Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Asma e pequenas vias aéreas: Preciso me preocupar?
CURSO NACIONAL DE ATUALIZAÇÃO EM PNEUMOLOGIA SÃO PAULO, 2011 J. ALBERTO NEDER Prof. Titular Livre Docente Chefe da Disciplina de Pneumologia UNIFESP-EPM

2
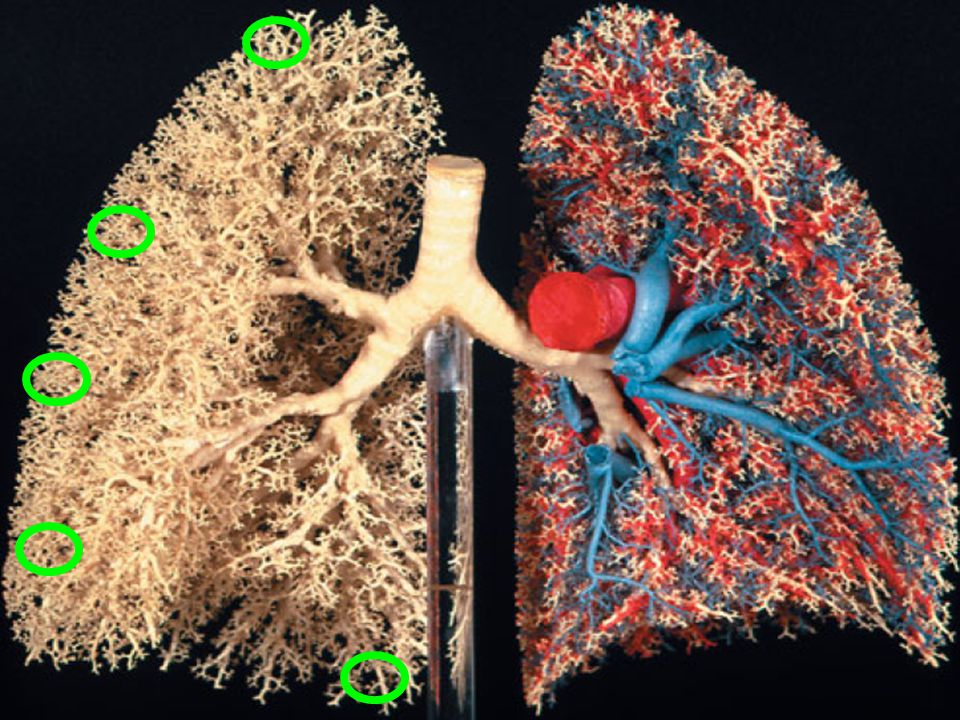
Árvore Brônquica

3
Indo da traquéia ao alvéolo....
PVA < 2 mm, semi-membranoso, sem cartilagem

4
O quê sustenta a PVA ?

5
Resistência ao fluxo de ar em humanos
Ou seja, a somatória de milhões de tubinhos é muito maior do que a traquéia !

6
As pequenas vias aéreas caracterizam-se por:
A) Pequeno diâmetro individual e elevada resistência global ao fluxo B) Estrutura cartilaginosa, estabilidade em baixos volumes pulmonares C) Baixa resistência e dependência da tração alveolar radial D) Estabilidade independentemente do volume e diâmetro > 2 cm
 Pequeno diâmetro individual e elevada resistência global ao fluxo. B) Estrutura cartilaginosa, estabilidade em baixos volumes pulmonares. C) Baixa resistência e dependência da tração alveolar radial. D) Estabilidade independentemente do volume e diâmetro > 2 cm.")
7
As pequenas vias aéreas caracterizam-se por:
A) Pequeno diâmetro individual e elevada resistência global ao fluxo B) Estrutura cartilaginosa, estabilidade em baixos volumes pulmonares C) Baixa resistência e dependência da tração alveolar radial D) Estabilidade independentemente do volume e diâmetro > 2 cm
 Pequeno diâmetro individual e elevada resistência global ao fluxo. B) Estrutura cartilaginosa, estabilidade em baixos volumes pulmonares. C) Baixa resistência e dependência da tração alveolar radial. D) Estabilidade independentemente do volume e diâmetro > 2 cm.")
8
Asma – Definição: 2002 Há evidências que tanto a inflamação aguda quanto a crônica estão irregularmente distribuídas nas vias aéreas, incluindo as pequenas vias aéreas (menos de 2 mm de diâmetro), e no parênquima. Esta distribuição disseminada da inflamação está associada com implicações para a liberação de medicações inaladas para áreas apropriadas do pulmão.
, e no parênquima. Esta distribuição disseminada da inflamação está associada com implicações para a liberação de medicações inaladas para áreas apropriadas do pulmão.")
9
Avaliação das pequenas vias aéreas
Podemos avaliar especificamente as pequenas vias aéreas? Pequenas vias aéreas Testes de função pulmonar Imagem Oscilometria de impulso Óxido nítrico no ar exalado

