Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Dor em Medicina Física e de Reabilitação
Unidade de Ensino de Medicina Física e de Reabilitação Faculdade de Ciências Médicas de Lisboa This slide illustrates three broad categories of Pain: neuropática (pathologic), nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ;11-57 Additional key words: descriptor
, nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References. International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ; Additional key words: descriptor.")
2
Dor Experiência sensorial e emocional desagradável, associada a uma lesão tecidular real ou potencial, ou que é vivida como tal International Association for the Study of Pain (IASP), 1994
,")
3
Dor Défice funcional Ansiedade Depressão Perturbações do sono
Patients who suffer from chronic Pain experience difficulties initiating and maintaining sleep and are often depressed and anxious. The inter-relationship between these three factors, as shown on this slide, is complex, but must be considered carefully if tratamento for neuropathic pain is to be satisfactory. The key talking points on this slide are as follows: Although most Pain disorders begin with injury or disease, their course and outcome are affected by emotional, behavioral and social factors. An individual’s emotional reaction to, and capacity to cope with, the fluctuating course of neuropathic pain disorders and their complications such as physical impairment, disability, and loss of role functioning will also affect outcome. Chronic Pain significantly interferes with sleep, with most studies showing a positive correlation between Pain intensity and degree of sleep disturbance. Many chronic Pain patients have sinais and sintomas of depression and anxiety; sleep deprivation can lead to anxiety, and depression can be both the causa and result of sleep deprivation. Chronic Pain, sleep disturbances, and depression/anxiety must be addressed if patients are to be restored to optimal functionality. Physicians must evaluate all aspects of Pain, sleep and mood in patients with chronic Pain. Controlo and tratamento should address both the Pain and the comorbidities, to improve daily functioning, and enhance quality of life. Reference Nicholson and Verma. Pain Med. 2004;5(suppl. 1):S9-S27 Additional key words: mood Ansiedade Depressão Perturbações do sono Nicholson and Verma. Pain Med. 2004;5 (suppl. 1):S9-S27
:S9-S27. Additional key words: mood. Ansiedade Depressão. Perturbações do sono. Nicholson and Verma. Pain Med. 2004;5 (suppl. 1):S9-S27.")
4
Desempenha um papel protector Em geral, identifica-se uma agressão
Dor aguda Dor crónica ≥3–6 meses Desempenha um papel protector Em geral, identifica-se uma agressão Não tem um papel protector Deteriora a saúde e a funcionalidade This slide illustrates how acute and chronic pain are often classified along a pain continuum.

