOGICO X ANATOMOPATOLOGICO PATOLOGISTA : HISTORIA RELEVANTE APRESENTAÇÃO CLINICA RADIOLOGIA

4
PNEUMONIA INTERSTICIAL USUAL
BIOPSIA PULMONAR FORMOL A 10% FRASCO IDENTIFICADO INCLUINDO A LOCALIZAÇÃO PULMONAR DA BIOPSIA EX : LOBO DIREITO/ LINGULA Tamanho ideal adulto : min 2 cm/ geral 7-8 cm ESTUDO MICROBIOLOGICO – FRASCO SECO ESTERIL MATERIAL PARA MICROSCOPIA ELETRONICA – GLUTARALDEIDO MATERIAL PARA ESTUDO GENETICO – CONGELADO OU RNAlater One mm pieces of tissue are taken from different areas and fixed in glutaraldehyde for ultrastructural investigation. Additional tissue should be snap frozen or placed in RNAlater to facilitate additional genetic testing, if possible. Ideally pathologist or other experienced person: gently inflates the remaining tissue with formalin via a small bore needle, taking care not to over-expand the tissue as this can cause artefact that mimics lymphangiectasia, or wash out alveolar contents such as macrophages Otherwise and in most cases, the tissue goes straight into formalin. The specimen will normally be a wedge of subpleural lung, stapled along the surgical margin. A description includes its dimensions and any parenchymal or pleural abnormalities. The row of staples is cut off (unless already used). The axis of slicing will depend on the volume of tissue, but ideally aim for sections with the largest possible area.
. The axis of slicing will depend on the volume of tissue, but ideally aim for sections with the largest possible area.")
7
PNEUMONIA INTERSTICIAL USUAL
BIOPSIA TRANSBRONQUICA: EXCLUSAO NEOPLASIA, SARCOIDOSE, PROCESSOS INFECCIOSOS Sensibilidade e a especificidade para UIP ? /quantidade e locais desconhecidos TORACOSCOPIA VIDEO ASSISTIDA/ BIOPSIAS ABERTAS IDEAL BIOPSIAS CIRURGICAS EM MAIS DE UM LOBO Evitar –Fibrose severa com padrão honeycomb - INESPECIFICO . Clampeamento REVISOES DE LAMINA: NOVOS DADOS CLINICOS , IDENTIFICAÇÃO DE UMA POSSIVEL CAUSA DA FIBROSE RESPOSTA AO TRATAMENTO. TRANSBRONQUICA:The role of transbronchial biopsies in the diagnosis of the IIPs in most cases is to exclude sarcoidosis, neoplasms, and certain infections. In some cases with classic clinical and radiologic features of COP (50, 51) or AIP the histologic diagnosis of an OP or DAD pattern, respectively, may be viewed as confirmatory on a bronchoscopic biopsy specimen ( See below). lung biopsies from more than one lobe of the lung: severe fibrosis with honeycombing the biopsy specimen should not be taken from the worst-looking areas because these frequently show nonspecific changes Ideally the lung biopsy should include the full spectrum of the gross appearance,including honeycomb foci, because these confirm severe fibrosis, one of the criteria for UIP In cases requiring histopathology, the specificity and positive predictive value of UIP pattern identified by transbronchial biopsy has not been rigorously studied. While transbronchial biopsy specimens may show all the histologic features of UIP (123), the sensitivity and specificity of this approach for the diagnosis for UIP pattern is unknown. It is also unknown how many and from where transbronchial biopsies should be obtained. Question: Should transbronchial lung biopsy be used in the evaluation of suspected IPF? Transbronchial lung biopsy is useful in the evaluation of selected conditions (e.g., granulomatous disorders such as sarcoidosis). A UIP pattern on HRCT makes these conditions unlikely (104, 105, 109). In cases requiring biopsies should be obtained The surgeon must also attempt to avoid deflation of the specimen through clamping, as this complicates interpretation of histological findings. In a small proportion of cases the pathologic diagnosis may need to be revised in the light of an unexpected clinical course, identification of a potential cause for lung fibrosis, or response to treatment. Periodic review should include re-examination of the original lung biopsy and radiologic material in addition to the data from the clinical follow-up.
 or AIP the histologic diagnosis of an. OP or DAD pattern, respectively, may be viewed as confirmatory on a bronchoscopic biopsy specimen ( See below). lung biopsies from more than one lobe of the lung: severe fibrosis with honeycombing the biopsy specimen. should not be taken from the worst-looking areas because. these frequently show nonspecific changes. Ideally the lung biopsy should include the full spectrum of the gross appearance,including honeycomb foci, because these confirm severe fibrosis, one of the criteria for UIP. In cases requiring. histopathology, the specificity and positive predictive. value of UIP pattern identified by transbronchial biopsy. has not been rigorously studied. While transbronchial. biopsy specimens may show all the histologic features of. UIP (123), the sensitivity and specificity of this approach. for the diagnosis for UIP pattern is unknown. It is also. unknown how many and from where transbronchial. biopsies should be obtained. Question: Should transbronchial lung biopsy be used in the. evaluation of suspected IPF Transbronchial lung biopsy is useful in the evaluation of. selected conditions (e.g., granulomatous disorders such as. sarcoidosis). A UIP pattern on HRCT makes these. conditions unlikely (104, 105, 109). In cases requiring. biopsies should be obtained. The surgeon must also attempt to avoid deflation of the specimen through clamping, as this complicates interpretation of histological findings. In a small proportion of cases the pathologic diagnosis may. need to be revised in the light of an unexpected clinical. course, identification of a potential cause for lung fibrosis, or response to treatment. Periodic review should include. re-examination of the original lung biopsy and radiologic. material in addition to the data from the clinical follow-up.")
8
PNEUMONIA INTERSTICIAL USUAL
PROBLEMAS INTERPRETAÇÃO Informação clinica inadequada. Dados radiológicos inadequados. Biopsias inadequadas ( pequenas /não representativa ) Terapia previa – alterações na radiologia e histologia Achados histologicos diferentes nos lobos.
 Terapia previa – alterações na radiologia e histologia. Achados histologicos diferentes nos lobos.")