10
PIP NO FLOW EXP FORCED EXP Porquê o VEF1 NÃO reflete bem
a função das PVA ? NO FLOW EXP Ou seja, a mesma força que impulsiona o ar do alvéolo na expiração forçada, limita sua eliminação nas médias e grandes vias aéreas PIP FORCED EXP

11
Correlações fisiológicas da inflamação do pulmão distal na asma
Correlação Spearman p VEF1 vs mastócitos -0,07 0,9 VEF1 vs linfócitos 0,39 0,3 Sutherland et al JACI 2004 Background The distal lung is an important site of inflammation in asthma. Maximal midexpiratory flows and the ratio of maximal:partial flows are purported to reflect distal lung function. Objective We obtained contemporaneous transbronchial biopsy, spirometry, and plethysmography to describe more accurately the relationship between physiology and distal lung inflammation in asthma. Methods Ten patients with severe, persistent asthma with mean ± SE FEV1 of 2.8 ± 0.2 L and overnight fall in FEV1 of 22.8% ± 3.8% underwent transbronchial biopsy, spirometry, maximal midexpiratory flows, maximal:partial ratio, and lung volumes, all at 4 am. Morphometric analysis was performed after immunohistochemistry for eosinophils, lymphocytes, macrophages, mast cells, and neutrophils. Results Maximal midexpiratory flows, maximal:partial ratio, FEV1, and forced vital capacity were not significantly correlated with alveolar tissue inflammation. However, the degree of eosinophilic alveolar inflammation was significantly and positively correlated with both total lung capacity (Spearman ρ = 0.70; P = .03) and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation. Sutherland et al. JACI 2004
 and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion. Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation. Sutherland et al. JACI")
12
Mede melhor a função das PVA De ser sempre expresso em relação
FEF 25-75% Mede melhor a função das PVA do que o VEF1 De ser sempre expresso em relação a CVF MAS É MUITO VARIÁVEL !!