5
Dor nociceptiva Dor causada por lesão tecidular (musculo-esquelética, cutânea ou visceral) Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed ;11-57 This slide illustrates three broad categories of Pain: neuropática (pathologic), nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ;11-57 Additional key words: descriptor
. Textbook of Pain. 4th Ed ; This slide illustrates three broad categories of Pain: neuropática (pathologic), nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References. International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ; Additional key words: descriptor.")
6
Dor nociceptiva Experiência sensorial, traduzindo-se numa resposta de neurónios sensoriais periféricos específicos (nociceptores) a estímulos nóxicos (nocivos) Habitualmente, a região dolorosa situa-se no local da lesão Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region is typically localized at the site of injury in nociceptive pain. This contrasts with neuropathic pain where the painful region may not necessarily be the same as the site of injury and occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). This is outlined on slide 15. Nociceptive pain usually responds well to conventional analgesics such as acetaminophen (paracetamol), non-steroidal anti-inflammatory drugs (NSAIDs), cyclo-oxygenase (COX)-2 inhibitors or opioids.
 a estímulos nóxicos (nocivos) Habitualmente, a região dolorosa situa-se no local da lesão. Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region is typically localized at the site of injury in nociceptive pain. This contrasts with neuropathic pain where the painful region may not necessarily be the same as the site of injury and occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). This is outlined on slide 15. Nociceptive pain usually responds well to conventional analgesics such as acetaminophen (paracetamol), non-steroidal anti-inflammatory drugs (NSAIDs), cyclo-oxygenase (COX)-2 inhibitors or opioids.")
7
Dor nociceptiva Frequentemente descrita como latejante, moinha ou rigidez Pode ser crónica, mas geralmente é transitória, desaparecendo após cura dos tecidos lesados Responde aos analgésicos “convencionais” Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region is typically localized at the site of injury in nociceptive pain. This contrasts with neuropathic pain where the painful region may not necessarily be the same as the site of injury and occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). This is outlined on slide 15. Nociceptive pain usually responds well to conventional analgesics such as acetaminophen (paracetamol), non-steroidal anti-inflammatory drugs (NSAIDs), cyclo-oxygenase (COX)-2 inhibitors or opioids.
. This is outlined on slide 15. Nociceptive pain usually responds well to conventional analgesics such as acetaminophen (paracetamol), non-steroidal anti-inflammatory drugs (NSAIDs), cyclo-oxygenase (COX)-2 inhibitors or opioids.")
8
Dor nociceptiva crónica
Percepção da dor Informação ascendente Modulação descendente Lesão tecidular Medula espinhal Nervo periférico Note to speaker: this slide contains an animated build to represent the involvement of the nervous system in chronic nociceptive pain (osteoarthritis of the knee). Clicking on this slide will cause subsequent components of this build to appear automatically. In osteoarthritis, chronic pain is caused by activation of local nociceptors by inflammation in the affected joint. These activated nociceptors send impulses along the peripheral (afferent) nerves to the dorsal roots where they enter the spinal cord to reach the dorsal horn. Signals ascend from the sensory nerves via various pathways to the brain where they give rise to the experience of pain. Pathways include the brain stem, thalamus, limbic system and other cortical areas, which are all responsible for processing sensation, emotion, stress, and memory. The brain, in turn, sends signals via descending tracts into the dorsal horn to modulate the incoming (afferent) signals from the painful knee joint, and to evoke a reflex or behavioral response to osteoarthritis pain (e.g. rubbing the painful area and restricting movement), or to inhibit the afferent signal entirely. The goal of osteoarthritis pain treatment is to relieve inflammatory pain with conventional analgesics (acetaminophen [paracetamol], NSAIDS, COX-2 inhibitors or opioids), while maintaining joint function and mobility. Activação de nociceptores locais
. Clicking on this slide will cause subsequent components of this build to appear automatically. In osteoarthritis, chronic pain is caused by activation of local nociceptors by inflammation in the affected joint. These activated nociceptors send impulses along the peripheral (afferent) nerves to the dorsal roots where they enter the spinal cord to reach the dorsal horn. Signals ascend from the sensory nerves via various pathways to the brain where they give rise to the experience of pain. Pathways include the brain stem, thalamus, limbic system and other cortical areas, which are all responsible for processing sensation, emotion, stress, and memory. The brain, in turn, sends signals via descending tracts into the dorsal horn to modulate the incoming (afferent) signals from the painful knee joint, and to evoke a reflex or behavioral response to osteoarthritis pain (e.g. rubbing the painful area and restricting movement), or to inhibit the afferent signal entirely. The goal of osteoarthritis pain treatment is to relieve inflammatory pain with conventional analgesics (acetaminophen [paracetamol], NSAIDS, COX-2 inhibitors or opioids), while maintaining joint function and mobility. Activação de nociceptores locais.")
9
Dor Neuropática Dor iniciada ou causada por disfunção ou lesão primária do sistema nervoso central ou periférico (incluindo o sistema nervoso autónomo) International Association for the Study of Pain. IASP Pain Terminology This slide illustrates three broad categories of Pain: neuropática (pathologic), nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ;11-57 Additional key words: descriptor
