Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Up to Date Câncer de rim tratamento minimamente invasivo
Álvaro Sarkis Professor Livre Docente Universidade de São Paulo Urologista do Hospital do Servidor Público de São Paulo

2
Outline Nefrectomia minimamente invasiva vs aberta para tumores 4cm a 7cm Crioablação laparoscópica vs PN para tumores renais pequenos: revisão sistemática Evolução funcional e oncológica de NSS para tumores renais >7 cm

3
Nefrectomia minimamente invasiva vs aberta para tumores 4cm a 7cm

4
MSKCC N=280 de 2290

5
Seguimento livre de recidivas e metástases
Mediana de follow-up para OPN 29 meses e MIPN 13 mo, Seguimento curtoi!! Seguimento livre de recidivas e metástases EUROPEAN UROLOGY 61 (2012) 593–599
 593–599.")
6
Nefrectomia parcial para Tumores > 4 cm
EUROPEAN UROLOGY 61 (2012) 593–599
 593–599.")
7
9()% das nefrectomias não são parciais
EUROPEAN UROLOGY 61 (2012) 593–599
 593–599.")
8
Conclusão LPN pode ser feita com segurança em tumores > 4 a 7cm, com aumento de morbidade (fistula 7% laparoscopia vs 5% aberta) PN can be performed safely although with some increased risk of unique complications [22] compared with RN. Published data from patients with tumors 4 cm identify a 12% rate of surgical complications and a 5% rate of urinary fistula [2] for OPN; complication rates for laparoscopic series appear to range from 20% to 37% [16,17] with a urinary fistula rate of 7% [16]. This appears comparable with the one study of robot-assisted PN for tumors 4 cm that cites a urinary fistula rate of 5% [35]. Our standardized prospective institutional complication reporting system with use of detailed retrospective review criteria for adverse events previously demonstrated a higher rate of actual adverse event detection and reporting [40]. This may account for the higher observed rate of overall complications relative to 598 EUROPEAN UROLOGY 61 (2012) 593–599 other published reports, although less so our rate of grade 3 complications (OPN 7%, MIPN 15%) that compares with events in other large series [2]. The association between complications and medical comorbidities is well documen- ted, and the proportion of higher ASA scores in this series are notable, with scores >3 in 44% and 56% of OPN and MIPN cases, respectively, compared with 35% of those reported in other combined series [2].
 593–599. other published reports, although less so our rate of grade 3 complications (OPN 7%, MIPN 15%) that compares with events in other large series [2]. The association between complications and medical comorbidities is well documen- ted, and the proportion of higher ASA scores in this series are notable, with scores >3 in 44% and 56% of OPN and MIPN cases, respectively, compared with 35% of those reported in other combined series [2].")
9
Crioablação laparoscópica vs PN para tumores renais pequenos revisão sistemática

10
Crioablação laparoscópica vs PN para tumores renais pequenos
EUROPEAN UROLOGY 60 (2011) 435–443
 435–443.")
11
EUROPEAN UROLOGY 60 (2011) 435–443
 435–443")
12
Crioablação laparoscópica vs PN para tumores renais pequenos
EUROPEAN UROLOGY 60 (2011) 435–443
 435–443.")
13
Crioablação laparoscópica vs PN para tumores renais pequenos
EUROPEAN UROLOGY 60 (2011) 435–443
 435–443.")
14
Conclusões LCA e PN são opções viáveis para o tratamento de SRMs
LCA tem maior risco de progressão local PN é "gold standard" Both PN and LCA procedures are viable options for management of patients with SRMs. Compared with PN, LCA results in a higher risk of local tumor progression. The risk of perioperative complications appears to be lower following LCA; however, this difference is strongly influ- enced by selection bias, and thus limited conclusions can be made regarding true differences in complications between both procedures. PN is therefore the gold standard for SRMs, but LCA may be indicated in selected patients with significant comorbidity. Balancing cancer control and patient morbidity will be crucial for counseling the patient.