13
Outros parâmetros: FEF 25-75% Correlação Spearman p
Eosinófilos vs FEF25-75 - 0,25 0,5 Macrófagos vs FEF25-75 1,0 Neutrófilos vs FEF25-75 - 0,16 0,7 Linfócitos vs FEF25-75 - 0,19 0,6 Dados conflitantes Níveis de FEF25–75% são influenciados por alterações de volume pulmonar e obstrução das grandes vias aéreas Sutherland et al JACI 2004 Background The distal lung is an important site of inflammation in asthma. Maximal midexpiratory flows and the ratio of maximal:partial flows are purported to reflect distal lung function. Objective We obtained contemporaneous transbronchial biopsy, spirometry, and plethysmography to describe more accurately the relationship between physiology and distal lung inflammation in asthma. Methods Ten patients with severe, persistent asthma with mean ± SE FEV1 of 2.8 ± 0.2 L and overnight fall in FEV1 of 22.8% ± 3.8% underwent transbronchial biopsy, spirometry, maximal midexpiratory flows, maximal:partial ratio, and lung volumes, all at 4 am. Morphometric analysis was performed after immunohistochemistry for eosinophils, lymphocytes, macrophages, mast cells, and neutrophils. Results Maximal midexpiratory flows, maximal:partial ratio, FEV1, and forced vital capacity were not significantly correlated with alveolar tissue inflammation. However, the degree of eosinophilic alveolar inflammation was significantly and positively correlated with both total lung capacity (Spearman ρ = 0.70; P = .03) and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation. Sutherland et al. JACI 2004
 and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion. Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation. Sutherland et al. JACI")
14
Aprisionamento de ar e pequenas vias aéreas
Em paciente com aumento do VR e diminuição da CV, a causa mais provável é doença das pequenas vias aéreas Imagem (TCAR) Testes de Função Pulmonar APRISIONAMENTO DE AR NORMAL VR CVF Inspiração Contoli et al. Allergy 2010 The involvement of small airways in the pathogenesis of asthma and chronic obstructive pulmonary disease (COPD) has been debated for a long time. However, a proper definition of small airway disease is still lacking, and neither a widely accepted biomarker nor a functional parameter to assess small airway abnormalities and to explore the effect of tested compounds on small airways is available. Aiming towards increased knowledge and consensus on this topic, this perspective paper intends to (i) strengthen awareness among the scientific community on the role of small airways in asthma and COPD; (ii) examine the pros and cons of some biological, functional and imaging parameters in the assessment of small airway abnormalities; and (iii) discuss the evidence for distal airway pharmacological targeting in asthma and COPD. Expiração Contoli et al. Allergy 2010 14
 Testes de Função Pulmonar. APRISIONAMENTO DE AR. NORMAL. VR. CVF. Inspiração. Contoli et al. Allergy The involvement of small airways in the pathogenesis of asthma and chronic obstructive pulmonary disease (COPD) has been debated for a long time. However, a proper definition of small airway disease is still lacking, and neither a widely accepted biomarker nor a functional parameter to assess small airway abnormalities and to explore the effect of tested compounds on small airways is available. Aiming towards increased knowledge and consensus on this topic, this perspective paper intends to (i) strengthen awareness among the scientific community on the role of small airways in asthma and COPD; (ii) examine the pros and cons of some biological, functional and imaging parameters in the assessment of small airway abnormalities; and (iii) discuss the evidence for distal airway pharmacological targeting in asthma and COPD. Expiração. Contoli et al. Allergy")
15
CVF x CVL CVF CV lenta Em indivíduos sem obstrução deve se < 0,20L CVF < CV em paciente com DVO - Compressão dinâmica de VV aéreas, com alçaponamento de ar na manobra de CVF OU SEJA, AS PVA SE FECHAM MAIS FACILMENTE QUANDO ASSOPRAMOS COM FORÇA !

16
Outros parâmetros: VR % ΔVEF1 % ΔCVF Medidas basais BD
20 10 -10 -20 -30 -40 -50 % ΔVEF1 % ΔCVF 1,4 1,2 1 0,8 0,6 0,4 0,2 FEV1 FVC RV % predicted Medidas basais BD Brown et al. J Appl Physiol 2006