 International Association for the Study of Pain. IASP Pain Terminology. This slide illustrates three broad categories of Pain: neuropática (pathologic), nociceptiva (physiologic), and mixed Pain states that encompass both nociceptiva and neuropática components, with examples of common causes of each type of Pain. The key talking points on this slide are as follows: neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causas of neuropathic pain periférica include nevralgia pós-herpética (PHN) and neuropatia diabética periférica (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of neuropathic pain periférica. Nociceptive Pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive Pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute Pain, such as that seen with tissue inflamação and chronic Pain, such that accompanying osteoarthritis, are examples of nociceptiva Pain. Although there are no specific descriptors for each type of Pain, neuropathic pain is frequently described as ‘queimadura or formigueiro’ in quality, while nociceptiva Pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences Pain sensations that are a blend of Pain having a nociceptiva and a neuropática origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptiva Pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References. International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ; Additional key words: descriptor.")
10
Dor neuropática Frequentemente descrita como “descarga”, “choque eléctrico” ou “queimadura” Muitas vezes associada a “formigueiro” ou “dormência” Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region may not necessarily be the same as the site of injury. Pain occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. Neuropathic pain responds poorly to conventional analgesics. There is some evidence to show that opioids may have efficacy in the management of neuropathic pain.
. In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. Neuropathic pain responds poorly to conventional analgesics. There is some evidence to show that opioids may have efficacy in the management of neuropathic pain.")
11
The Journal of Pain, Vol 8, No 2 (February), 2007: pp 118-126
, 2007: pp")
12
Dor neuropática A região dolorosa não se situa, necessariamente, no local da lesão; a dor ocorre no território nervoso da estrutura afectada (nervo, raiz, medula espinal, cérebro) Quase sempre uma situação crónica (por exemplo nevralgia pós-herpética ou dor pós-AVC) Fraca resposta aos analgésicos “convencionais” Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region may not necessarily be the same as the site of injury. Pain occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. Neuropathic pain responds poorly to conventional analgesics. There is some evidence to show that opioids may have efficacy in the management of neuropathic pain.
 Quase sempre uma situação crónica (por exemplo nevralgia pós-herpética ou dor pós-AVC) Fraca resposta aos analgésicos convencionais Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 4 bullets sequentially. The painful region may not necessarily be the same as the site of injury. Pain occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. Neuropathic pain responds poorly to conventional analgesics. There is some evidence to show that opioids may have efficacy in the management of neuropathic pain.")
13
Exemplo de dor neuropática: lesão do nervo cubital após fractura óssea
This slide shows ulnar nerve damage, caused by direct trauma or compression following an elbow fracture, which can result in neuropathic pain. The nerve damage involves destruction of the myelin sheath of the nerve or part of the nerve (axon). Direct nerve trauma is a key cause of neuropathic pain. The pain exists after tissue healing and no longer represents an alert to injury, but indicates dysfunction within the nervous system. Nervo Cubital
. Direct nerve trauma is a key cause of neuropathic pain. The pain exists after tissue healing and no longer represents an alert to injury, but indicates dysfunction within the nervous system. Nervo Cubital.")
14
Informação ascendente Modulação descendente
Percepção da dor Lesão nervosa Informação ascendente Modulação descendente Impulsos gerados no nervo cubital Medula espinhal Note to speaker: this slide contains an animated build to represent the involvement of the nervous system in neuropathic pain (ulnar nerve lesion following bone fracture). Clicking on this slide will cause subsequent components of this build to appear automatically. In ulnar nerve damage, neuropathic pain is caused by direct trauma or compression of the nerve following elbow fracture. Damaged nerve fibers generate abnormal impulses that are transmitted along the sensory (afferent) nerves to the dorsal roots where they enter the spinal cord to reach the dorsal horn. Abnormal impulses over-stimulate the second-order neurons ascending to the cortex through various pathways (brain stem, thalamus, limbic system, and other cortical areas) where pain awareness develops. In neuropathic pain, a lesion or dysfunction of the nervous system may cause an excess of function (positive symptoms) or a deficit of function (negative symptoms): Positive symptoms – spontaneous pain, allodynia (pain due to a stimulus that does not normally provoke pain), dysesthesia, paresthesia, and hyperalgesia Negative symptoms – weakness or loss of sensation (e.g. wrist and hand flexion following ulnar nerve damage). Lesão Nociceptores periféricos