15
Evolução funcional e oncológica de NSS para tumores renais >7 cm

16
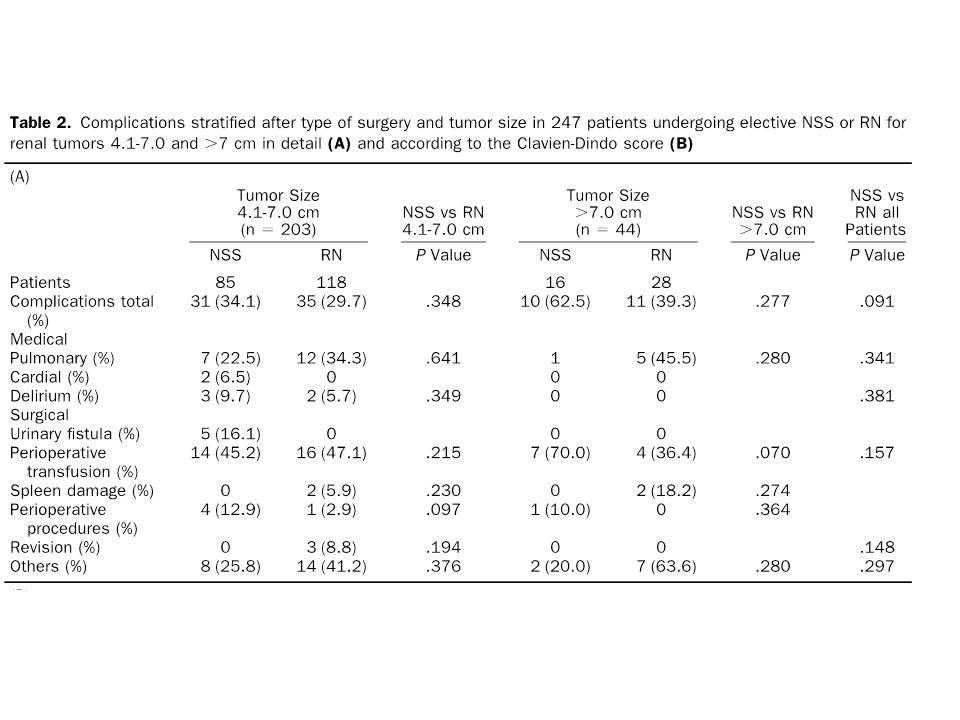
Evolução funcional e oncológica de NSS para tumoes renais >7 cm

17
5767 patients were treated for renal tumours at two institutions from 1984 to 2009.
In 91 patients, elective NSS was performed for renal tumours > 7 cm. The median follow-up was 28 mo (range: 1–247 mo). Twenty- seven patients (29.6%)
. Twenty- seven patients (29.6%)")
18
Comparavel à cirurgia aberta

19
Conclusão NSS para tumores renais > 7cm é viavel e pode ser sempre feita desde que tecnicamente factível* *proposta dos autores This study provides strong evidence of safety and efficacy of elective NSS for renal tumours 7 cm. Oncologic outcomes were equivalent to other studies and to RN series for tumours 7 cm. The risk of postoperative complications was comparable to NSS series for smaller tumours. Regardless of tumour size, elective NSS should be consid- ered for all patients when this surgical approach appears to be technically feasible.

20
Conclusões gerais LPN pode ser feita com segurança em tumores > 4 a 7cm, com aumento de morbidade (fistula 7% lap. vs 5% aberta) LCA e PN são opções viáveis para o tratamento de SRMs LCA tem maior risco de progressão local PN é "gold standard” NSS para tumores renais > 7cm é viavel e pode ser sempre feita desde que tecnicamente factível This study provides strong evidence of safety and efficacy of elective NSS for renal tumours 7 cm. Oncologic outcomes were equivalent to other studies and to RN series for tumours 7 cm. The risk of postoperative complications was comparable to NSS series for smaller tumours. Regardless of tumour size, elective NSS should be consid- ered for all patients when this surgical approach appears to be technically feasible.

22
n addition to a comparable oncological outcome be- tween NSS and RN for renal tumors larger than 4 cm, we have shown that increasing age, ASA score 34, preop- erative eGFR, and RN are associated with the develop- ment of CKD in a balanced cohort for patients treated by NSS or RN for renal tumors 4 cm. NSS maintains renal function with comparable perioperative morbidity to RN. It is therefore reasonable to postulate that NSS should be performed, whenever technically feasible.

Apresentações semelhantes