9
PNEUMONIA INTERSTICIAL USUAL
ASPECTOS HISTOLOGICOS PULMÃO HABITUAL X PULMÃO UIP

13
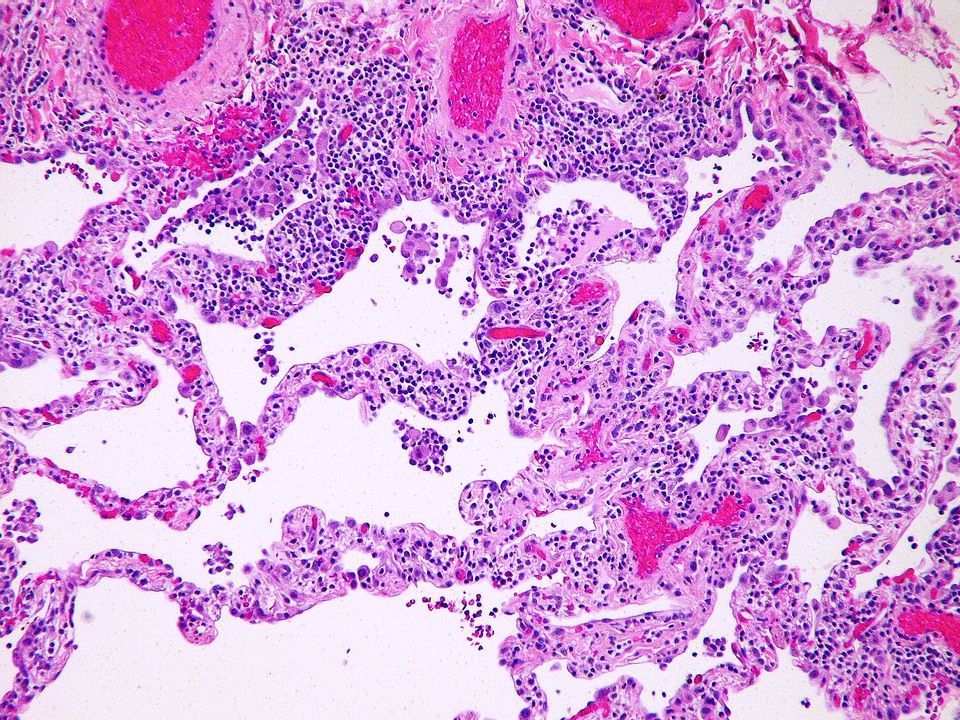
Bronchiole with surrounding alveoli.

14
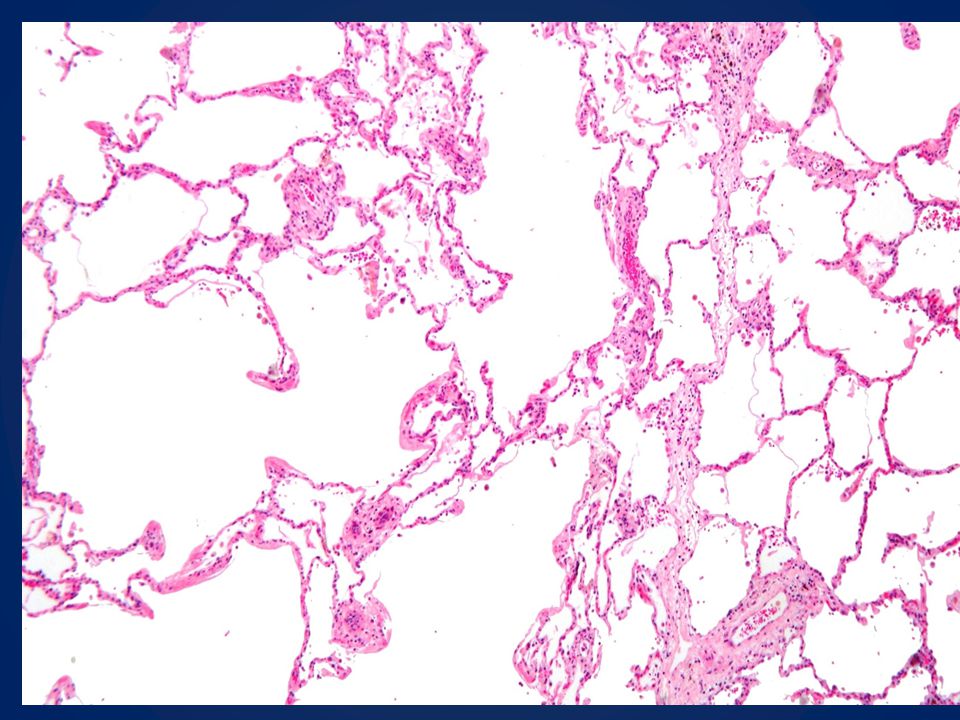
PNEUMONIA INTERSTICIAL USUAL
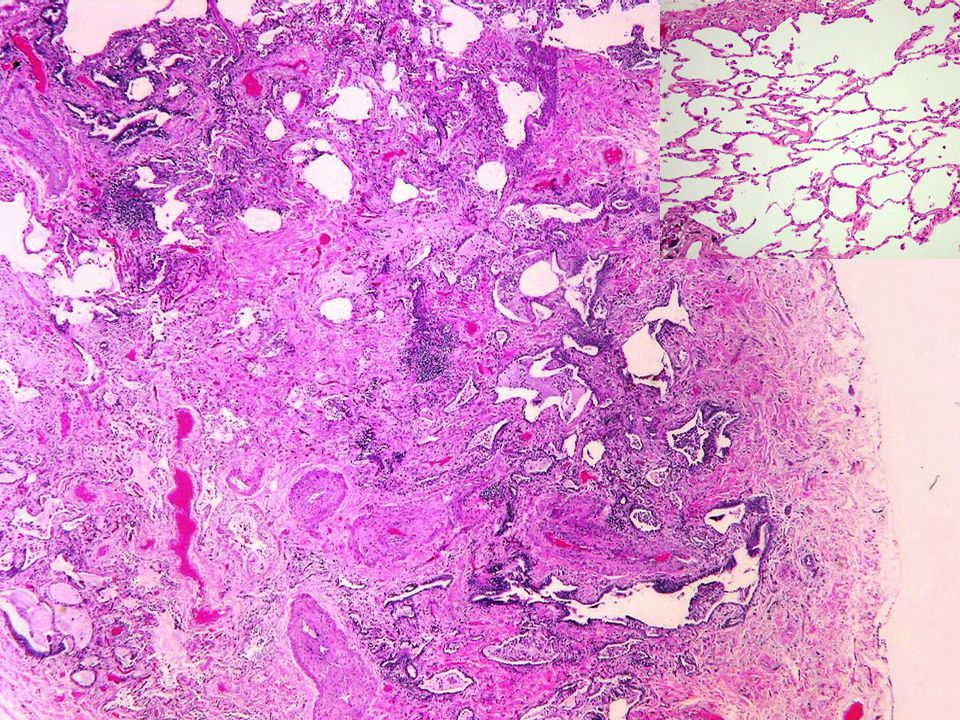
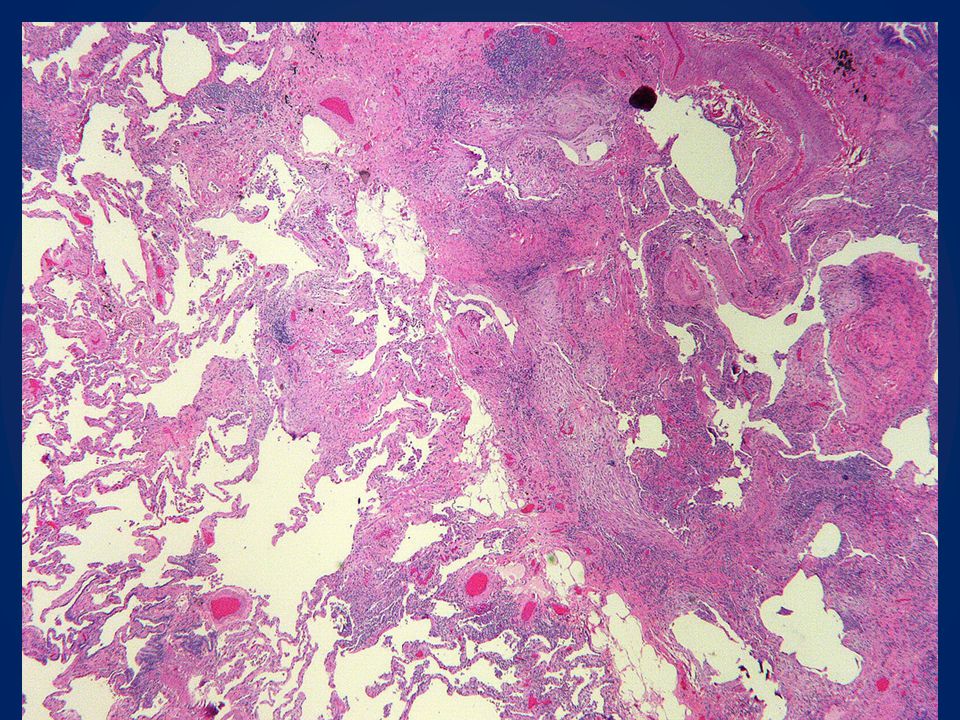
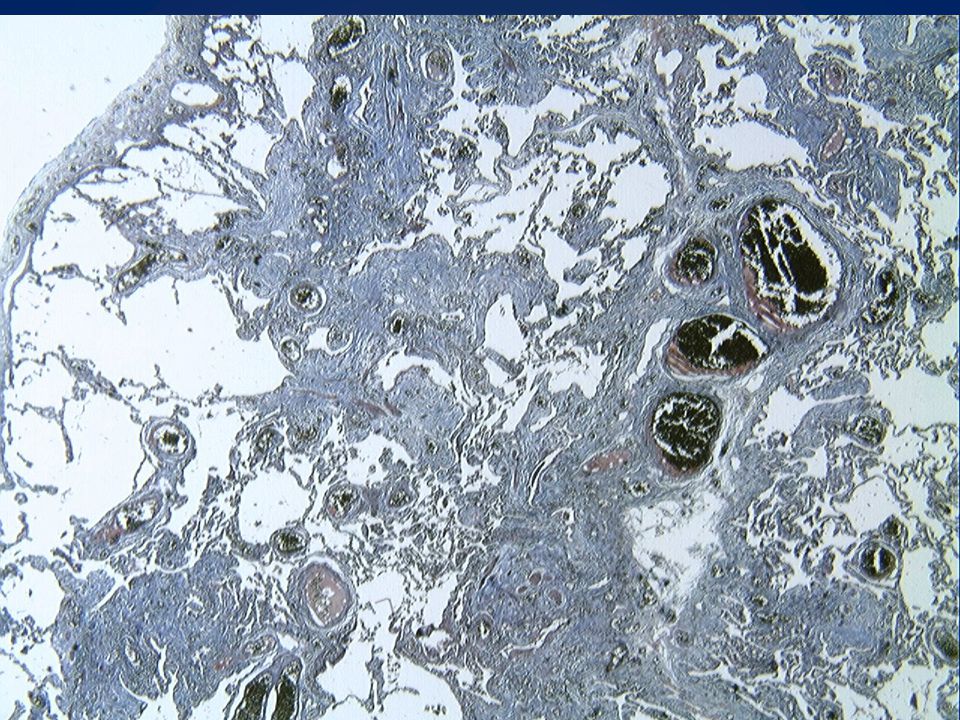
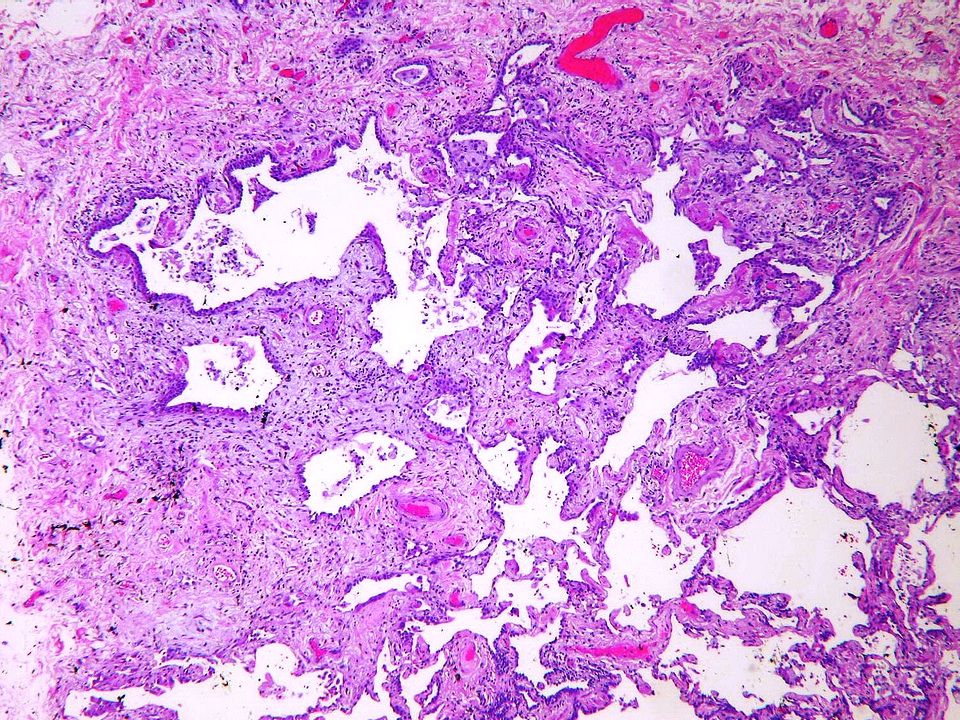
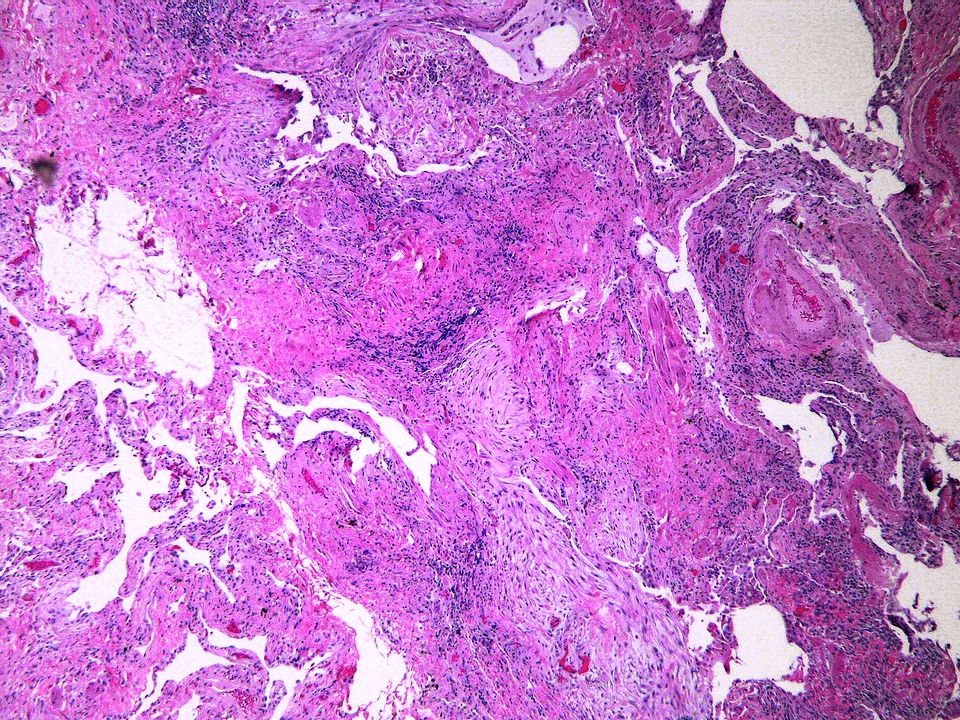
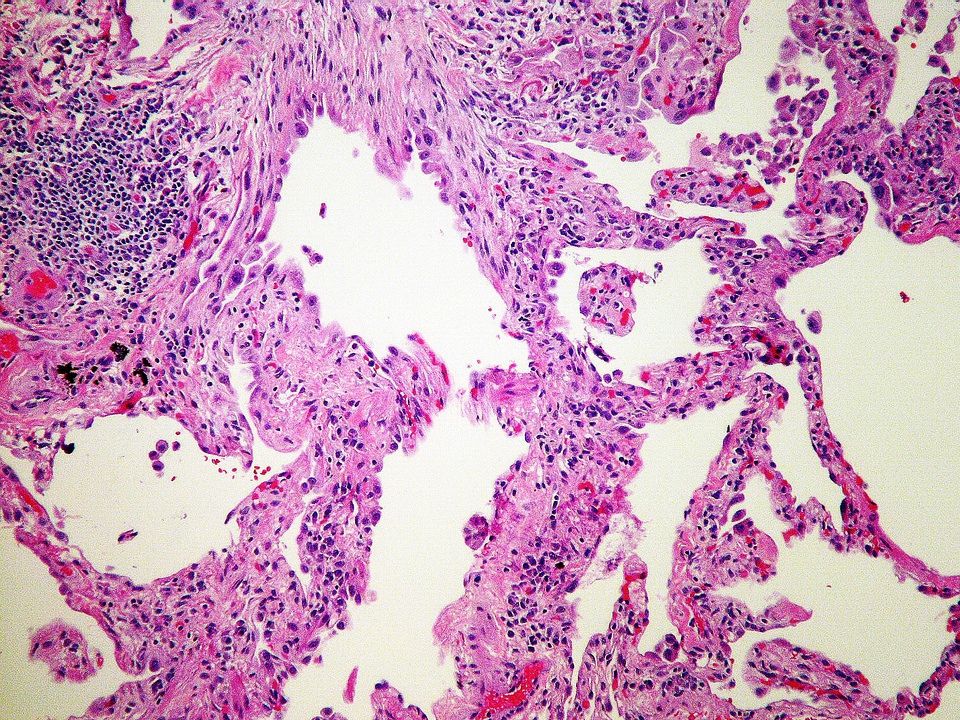
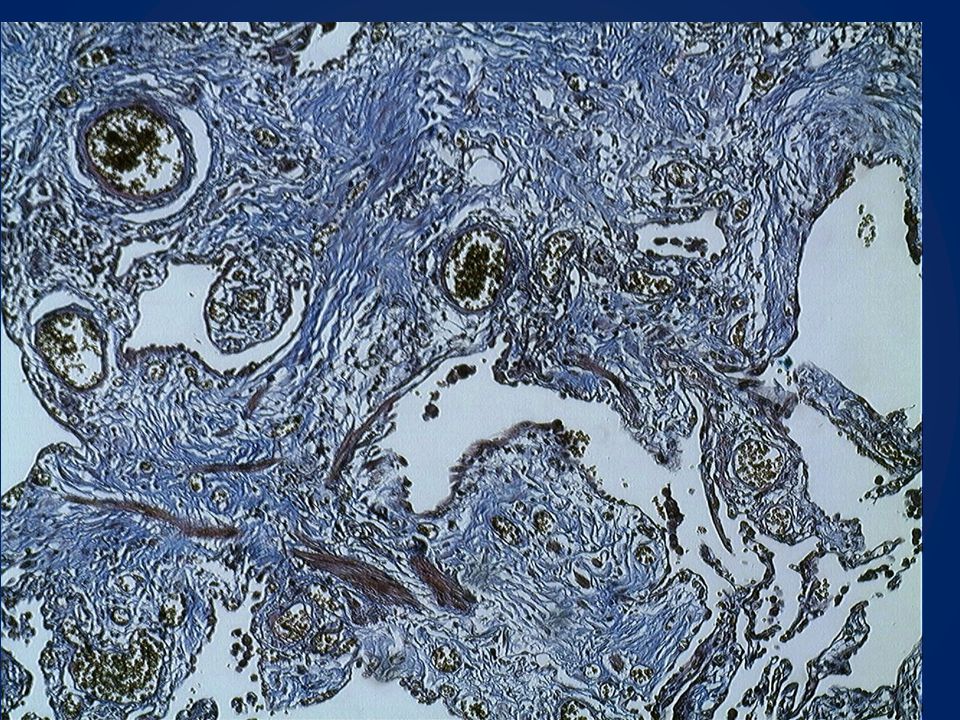
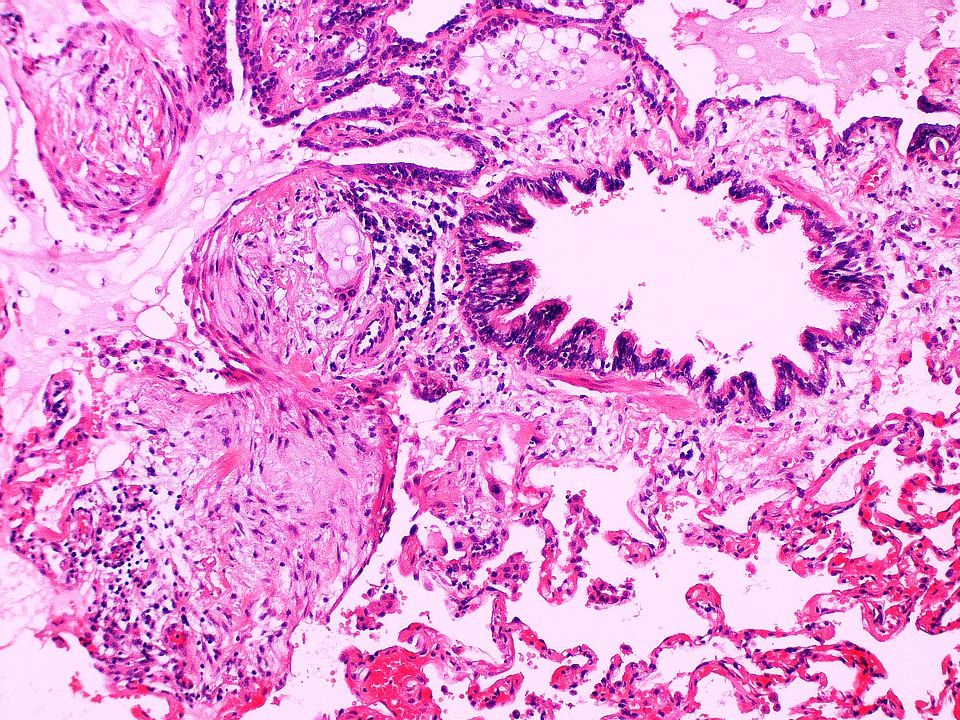
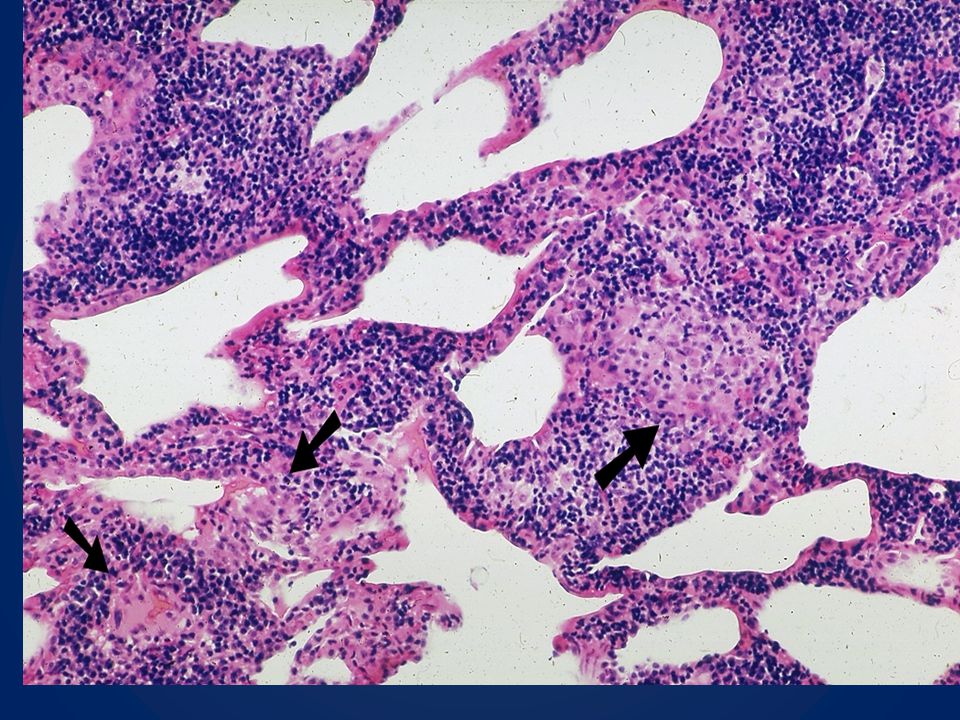