. Clicking on this slide will cause subsequent components of this build to appear automatically. In ulnar nerve damage, neuropathic pain is caused by direct trauma or compression of the nerve following elbow fracture. Damaged nerve fibers generate abnormal impulses that are transmitted along the sensory (afferent) nerves to the dorsal roots where they enter the spinal cord to reach the dorsal horn. Abnormal impulses over-stimulate the second-order neurons ascending to the cortex through various pathways (brain stem, thalamus, limbic system, and other cortical areas) where pain awareness develops. In neuropathic pain, a lesion or dysfunction of the nervous system may cause an excess of function (positive symptoms) or a deficit of function (negative symptoms): Positive symptoms – spontaneous pain, allodynia (pain due to a stimulus that does not normally provoke pain), dysesthesia, paresthesia, and hyperalgesia. Negative symptoms – weakness or loss of sensation (e.g. wrist and hand flexion following ulnar nerve damage). Lesão. Nociceptores periféricos.")
15
Dor neuropática Exemplos Neuropatia diabética periférica (NDP)
Lesão nervosa pós-cirurgia Nevralgia pós-herpética (NPH) Radiculopatia lombar Dor pós-AVC Descritores frequentes “Descarga” “Choque eléctrico” “Queimadura” “Formigueiro” “Dormência” This slide gives an overview of neuropathic pain, with examples of common causes. Neuropathic pain has been defined by the IASP as a pain that is “initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system”.1 Causes of peripheral neuropathic pain include postsurgical and posttraumatic nerve injury, diabetic peripheral neuropathy (DPN), postherpetic neuralgia (PHN) and radiculopathies. Poststroke pain, multiple sclerosis, and spinal cord injuries are all examples of central neuropathic pain. Neuropathic pain is frequently described as a “shooting”, “electric shock-like”, or “burning” pain – commonly associated with “tingling” and/or “numbness”. The painful region may not necessarily be the same as the site of injury. Pain occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. 1. International Association for the Study of Pain (IASP) pain terminology. (last accessed: 14/12/05)
 Radiculopatia lombar. Dor pós-AVC. Descritores frequentes. Descarga Choque eléctrico Queimadura Formigueiro Dormência This slide gives an overview of neuropathic pain, with examples of common causes. Neuropathic pain has been defined by the IASP as a pain that is initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system .1. Causes of peripheral neuropathic pain include postsurgical and posttraumatic nerve injury, diabetic peripheral neuropathy (DPN), postherpetic neuralgia (PHN) and radiculopathies. Poststroke pain, multiple sclerosis, and spinal cord injuries are all examples of central neuropathic pain. Neuropathic pain is frequently described as a shooting , electric shock-like , or burning pain – commonly associated with tingling and/or numbness . The painful region may not necessarily be the same as the site of injury. Pain occurs in the neurological territory of the affected structure (nerve, root, spinal cord, brain). In peripheral neuropathic pain, it is in the territory of the affected nerve or nerve root. In central neuropathic pain, it is related to the site of the lesion in the spinal cord or brain. 1. International Association for the Study of Pain (IASP) pain terminology. (last accessed: 14/12/05)")
16
Dor neuropática – causas centrais
AVC’s Lesões vértebro-medulares Esclerose múltipla Neoplasias neuropathic pain is initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system. Patients with neuropathic pain have chronic Pain, which is typically considered to be Pain that persists beyond the normal time of healing or for more than 3-6 months.This slide lists some of the most commonly encountered peripheral and central causes of neuropathic pain. The key points on this slide are as follows: Any type of peripheral nerve or root injury may lead to neuropathic pain: traumas, entrapments (like carpal tunnel syndrome), postsurgical iatrogenic nerve lesions, amputations, radiculopathies, etc. Metabolic disturbances may also causa neuropathies associated with neuropathic pain, most notably diabetes mellitus but also uremia and hypothyroidism. Infections such as HIV may also result in peripheral nerve damage. Toxins implicated in peripheral nerve injury include chemotherapeutic agents, lead, organophosphorates and alcohol. Glue sniffing has also been associated with neuropathic pain from peripheral neuropathy. Vascular disorders (polyarteritis nodosa, lupus erythematosus), nutritional deficiencies (niacin, thiamine, pyridoxine), and direct effects of cancer due to metastases and infiltration may also causa peripheral neuropathies leading to neuropathic pain. Central neuropathic pain may be present in about 8% of stroke patients, and in about 28% of patients with multiple sclerosis. Spinal cord lesions and tumors are also known, common causes of central neuropathic pain. References Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited. 1999 Galer BS, Dworkin RH (Eds). A clínica guide to neuropathic pain. Minneaplois, MN: McGraw-Hill Healthcare Information. 2000 Woolf CJ, Mannion RJ. Lancet. 1999;353:
, postsurgical iatrogenic nerve lesions, amputations, radiculopathies, etc. Metabolic disturbances may also causa neuropathies associated with neuropathic pain, most notably diabetes mellitus but also uremia and hypothyroidism. Infections such as HIV may also result in peripheral nerve damage. Toxins implicated in peripheral nerve injury include chemotherapeutic agents, lead, organophosphorates and alcohol. Glue sniffing has also been associated with neuropathic pain from peripheral neuropathy. Vascular disorders (polyarteritis nodosa, lupus erythematosus), nutritional deficiencies (niacin, thiamine, pyridoxine), and direct effects of cancer due to metastases and infiltration may also causa peripheral neuropathies leading to neuropathic pain. Central neuropathic pain may be present in about 8% of stroke patients, and in about 28% of patients with multiple sclerosis. Spinal cord lesions and tumors are also known, common causes of central neuropathic pain. References. Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited Galer BS, Dworkin RH (Eds). A clínica guide to neuropathic pain. Minneaplois, MN: McGraw-Hill Healthcare Information Woolf CJ, Mannion RJ. Lancet. 1999;353:")