17
Eosinófilos no pulmão distal se correlacionam com o volume
de gás torácico Sutherland et al JACI 2004 VGT (litro) Eosinófilos no pulmão distal (mm3/mm2) 5.5 6.5 6 5 4.5 4 2 3 2.5 3.5 .02 .04 .05 .08 .1 r = 0,65 p = 0,04 Sutherland et al JACI 2004 Background The distal lung is an important site of inflammation in asthma. Maximal midexpiratory flows and the ratio of maximal:partial flows are purported to reflect distal lung function. Objective We obtained contemporaneous transbronchial biopsy, spirometry, and plethysmography to describe more accurately the relationship between physiology and distal lung inflammation in asthma. Methods Ten patients with severe, persistent asthma with mean ± SE FEV1 of 2.8 ± 0.2 L and overnight fall in FEV1 of 22.8% ± 3.8% underwent transbronchial biopsy, spirometry, maximal midexpiratory flows, maximal:partial ratio, and lung volumes, all at 4 am. Morphometric analysis was performed after immunohistochemistry for eosinophils, lymphocytes, macrophages, mast cells, and neutrophils. Results Maximal midexpiratory flows, maximal:partial ratio, FEV1, and forced vital capacity were not significantly correlated with alveolar tissue inflammation. However, the degree of eosinophilic alveolar inflammation was significantly and positively correlated with both total lung capacity (Spearman ρ = 0.70; P = .03) and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation.
 Eosinófilos no pulmão distal (mm3/mm2) r = 0,65. p = 0,04. Sutherland et al JACI Background. The distal lung is an important site of inflammation in asthma. Maximal midexpiratory flows and the ratio of maximal:partial flows are purported to reflect distal lung function. Objective. We obtained contemporaneous transbronchial biopsy, spirometry, and plethysmography to describe more accurately the relationship between physiology and distal lung inflammation in asthma. Methods. Ten patients with severe, persistent asthma with mean ± SE FEV1 of 2.8 ± 0.2 L and overnight fall in FEV1 of 22.8% ± 3.8% underwent transbronchial biopsy, spirometry, maximal midexpiratory flows, maximal:partial ratio, and lung volumes, all at 4 am. Morphometric analysis was performed after immunohistochemistry for eosinophils, lymphocytes, macrophages, mast cells, and neutrophils. Results. Maximal midexpiratory flows, maximal:partial ratio, FEV1, and forced vital capacity were not significantly correlated with alveolar tissue inflammation. However, the degree of eosinophilic alveolar inflammation was significantly and positively correlated with both total lung capacity (Spearman ρ = 0.70; P = .03) and thoracic gas volume (ρ = 0.62; P = .05). Correlation between eosinophils and other lung volumes was not observed. Other inflammatory cell types did not correlate with lung volumes. Conclusion. Purported physiologic measures of distal lung function are poorly correlated with histopathologic evidence of distal lung inflammation. Measurement of lung volumes more accurately reflects eosinophilic distal lung inflammation.")
18
Lavado de N2 Respiração Única
Closing volume (CV) Closing capacity (CC) Slope of phase III (DN2) 18
 Closing. capacity (CC) Slope of phase III (DN2) 18.")
19
PIOR DISTRIBUIÇÃO DA VENTILAÇÃO
Avaliação das pequenas vias aéreas pelo lavado de N2SB Inclinação da Fase III do N2 exalado (resp 100% O2) DROGA A DROGA B INCLINAÇÃO MAIOR = PIOR DISTRIBUIÇÃO DA VENTILAÇÃO PELAS PVA (J Allergy Clin Immunol 2006;118:340-6.)
 DROGA A. DROGA B. INCLINAÇÃO MAIOR = PIOR DISTRIBUIÇÃO DA VENTILAÇÃO. PELAS PVA. (J Allergy Clin Immunol 2006;118:340-6.)")
20
VOLUME DE FECHAMENTO ∆ Vol (I) * Após 4 semanas Após 12 semanas
0,2 -0,5 0,1 0,0 -0,1 -0,2 -0,3 -0,4 Após 4 semanas ∆ Vol (I) Após 12 semanas # p<0.08 vs. basal CC: capacidade de fechamento DROGA A . DROGA B. * Paggiaro et al. Expert Rev. Resp. Med 2008 The fixed combination of beclomethasone and formoterol (BDP/F) is an extrafine hydrofluoroalkane-propelled formulation characterized by a small particle size and high particle deposition in the lower airways. The product is manufactured using a specific technology known as Modulite®, the advantages of which include a stable and uniform dose delivery and flexibility to tailor particle size. The high fraction of drug available for lung deposition and the resulting low fraction remaining in the upper airways account for a high efficacy coupled with a low systemic bioavailability, therefore making this combination competitive compared with other inhaled corticosteroid/long-acting â2-agonist (ICS/LABA) fixed combinations currently available. A 6-month study comparing BDP/F fixed combination with BDP and formoterol administered via separate inhalers showed a comparable efficacy on lung function and a greater efficacy in favor of the BDP/F fixed combination in terms of improvements in symptom scores and asthma control. Comparative studies in moderate-tosevere asthmatics have shown that the BDP/F combination displays a comparable efficacy to that of ICS/LABA combinations across the different asthma outcomes measured. The smaller particle size of this BDP/F combination in comparison with other ICS/LABA combinations makes it potentially more effective on small airways, a specific target for asthma treatment. This should be confirmed by specifically designed studies. Future development of this combination will include the evaluation of efficacy in maintaining asthma control using a stepdown approach and the assessment of its use as maintenance and reliever therapy, since formoterol has already been shown to be an effective reliever medication in asthma in another inhaler containing budesonide/formoterol. 