Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Aumento da excreção água e sódio à custa do espaço extracelular
DIURÉTICO Aumento da excreção água e sódio à custa do espaço extracelular

2
Mecanismos de contrarregulação
Elevação da PA Key Message: VPIs enhance levels of vasodilatory peptides and inhibit production of the vasoconstrictor Ang II, thereby restoring CV balance. Traditionally, the therapeutic approach to hypertension management has been to inhibit vasoconstriction or produce vasodilation. Increasingly, studies on hypertension show that BP regulation is a balance of endogenous vasodilators and vasoconstrictors. VPIs simultaneously augment the action of endogenous vasodilatory peptides and inhibit the production of the vasoconstrictor Ang II. This new approach favorably corrects the imbalance of CV vasoactive peptides in hypertension, resulting in greater BP reduction than other therapeutic approaches. Mecanismos compensadores Redução da PA

3
Equilíbrio sistemas neuro-humorais reguladores perfusão
Vasodilatores Natriuréticos Anti-proliferativos Anti-inflamatórios Antitrombogénicos Vasoconstritores Anti-natriuréticos Pró-proliferativos Pró-inflamatórios Trombogénicos Key Message: VPIs enhance levels of vasodilatory peptides and inhibit production of the vasoconstrictor Ang II, thereby restoring CV balance. Traditionally, the therapeutic approach to hypertension management has been to inhibit vasoconstriction or produce vasodilation. Increasingly, studies on hypertension show that BP regulation is a balance of endogenous vasodilators and vasoconstrictors. VPIs simultaneously augment the action of endogenous vasodilatory peptides and inhibit the production of the vasoconstrictor Ang II. This new approach favorably corrects the imbalance of CV vasoactive peptides in hypertension, resulting in greater BP reduction than other therapeutic approaches. Angiotensina 2 Aldosterona Adrenalina Noradrenalina Endotelina VSP TBX A2 Ubaína Dopamina ANF, BNF, CNF Adrenomedulina Prostaciclina Bradicinina NO

4
> Glomerular pressure e FF > Albumin excretion rate
Glomerulus Bowman’s capsule Afferent arteriole ACE inhibitors provide beneficial effects on renal function in diabetic renal disease, likely attributable to favorable systemic and renal hemodynamic changes. ACE inhibitors blunt the intrarenal arteriolar effects of angiotensin II, leading to dilation of efferent arterioles and reduction in glomerular capillary pressure and attendant glomerular hypertension. Furthermore, these agents reduce glomerular permeability, leading to lower urinary albumin excretion (Valentino et al, 1991). Efferent arteriole > Glomerular pressure e FF > Albumin excretion rate Valentino VA et al. Arch Intern Med 1991;151:
. Efferent. arteriole. > Glomerular pressure e FF. > Albumin excretion rate. Valentino VA et al. Arch Intern Med 1991;151:")
5
BP Glomerulus Bowman’s capsule Afferent arteriole Efferent arteriole
ACE inhibitors provide beneficial effects on renal function in diabetic renal disease, likely attributable to favorable systemic and renal hemodynamic changes. ACE inhibitors blunt the intrarenal arteriolar effects of angiotensin II, leading to dilation of efferent arterioles and reduction in glomerular capillary pressure and attendant glomerular hypertension. Furthermore, these agents reduce glomerular permeability, leading to lower urinary albumin excretion (Valentino et al, 1991). Efferent arteriole AII > Glomerular pressure e FF Valentino VA et al. Arch Intern Med 1991;151:
. Efferent. arteriole. AII. > Glomerular pressure e FF. Valentino VA et al. Arch Intern Med 1991;151:")
6
DIURÉTICO 1- Acção não directa no rim 2. Acção sobre mecanismos de transporte iónico a nível renal