17
Dor neuropática – causas periféricas
Traumáticas: cirurgia, encarceramento do nervo, amputação Metabólicas: Diabetes Mellitus, urémia Infecciosas: Herpes Zoster, VIH Tóxicas: quimioterapia, alcoolismo Vasculares: Lupus Eritematoso, Poliarterite Nodosa Nutricionais: niacina (ácido nicotínico), tiamina (vit. B1), piridoxina (vit. B6) Neoplasias: metástase, infiltração neuropathic pain is initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system. Patients with neuropathic pain have chronic Pain, which is typically considered to be Pain that persists beyond the normal time of healing or for more than 3-6 months.This slide lists some of the most commonly encountered peripheral and central causes of neuropathic pain. The key points on this slide are as follows: Any type of peripheral nerve or root injury may lead to neuropathic pain: traumas, entrapments (like carpal tunnel syndrome), postsurgical iatrogenic nerve lesions, amputations, radiculopathies, etc. Metabolic disturbances may also causa neuropathies associated with neuropathic pain, most notably diabetes mellitus but also uremia and hypothyroidism. Infections such as HIV may also result in peripheral nerve damage. Toxins implicated in peripheral nerve injury include chemotherapeutic agents, lead, organophosphorates and alcohol. Glue sniffing has also been associated with neuropathic pain from peripheral neuropathy. Vascular disorders (polyarteritis nodosa, lupus erythematosus), nutritional deficiencies (niacin, thiamine, pyridoxine), and direct effects of cancer due to metastases and infiltration may also causa peripheral neuropathies leading to neuropathic pain. Central neuropathic pain may be present in about 8% of stroke patients, and in about 28% of patients with multiple sclerosis. Spinal cord lesions and tumors are also known, common causes of central neuropathic pain. References Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited. 1999 Galer BS, Dworkin RH (Eds). A clínica guide to neuropathic pain. Minneaplois, MN: McGraw-Hill Healthcare Information. 2000 Woolf CJ, Mannion RJ. Lancet. 1999;353:
, tiamina (vit. B1), piridoxina (vit. B6) Neoplasias: metástase, infiltração. neuropathic pain is initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system. Patients with neuropathic pain have chronic Pain, which is typically considered to be Pain that persists beyond the normal time of healing or for more than 3-6 months.This slide lists some of the most commonly encountered peripheral and central causes of neuropathic pain. The key points on this slide are as follows: Any type of peripheral nerve or root injury may lead to neuropathic pain: traumas, entrapments (like carpal tunnel syndrome), postsurgical iatrogenic nerve lesions, amputations, radiculopathies, etc. Metabolic disturbances may also causa neuropathies associated with neuropathic pain, most notably diabetes mellitus but also uremia and hypothyroidism. Infections such as HIV may also result in peripheral nerve damage. Toxins implicated in peripheral nerve injury include chemotherapeutic agents, lead, organophosphorates and alcohol. Glue sniffing has also been associated with neuropathic pain from peripheral neuropathy. Vascular disorders (polyarteritis nodosa, lupus erythematosus), nutritional deficiencies (niacin, thiamine, pyridoxine), and direct effects of cancer due to metastases and infiltration may also causa peripheral neuropathies leading to neuropathic pain. Central neuropathic pain may be present in about 8% of stroke patients, and in about 28% of patients with multiple sclerosis. Spinal cord lesions and tumors are also known, common causes of central neuropathic pain. References. Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited Galer BS, Dworkin RH (Eds). A clínica guide to neuropathic pain. Minneaplois, MN: McGraw-Hill Healthcare Information Woolf CJ, Mannion RJ. Lancet. 1999;353:")
18
Dor neuropática – sintomas “positivos”
Dor espontânea Sensação dolorosa sem estímulo evidente Alodínia Resposta dolorosa a um estímulo habitualmente não doloroso (toque, movimento, frio, calor) Hiperalgesia Resposta aumentada a um estímulo habitualmente doloroso (frio, calor, picada) Disestesia Sensação desagradável, espontânea ou evocada (por exemplo sensação de descarga) Parestesia Sensação anormal não desagradável, espontânea ou evocada (por exemplo sensação de formigueiro, zumbido, vibração) This slide (and the following one) can be placed immediately after slide 39, which summarizes the positive and negative sensory symptoms of neuropathic pain.
 Hiperalgesia. Resposta aumentada a um estímulo habitualmente doloroso (frio, calor, picada) Disestesia. Sensação desagradável, espontânea ou evocada (por exemplo sensação de descarga) Parestesia. Sensação anormal não desagradável, espontânea ou evocada (por exemplo sensação de formigueiro, zumbido, vibração) This slide (and the following one) can be placed immediately after slide 39, which summarizes the positive and negative sensory symptoms of neuropathic pain.")
19
Dor neuropática – sintomas “negativos”
Hipoestesia Diminuição da sensibilidade a estímulos, excluindo os sentidos especiais (por exemplo: toque, dor) Anestesia Perda total de sensibilidade Analgesia Ausência de dor em resposta a estímulos habitualmente dolorosos Hipoalgesia Diminuição da dor em resposta a estímulos habitualmente dolorosos This slide (and the previous one) can be placed immediately after slide 39, which summarizes the positive and negative sensory symptoms of neuropathic pain.
 Anestesia. Perda total de sensibilidade. Analgesia. Ausência de dor em resposta a estímulos habitualmente dolorosos. Hipoalgesia. Diminuição da dor em resposta a estímulos habitualmente dolorosos. This slide (and the previous one) can be placed immediately after slide 39, which summarizes the positive and negative sensory symptoms of neuropathic pain.")
20
A geração da dor neuropática ocorre ao nível do próprio sistema de transmissão da dor, com envolvimento de fibras Aβ, Aδ e C