CARACTERISTICAS HISTOLOGICAS FIBROSE DENSA – ALTERAÇOES DE PADRÃO ARQUITETURAL ENVOLVIMENTO PULMONAR IRREGULAR DISTRIBUIÇÃO SUBPLEURAL / PARASSEPTAL FOCOS FIBROBLASTICOS ACHADOS NEGATIVOS PERTINENTES Ausência de outras doenças intersticiais ativas ( ex sarcoidose) Ausência inflamação crônica intensa Ausência de granulomas Ausência de depositos de substancias inorganicas ( ex :asbestos ) Ausência de eosinofilia intensa. HONEYCOMBDense fibrosis causing remodeling of lung architecture with frequent “honeycomb” fibrosis Fibroblastic foci typically scattered at the edges of dense scars Patchy lung involvement Frequent subpleural and paraseptal distribution Pertinent Negative Findings Lack of active lesions of other interstitial diseases (i.e., sarcoidosis or Langerhans’ cell histiocytosis) Lack of marked interstitial chronic inflammation Granulomas: inconspicuous or absent Lack of substantial inorganic dust deposits, i.e., asbestos bodies (except for carbon black pigment) Lack of marked eosinophilia
 Ausência inflamação crônica intensa. Ausência de granulomas. Ausência de depositos de substancias inorganicas ( ex :asbestos ) Ausência de eosinofilia intensa. HONEYCOMBDense fibrosis causing remodeling of lung architecture with frequent. honeycomb fibrosis. Fibroblastic foci typically scattered at the edges of dense scars. Patchy lung involvement. Frequent subpleural and paraseptal distribution. Pertinent Negative Findings. Lack of active