7
DIURÉTICO 1- Acção não directa no rim MANITOL a) administração endovenosa b) totalmente filtrado no glomérulo c) hipervolemia transitória
 administração endovenosa b) totalmente filtrado no glomérulo c) hipervolemia transitória.")
8
DIURÉTICO 2. Acção sobre mecanismos de transporte iónico a nível renal Tiazidas e homólogos Indapamida Diuréticos da ansa (furosemida, ácido etacrínico Metolazona Diuréticos poupadores de potássio Inibidores da anídrase carbónica Antagonistas da ADH

9
DIURÉTICOs Na+ K+ 2 Cl- Na+ H+ Na+ K+

10
Diuréticos

11
DIURÉTICOs Na+ K+ 2 Cl- Na+ H+ ALDOSTERONA Na+ K+

12
DIURÉTICOs Hiponatremia Na+ Hipocalemia Hipocloremia K+ Cl+ Na+ K+

13
Diuréticos

14
Diuréticos

15
DIURÉTICOs Hiponatremia Na+ Hipocalemia Hipocloremia K+ Cl+ Alcalose

16
DIURÉTICOs TIAZIDAS D. ANSA Hiponatremia Na+ Hipocalemia Hipocloremia
K+ 2 Cl- K+ Cl+ Na+ H+ Alcalose H+ Hipocalemia Na+ K+ K+

17
Tiazidas e homólogos Diuréticos da ansa (furosemida, acido etacrínico)
D. ansa Tiazidas

18
DIURÉTICO Tiazidas e homólogos Diuréticos da ansa (furosemida, acido etacrínico) EFEITOS COMUNS Aumento dos níveis séricos de: glicose, ácido úrico, colesterol, triglicerídeos

19
DIURÉTICO Tiazidas e homólogos Diuréticos da ansa (furosemida, acido etacrínico) EFEITOS COMUNS Aumento dos níveis séricos de: Renina, glicose, ácido úrico, colesterol, triglicerídeos Aumento da excreção urinária de cálcio (Furosemida) i.e. maior risco de osteoporose. Redução da excreção urinária de cálcio (Tiazidas) i.e. menor risco de osteoporose.
 i.e. maior risco de osteoporose. Redução da excreção urinária de cálcio (Tiazidas) i.e. menor risco de osteoporose.")
20
DIURÉTICOs Ansa de Henle Na+ Na+ K+ 2 Cl- K+ + K+ Mg+, Ca2+