21
Nociceptivo, (mecânico, térmico ou químico) Nociceptores Aδ, C
Função do nervo Estímulo Aferente primário Sensação Normal Inócuo, mecânico Aβ Toque normal Nociceptivo, (mecânico, térmico ou químico) Nociceptores Aδ, C Dor “normal” Diminuida Hipostesia táctil Nociceptores Aδ, C Hipoalgesia mecânica, ao calor ou frio Aumentada alodínia Hiperalgesia mecânica, ao calor ou frio Adaptado de: Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed ;
 Nociceptores Aδ, C. Dor normal Diminuida. Hipostesia táctil. Nociceptores Aδ, C. Hipoalgesia mecânica, ao calor ou frio. Aumentada. alodínia. Hiperalgesia mecânica, ao calor ou frio. Adaptado de: Wall PD, Melzack R (Eds). Textbook of Pain. 4th Ed ;")
22
Dor Nociceptiva Dor neuropática
The co-existence of pain types has been referred to as “mixed” or “combined” pain. Examples of these conditions include low back pain with associated lumbar radiculopathy, cancer pain and carpal tunnel syndrome.

23
Dor Nociceptiva Dor Mista Dor neuropática
The co-existence of pain types has been referred to as “mixed” or “combined” pain. Examples of these conditions include low back pain with associated lumbar radiculopathy, cancer pain and carpal tunnel syndrome.