2. Papi et al Allergy 2007 Background: Recommended treatment for moderate to severe asthma is the combination of an inhaled corticosteroid and a long-acting beta2-agonist. The present study was designed to compare a new fixed combination of extrafine beclomethasone and formoterol, with the fixed combination fluticasone and salmeterol. Methods: This was a phase III, multinational, multicentre, double-blind, randomized, two-arm parallel groups, controlled study. After a 2-week run-in period, 228 patients with moderate to severe asthma were randomized to a 12-week treatment with either beclomethasone 100 lg plus formoterol 6 lg or fluticasone 125 lg plus salmeterol 25 lg, both delivered two inhalations b.i.d. via a pressurized metered dose inhaler. Results: The analysis of noninferiority on the primary outcome, morning peak expiratory flow in the last 2 weeks of treatment, showed no difference between groups (difference )3.32 l/min; 95% CI )17.92 to 11.28). A significant improvement from baseline in lung function, symptom score and rescue medication use was observed in both groups at all time points. Beclomethasone plus formoterol combination showed a significantly faster onset of bronchodilation when compared with fluticasone plus salmeterol with the difference maintained for up to 1 h postdosing. No differences were observed between treatments in the rate of asthma exacerbations, frequency of adverse events and overnight urinary cortisol/creatinine ratio. Conclusions: The new combination of extrafine beclomethasone plus formoterol is not inferior to the marketed combination of fluticasone and salmeterol in terms of efficacy and tolerability, with the advantage of a faster onset of bronchodilation. (ClinicalTrials.gov number, NCT ). Paggiaro et al. Expert Rev. Resp. Med. 2008 2. Papi et al Allergy 2007 20
 Após 12 semanas. # p<0.08 vs. basal. CC: capacidade de fechamento. DROGA A. . DROGA B. * Paggiaro et al. Expert Rev. Resp. Med The fixed combination of beclomethasone and formoterol (BDP/F) is an extrafine. hydrofluoroalkane-propelled formulation characterized by a small particle size and high. particle deposition in the lower airways. The product is manufactured using a specific. technology known as Modulite®, the advantages of which include a stable and uniform dose. delivery and flexibility to tailor particle size. The high fraction of drug available for lung. deposition and the resulting low fraction remaining in the upper airways account for a high. efficacy coupled with a low systemic bioavailability, therefore making this combination. competitive compared with other inhaled corticosteroid/long-acting â2-agonist (ICS/LABA) fixed combinations currently available. A 6-month study comparing BDP/F fixed combination. with BDP and formoterol administered via separate inhalers showed a comparable efficacy on. lung function and a greater efficacy in favor of the BDP/F fixed combination in terms of. improvements in symptom scores and asthma control. Comparative studies in moderate-tosevere. asthmatics have shown that the BDP/F combination displays a comparable efficacy to. that of ICS/LABA combinations across the different asthma outcomes measured. The smaller. particle size of this BDP/F combination in comparison with other ICS/LABA combinations. makes it potentially more effective on small airways, a specific target for asthma treatment. This should be confirmed by specifically designed studies. Future development of this. combination will include the evaluation of efficacy in maintaining asthma control using a stepdown. approach and the assessment of its use as maintenance and reliever therapy, since. formoterol has already been shown to be an effective reliever medication in asthma in another. inhaler containing budesonide/formoterol. 2. Papi et al Allergy Background: Recommended treatment for moderate to severe asthma is the. combination of an inhaled corticosteroid and a long-acting beta2-agonist. The. present study was designed to compare a new fixed combination of extrafine. beclomethasone and formoterol, with the fixed combination fluticasone and. salmeterol. Methods: This was a phase III, multinational, multicentre, double-blind, randomized, two-arm parallel groups, controlled study. After a 2-week run-in. period, 228 patients with moderate to severe asthma were randomized to a. 12-week treatment with either beclomethasone 100 lg plus formoterol 6 lg or. fluticasone 125 lg plus salmeterol 25 lg, both delivered two inhalations b.i.d. via a pressurized metered dose inhaler. Results: The analysis of noninferiority on the primary outcome, morning peak. expiratory flow in the last 2 weeks of treatment, showed no difference between. groups (difference )3.32 l/min; 95% CI )17.92 to 11.28). A significant. improvement from baseline in lung function, symptom score and rescue medication. use was observed in both groups at all time points. Beclomethasone plus. formoterol combination showed a significantly faster onset of bronchodilation. when compared with fluticasone plus salmeterol with the difference. maintained for up to 1 h postdosing. No differences were observed between. treatments in the rate of asthma exacerbations, frequency of adverse events. and overnight urinary cortisol/creatinine ratio. Conclusions: The new combination of extrafine beclomethasone plus formoterol. is not inferior to the marketed combination of fluticasone and salmeterol in. terms of efficacy and tolerability, with the advantage of a faster onset of bronchodilation. (ClinicalTrials.gov number, NCT ). Paggiaro et al. Expert Rev. Resp. Med Papi et al Allergy")
21
Medida da resistência das vias aéreas
pela Técnica da Oscilação Forçada (FOT) v FOT pode complementar ou mesmo substituir a espirometria para pacientes que tem dificuldade para realizar uma espirometria. FOT utiliza sinais externos de pressão aplicada e os seus resultados de fluxos para determinar parâmetros de mecânica pulmonar. FOT minimiza demandas e requer apenas cooperação passiva dos pacientes v 21
 v. FOT pode complementar ou mesmo substituir a espirometria para pacientes que tem dificuldade para realizar uma espirometria. FOT utiliza sinais externos de pressão aplicada e os seus resultados de fluxos para determinar parâmetros de mecânica pulmonar. FOT minimiza demandas e requer apenas cooperação passiva dos pacientes. v. 21.")
22
Analisador de Quimiluminescência
Medida do NO exalado online Analisador de Quimiluminescência Bomba Gerador de ozônio Tubo de teflon Bocal Fotomultiplicador Registro dos resultados Resistência ~5cm H20 NO + O3 NO2 + O2 NO2 NO2 +