lesions of other interstitial diseases (i.e., sarcoidosis or Langerhans’ cell histiocytosis) Lack of marked interstitial chronic inflammation. Granulomas: inconspicuous or absent. Lack of substantial inorganic dust deposits, i.e., asbestos bodies (except for. carbon black pigment) Lack of marked eosinophilia.")
27
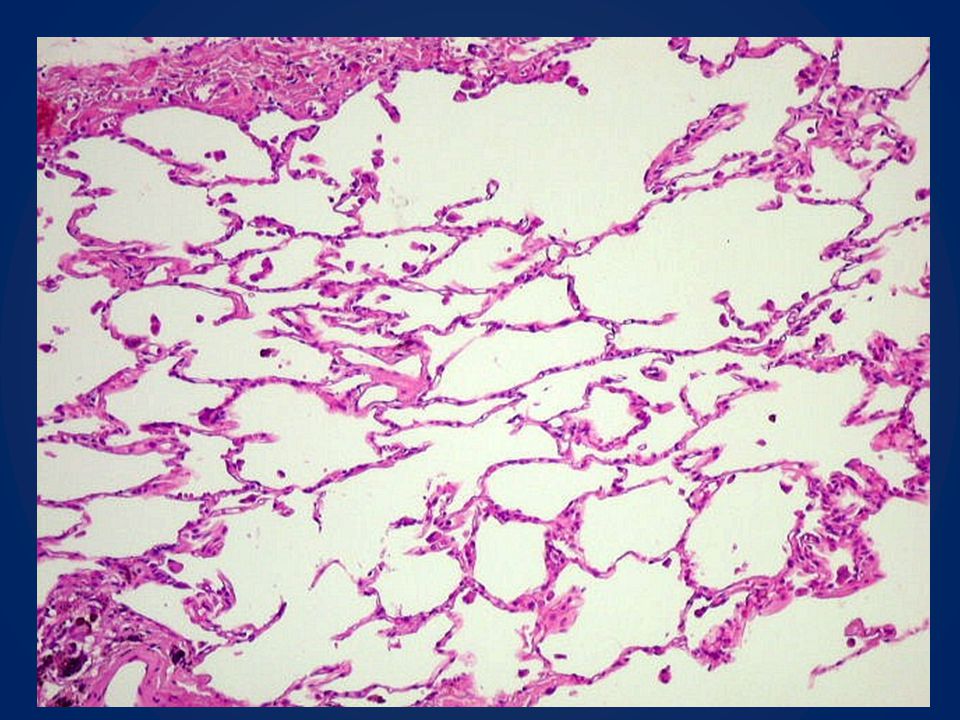
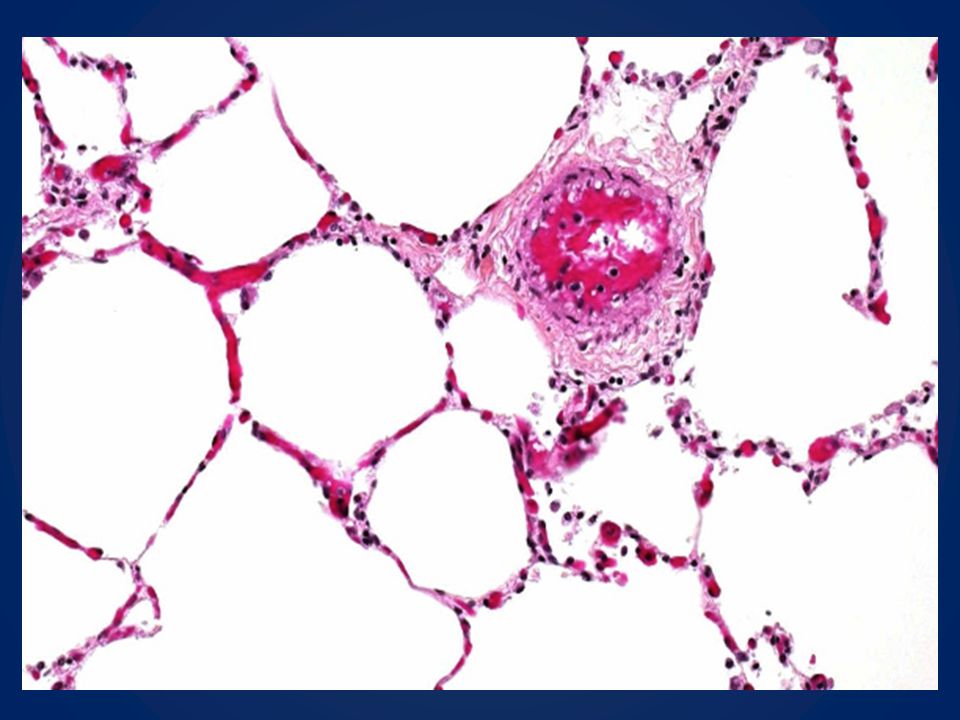
PNEUMONIA INTERSTICIAL USUAL
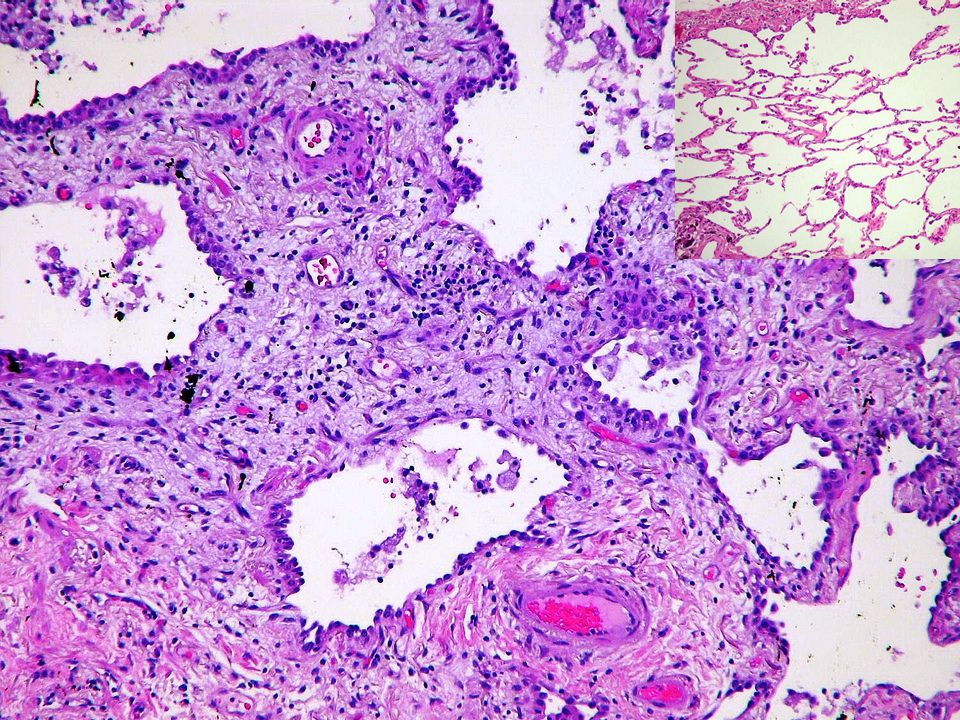
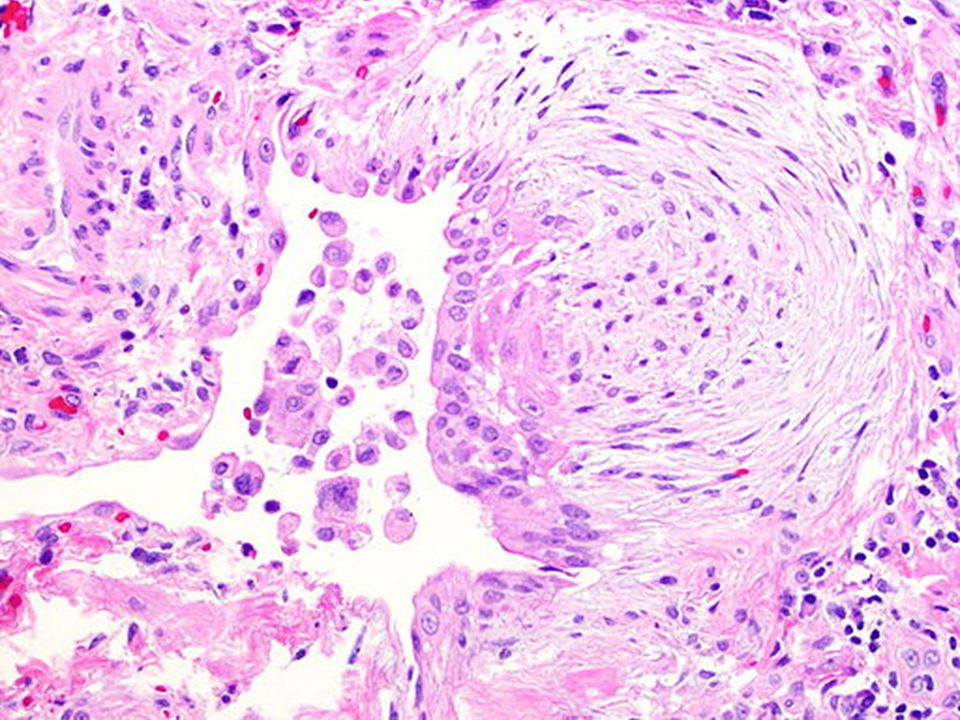
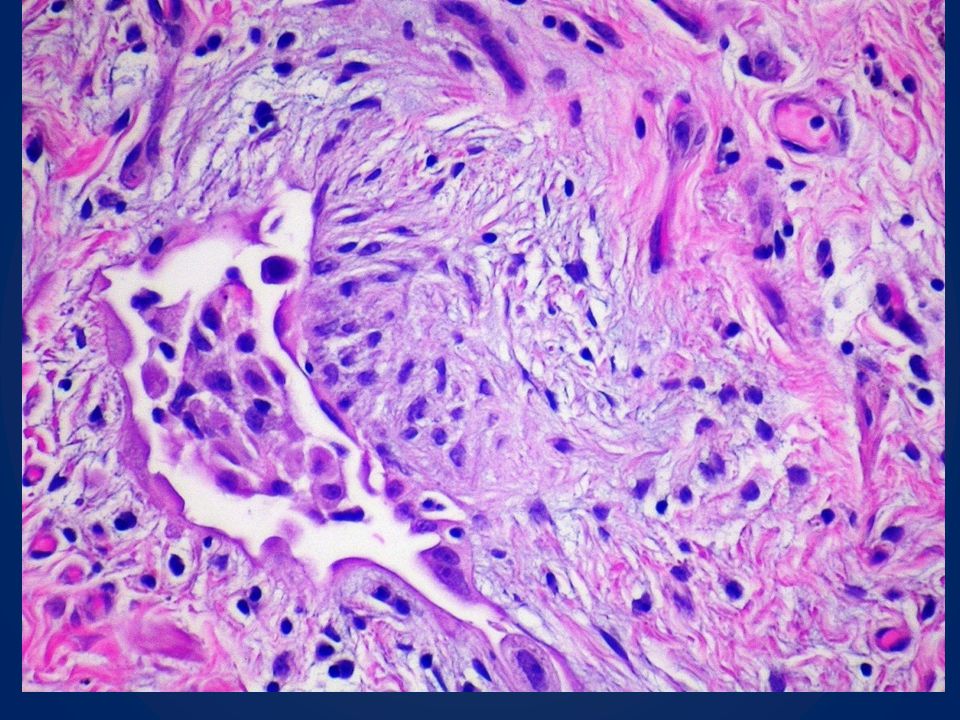
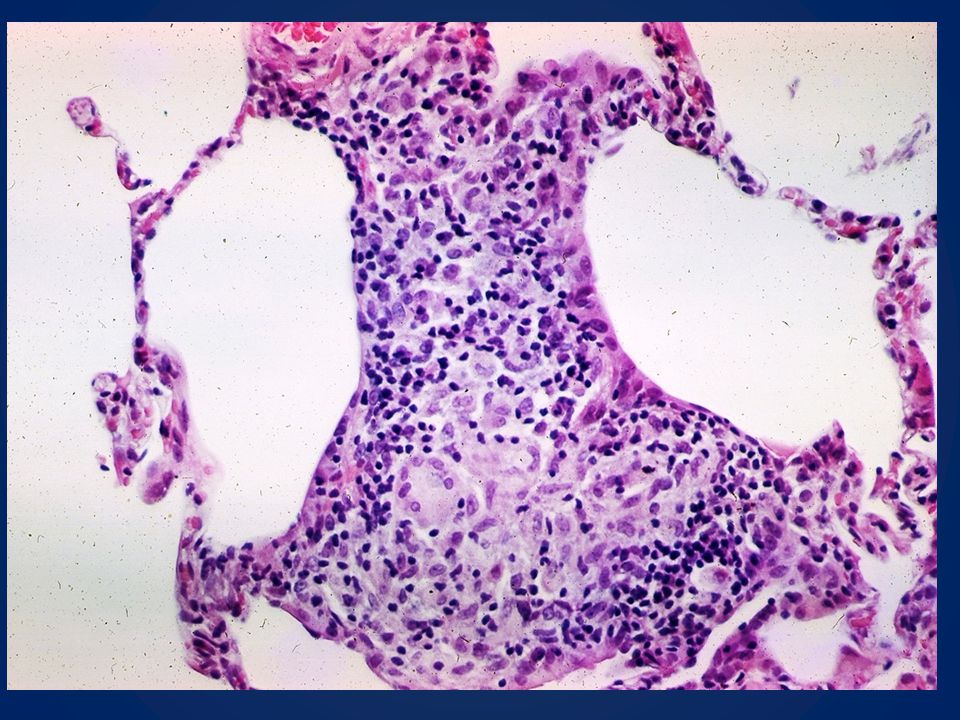