24
Dor mista ou combinada A coexistência dos dois tipos de dor tem sido referida como estado de dor “mista” ou “combinada” e pode surgir em múltiplas situações, tais como síndrome do canal cárpico, dor lombar associada a radiculopatia e dor neoplásica O seu tratamento efectivo requer uma abordagem terapêutica abrangente, para aliviar as componentes nociceptiva e neuropática da dor Note to speaker: this slide contains an animated build. The first bullet appears automatically, then click on the slide to bring up the remaining 3 bullets sequentially.

25
Exemplo de dor mista: hérnia discal com radiculopatia
Activação dos nociceptores periféricos –componente nociceptiva da dor Compressão e inflamação da raíz nervosa –componente neuropática da dor Note to speaker: this slide contains an animated build to represent co-presenting pain (herniated disc causing low back pain and lumbar radiculopathy). Clicking on this slide causes subsequent components of the build to appear automatically. Nociceptive pain component: Localized, low back pain at the site of the herniated disc is mediated by the release of inflammatory mediators from degrading cartilage cells, activating peripheral nociceptors and sending impulses along the sensory (afferent) nerves to the dorsal horn and then to the brain. Neuropathic pain component: Pain impulses are mediated by nerve damage following compression of the dorsal root and abnormal impulses enter the spinal cord to reach the dorsal horn. These abnormal impulses can over-stimulate the secondary nerves ascending to the cortex through various pathways relaying in the brain stem, thalamus and limbic system where pain awareness develops. Such nerve damage (a lesion or dysfunction at any point of the ascending or descending pathways) can cause: Positive symptoms – spontaneous pain and tingling, radiating down to the lower legs. Negative symptoms – weakness or loss of sensation and numbness, radiating down to the lower legs. Broader analgesic treatment options may be required for the management of co-exisitng pain conditions to encompass both nociceptive and neuropathic elements.
. Clicking on this slide causes subsequent components of the build to appear automatically. Nociceptive pain component: Localized, low back pain at the site of the herniated disc is mediated by the release of inflammatory mediators from degrading cartilage cells, activating peripheral nociceptors and sending impulses along the sensory (afferent) nerves to the dorsal horn and then to the brain. Neuropathic pain component: Pain impulses are mediated by nerve damage following compression of the dorsal root and abnormal impulses enter the spinal cord to reach the dorsal horn. These abnormal impulses can over-stimulate the secondary nerves ascending to the cortex through various pathways relaying in the brain stem, thalamus and limbic system where pain awareness develops. Such nerve damage (a lesion or dysfunction at any point of the ascending or descending pathways) can cause: Positive symptoms – spontaneous pain and tingling, radiating down to the lower legs. Negative symptoms – weakness or loss of sensation and numbness, radiating down to the lower legs. Broader analgesic treatment options may be required for the management of co-exisitng pain conditions to encompass both nociceptive and neuropathic elements.")
26
Dor não localizada: referida ou radicular?
Em geral, a dor nociceptiva é localizada; porém, quando a lesão ocorre em estruturas profundas, a dor pode ser referida A dor referida é uma dor nociceptiva descrita pelos doentes como: dor “aborrecida”, “latejante” ou “moinha” A dor radicular é uma dor neuropática descrita pelos doentes como “descarga”, “choque eléctrico” ou “queimadura” e muitas vezes associada a “formigueiro” e “dormência” Referred pain: Although usually localized, when injury occurs to deep structures, nociceptive pain may be referred (e.g. gall bladder → shoulder pain, kidney stones → groin pain, myocardial infarction → arm pain) Referred pain is the consequence of the convergence of input from different areas of the body to the same spinal cord neurons. Radicular pain: Radicular pain is felt within the innervation territory of the affected root. Radicular pain can be accompanied by tingling and numbness, muscle weakness and loss of specific reflexes, and is caused by direct compression and/or injury to a spinal nerve root.
 Referred pain is the consequence of the convergence of input from different areas of the body to the same spinal cord neurons. Radicular pain: Radicular pain is felt within the innervation territory of the affected root. Radicular pain can be accompanied by tingling and numbness, muscle weakness and loss of specific reflexes, and is caused by direct compression and/or injury to a spinal nerve root.")
27
Abordagem “dos 3L” no diagnóstico diferencial
Os descritores verbais são sugestivos de DNe? Sim Não Provável dor nociceptiva Detecta alterações sensoriais com os ‘testes de cabeceira’? Sim Não Identificar a lesão/ disfunção do sistema nervoso responsável Considerar tratamento Considerar envio a consulta de referência Sim Não Confirmação do diagnóstico iniciar tratamento para dor neuropática MODIFICADO EM RELAÇÃO AO SLIDE PARA MF’S Note to speaker: this slide contains an animated build. Click on the slide to bring up each element of the build sequentially. Confirming the presence of neuropathic pain using the 3L approach: Identification of a cluster of common verbal descriptors should lead to the suspicion of neuropathic pain. Finding sensory abnormalities (either a deficit, such as hypoesthesia, or an excess of function such as hyperalgesia) in the painful area adds support for a neuropathic origin of the pain, particularly if the pain and the sensory abnormality are within a neuroanatomical territory. • Once neuropathic pain is suspected, the responsible neurological lesion/dysfunction must be identified. Occasionally sensory abnormalities may not be detected and/or the nervous system lesion/dysfunction cannot be easily identified. If neuropathic pain is still suspected, specialist referral should be considered (and appropriate pain treatment initiated in the interim period). Once neuropathic pain diagnosis is confirmed, consider initiating appropriate therapy.
 in the painful area adds support for a neuropathic origin of the pain, particularly if the pain and the sensory abnormality are within a neuroanatomical territory. • Once neuropathic pain is suspected, the responsible neurological lesion/dysfunction must be identified. Occasionally sensory abnormalities may not be detected and/or the nervous system lesion/dysfunction cannot be easily identified. If neuropathic pain is still suspected, specialist referral should be considered (and appropriate pain treatment initiated in the interim period). Once neuropathic pain diagnosis is confirmed, consider initiating appropriate therapy.")
28
Referenciação da Dor Neuropática (Finnerup et al., 2007)
Complexidade Baixa Moderada Elevada M.G.F. M.G.F. M.G.F. C.Dor M.F.R. C.Dor Ort. Neur. M.F.R. Psiq. Ort. Não inclui nevralgia do trigémio (deve usar-se Carbamazepina) Psiq. Neur.
 Psiq. Neur.")
29
Direcção Geral da Saúde Circular Normativa nº 9, de 14 de Junho de 2003
Registo sistemático da intensidade da dor Utilização para registo de escalas validadas