21
DIURÉTICOs Tubo distal Na+ Na+ Cl- K+ PHT K+ Ca2+ Ca2+ Na+

22
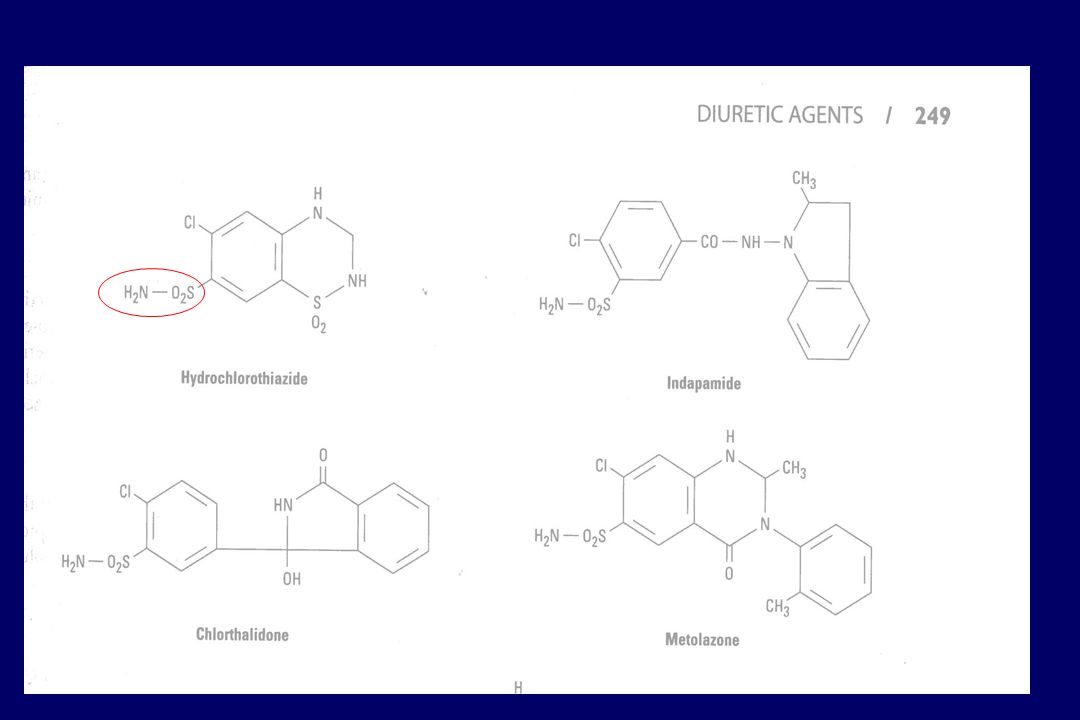
Tiazidas e homólogos (clorotalidona –tb sulfonamidico)
DIURÉTICO Tiazidas e homólogos (clorotalidona –tb sulfonamidico) FARMACO Clorotalidona Hidroclorotiazida Clorotiazida Politiazida DURAÇÂO DA ACÇÂO 48-72 h 6-12 h 24-48h
 FARMACO. Clorotalidona. Hidroclorotiazida. Clorotiazida. Politiazida. DURAÇÂO DA ACÇÂO h h h.")
24
DIURETICOS 1.< competição com excrecção tubular de ácido úrico
» < hiperuricemia 2. Eficácia mesmo se TFG < 40 ml/min 3. Menor risco de hiperglicemia e de aumento do CT/TG

25
Tiazidas e homólogos (clorotalidona –tb sulfonamidico)
DIURÉTICO Tiazidas e homólogos (clorotalidona –tb sulfonamidico) INDICAÇÕES CLÍNICAS ESTADOS EDEMATOSOS GENERALIZADOS HIPERTENSÃO ARTERIAL INSUFICIÊNCIA CARDÍACA Nefrolitiase por hipercalciúria ideopatica Diabetes insipida nefrogénica
 INDICAÇÕES CLÍNICAS. ESTADOS EDEMATOSOS GENERALIZADOS. HIPERTENSÃO ARTERIAL. INSUFICIÊNCIA CARDÍACA. Nefrolitiase por hipercalciúria ideopatica. Diabetes insipida nefrogénica.")
26
DIURÉTICO Indapamida Acção no tubulo distal Expoliação de potássio Menor interferencia na glicemia, lipidemia Possivel efeito antagonista cálcio Regressão HVE superior aos diureticos

27
TIAZIDAS MECANISMO DE ACÇÂO
Excreção % do Na+ Excreção de K Inhibição da anidrase carbonica: maior elimination de HCO3 Baixa relação dose-efeito Treatment of heart failure. Diuretics: Mechanism of action of the thiazides The thiazides are diuretics of intermediate potency, excreting 5-10% of the filtered fraction of Na. The act from the luminal surface inhibiting the active transport of Cl and the subsequent diffusion of Na and water in the cortical diluting segment of the ascending portion of the loop of Henle. The also increase elimination of K by increasing the exchange of Na/K in the distal convoluted tubule and increase the urinary elimination of HCO3 by inhibiting carbonic anhydrase. In addition they increase tubular reabsorption of uric acid, Ca and Mg. There are important differences in the strength and duration of diuretic action depending on which thiazide is used.