CARACTERISTICAS HISTOLOGICAS FIBROSE DENSA – ALTERAÇOES DE PADRÃO ARQUITETURAL FOCOS FIBROBLASTICOS ENVOLVIMENTO PULMONAR IRREGULAR DISTRIBUIÇÃO SUBPLEURAL / PARASSEPTAL ACHADOS NEGATIVOS PERTINENTES Ausência de outras doenças intersticiais ativas ( ex sarcoidose) Ausência inflamação cronica intensa Ausência de granulomas Ausência de depositos de substancias inorganicas ( ex :asbestos ) Ausência de eosinofilia intensa. HONEYCOMBDense fibrosis causing remodeling of lung architecture with frequent “honeycomb” fibrosis Fibroblastic foci typically scattered at the edges of dense scars Patchy lung involvement Frequent subpleural and paraseptal distribution Pertinent Negative Findings Lack of active lesions of other interstitial diseases (i.e., sarcoidosis or Langerhans’ cell histiocytosis) Lack of marked interstitial chronic inflammation Granulomas: inconspicuous or absent Lack of substantial inorganic dust deposits, i.e., asbestos bodies (except for carbon black pigment) Lack of marked eosinophilia
 Ausência inflamação cronica intensa. Ausência de granulomas. Ausência de depositos de substancias inorganicas ( ex :asbestos ) Ausência de eosinofilia intensa. HONEYCOMBDense fibrosis causing remodeling of lung architecture with frequent. honeycomb fibrosis. Fibroblastic foci typically scattered at the edges of dense scars. Patchy lung involvement. Frequent subpleural and paraseptal distribution. Pertinent Negative Findings. Lack of active lesions of other interstitial diseases (i.e., sarcoidosis or Langerhans’ cell histiocytosis) Lack of marked interstitial chronic inflammation. Granulomas: inconspicuous or absent. Lack of substantial inorganic dust deposits, i.e., asbestos bodies (except for. carbon black pigment) Lack of marked eosinophilia.")
31
PNEUMONIA INTERSTICIAL USUAL
Am J Respir Crit Care Med Vol 183. pp 788–824, 2011

32
DIAGNOSTICO CLINICO X RADIOLOGICO X ANATOMOPATOLOGICO
PNEUMONIA INTERSTICIAL USUAL DIAGNOSTICO CLINICO X RADIOLOGICO X ANATOMOPATOLOGICO

33
Dra Larissa Cardoso Marinho Unidade de Anatomia Patologica
Thank you ! Dra Larissa Cardoso Marinho Unidade de Anatomia Patologica HUB –UnB

Apresentações semelhantes