30
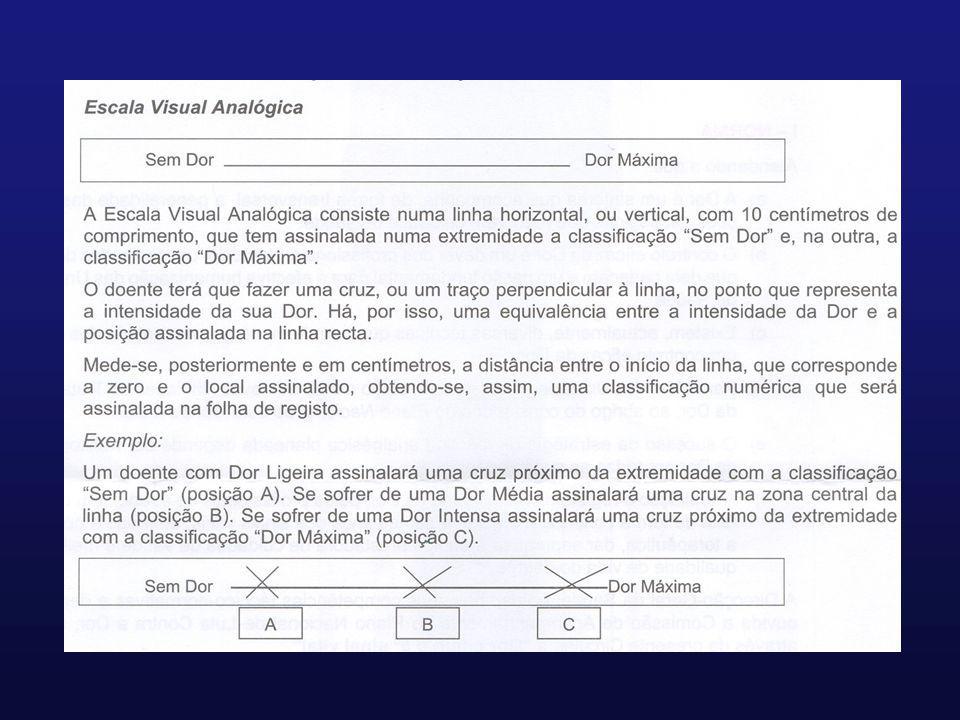
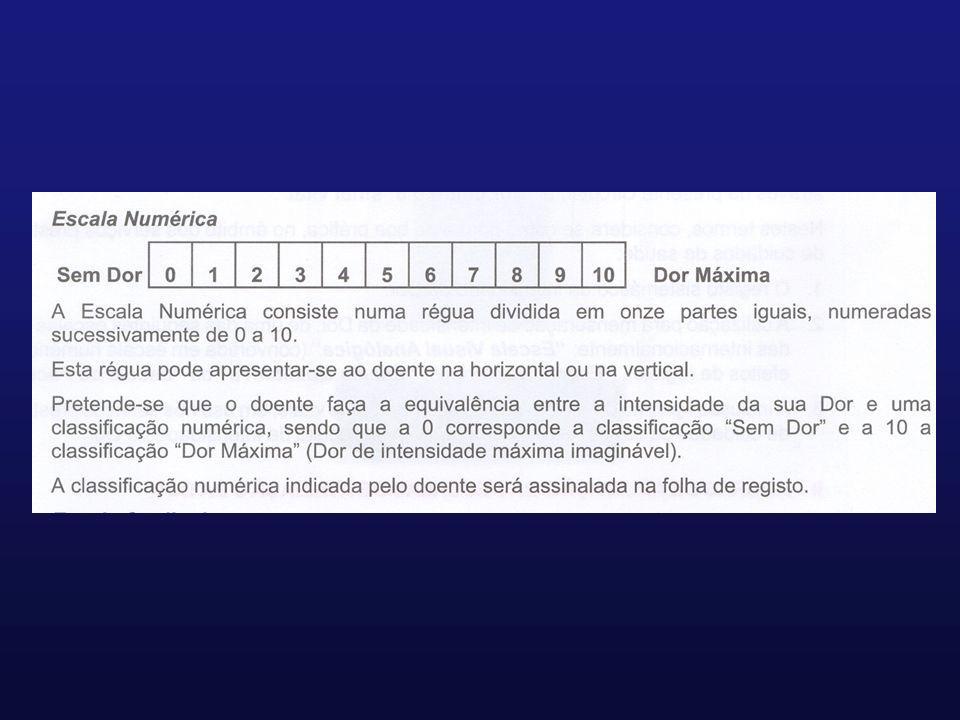
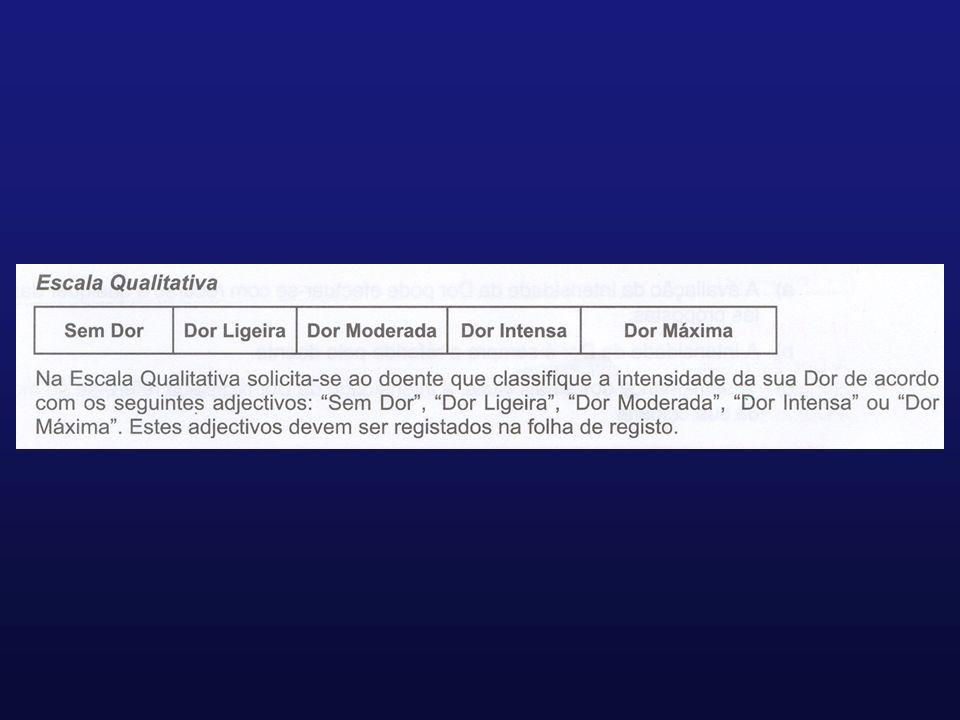
Escalas de intensidade da dor
Escala visual analógica Escala numérica Escala qualitativa Escala de faces

35
Avaliação clínica da dor
Intensidade Distribuição Qualidade Limiar de tolerância Comportamento Evolução temporal Sono Fadiga “Stress” Suporte social

36
Analgesia em Medicina Física e de Reabilitação
Tratamento Farmacológico Agentes Físicos Massagem Cinesiterapia Hidroterapia/Balneoterapia

37
Analgesia em Medicina Física e de Reabilitação
Intervenção em casos seleccionados Hierarquização do acesso ao tratamento Monitorização dos resultados

38
Analgesia em Medicina Física e de Reabilitação
Contribuir para o alívio da dor e evitar a deterioração funcional

39
Analgesia em Medicina Física e de Reabilitação
Contribuir para o alívio da dor e evitar a deterioração funcional Nunca esquecer que...

40
“...dor é quando o doente diz que dói !”

Apresentações semelhantes








, associada a reacção emocional (mal-estar,>")


, e que pode levar a incapacitação funcional.>")