23
Testes Funcionais x Nível de Obstrução
VEF1 / CVF SGaw R Alta Freq RL 2 mm RP VEF1 ou CVF VR R Baixa Freq Volume de fechamento 23

24
Qual dos seguintes CONJUNTOS de alterações funcionais seria mais esperado num paciente com extenso comprometimento das pequenas vias aéreas

25
Qual dos seguintes CONJUNTOS de alterações funcionais seria mais esperado num paciente com extenso comprometimento das pequenas vias aéreas

26
PVA Normal x Asma

27
A progressão da inflamação das PVA na asma

28
Inflamação das PVA na Asma
Am J Respir Crit Care Med 154 (1996), pp. 1505–1510
, pp. 1505–1510.")
29
INFLAMAÇÃO NAS PEQUENAS VIAS AÉREAS IMPACTOS SOBRE OS SINTOMAS DA ASMA
+ # * Concentração de óxido nítrico (NO) alveolar, em pacientes asmáticos com ou sem sintomas noturnos e comparação com voluntários normais. Ref. Lehtimaki et al. Eur Respir J 2002
 alveolar, em pacientes asmáticos com ou sem sintomas noturnos e comparação com voluntários normais. Ref. Lehtimaki et al. Eur Respir J")
30
O PROCESSO INFLAMATÓRIO. NA ASMA, ACOMETE
TANTO AS GRANDES COM AS PEQUENAS VIAS AÉREAS T cells and eosinophils increased in small airways Cytokines increased in small airways Células T e eosinófilos aumentam nas pequenas vias aéreas Citocinas aumentam nas pequenas vias aéreas Vias aéreas < 2 mm Pi < 2 mm > 2 mm Vias aéreas < 2 mm Pi Vias aéreas > 2 mm Pi Ref. Tulic & Hamid, CHEST 2003; 123:348S–355S

31
Inflamação das PVA na Asma
Hamid, Y. Song, T.C. Kotsimbos, E. Minshall, T.R. Bai and R.G. Hegele et al., Inflammation of small airways in asthma, J Allergy Clin Immunol 100 (1997), pp. 44–51
, pp. 44–51.")
32
Inflamação das PVA na Asma
Taha RA, Minshall EM, Miotto D, et al. Eotaxin and monocyte chemotactic protein-4 mRNA expression in small airways of asthmatic and nonasthmatic individuals. J Allergy Clin Immunol 1999;103:479

33
Contrastando as PVA na Asma e na DPOC

34
PVA na ASMA nonononononono

35
NA PRÁTICA, QUANDO SUSPEITO DE MAIOR ACOMETIMENTO DAS PVA ??
“Pistas” clínicas Controle parcial apesar de tratamento otimizado Sintomas noturnos particularmente intensos “Pistas” funcionais Asmático com distúrbio “inespecífico” Grande diferença CVF-CV Asmático que recruta volume (ganha CVF) com BD “Pistas” estruturais Aprisionamento expiratório exuberante Hiperinsuflação desproporcional ao esperado pelo VEF1
 com BD. Pistas estruturais. Aprisionamento expiratório exuberante. Hiperinsuflação desproporcional ao esperado pelo VEF1.")
36
Qual dos seguintes pacientes teria maior probabilidade de apresentar extenso comprometimento das pequenas vias aéreas ?

37
Qual dos seguintes pacientes teria maior probabilidade de apresentar extenso comprometimento das pequenas vias aéreas ?

Apresentações semelhantes