28
LOOP DIURETICS MECHANISM OF ACTION
Excreção de % do Na+ filtrado Eliminação de K+, Ca+ e Mg++ Resistência das arteriolas aferentes Fluxo cortical e GFR Libertação renal de PGs AINEs antagonizam diurese Treatment of heart failure. Diuretics Mechanism of action of loop diuretics Loop diuretics are the strongest, prompting the excretion of 15-20% of the filtered Na+. They act in the thick segment of the ascending loop of Henle, inhibiting the cotransport of Cl--Na+-K+ at the luminal surface. They also increase the elimination of K+, as the increase in Na that reaches the distal convoluted tubule stimulates its exchange for K+ and H+; in addition, they also stimulate the secretion of renin and the production of aldosterone which augments the elimination of K+. By inhibiting carbonic anhydrase, they increase the urinary elimination of HCO-3. They also increase elimination of Ca++ and Mg++. GFR: glomerular filtration rate; PGS: prostaglandins; NSAIDs: nonsteroidal anti-inflammatory drugs.

29
DIURETICS ADVERSE REACTIONS Thiazide and Loop Diuretics
Alteração electrolitica: Volume Na+, K+, Mg++ alcalose metabólica Alteração metabólica glicemia, uremia, gota LDL-C and TG Reacções alérgicas cutâneas Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics Thiazide and loop diuretics create electrolyte imbalances: hypovolemia, hyponatremia, hypokalemia, hypomagnesemia, hypercalcemia and metabolic alkalosis. They also create metabolic changes (hyperglycemia, hyperuricemia, gout, increase in LDL-cholesterol and triglycerides), impotence and menstrual cramps. Hypokalemia can be treated with K+ supplements or with the simultaneous use of potassium-sparing diuretics. Cutaneous allergic reactions (rash, pruritis) are frequent. In addition, these are cross-reactions between the various thiazides (except chlorthalidone) and because of their chemical resemblance, with furosemide and bumetanide. Thiazides can aggravate myopia in pregnant women.
, impotence and menstrual cramps. Hypokalemia can be treated with K+ supplements or with the simultaneous use of potassium-sparing diuretics. Cutaneous allergic reactions (rash, pruritis) are frequent. In addition, these are cross-reactions between the various thiazides (except chlorthalidone) and because of their chemical resemblance, with furosemide and bumetanide. Thiazides can aggravate myopia in pregnant women.")
30
DIURETICS ADVERSE REACTIONS Thiazide and Loop Diuretics
Idiosyncratic effects: Blood dyscrasia, cholestatic jaundice and acute pancreatitis Gastrointestinal effects Genitourinary effects: Impotence and menstrual cramps Deafness, nephrotoxicity (Loop diuretics) Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics Known adverse reactions include parenchymal (pancreatitis, cholestatic jaundice, hemolytic anemia, thrombocytopenia), gastrointestinal effects (ethacrynic acid), myalgias (bumetanide, piretanide) and muscle cramps related to electrolyte disorders. Loop diuretics are associated with ototoxicity with loss of hearing and balance and these are more frequent in patients with renal insufficiency or with concomitant use of aminoglycoside antibiotics. They may also cause interstitial nephritis.
 Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics. Known adverse reactions include parenchymal (pancreatitis, cholestatic jaundice, hemolytic anemia, thrombocytopenia), gastrointestinal effects (ethacrynic acid), myalgias (bumetanide, piretanide) and muscle cramps related to electrolyte disorders. Loop diuretics are associated with ototoxicity with loss of hearing and balance and these are more frequent in patients with renal insufficiency or with concomitant use of aminoglycoside antibiotics. They may also cause interstitial nephritis.")
31
DIURÉTICO Tiazidas e homólogos Diuréticos da ansa (furosemida, acido etacrínico) EFEITOS COMUNS Tiazidas: atenuação da acção perante “clearances baixos da creatinina

32
DIURÉTICOs Na+ K+ 2 Cl- Na+ Na+ H+ Acidose H+ Urina alcalina Na+ K+

33
DIURÉTICO Inibidores da anídrase carbónica (Acetazolamida Metazolamida Diclorofenamida)
")
34
Inibidores da anídrase carbónica (acetazolamida)
DIURÉTICO Inibidores da anídrase carbónica (acetazolamida) H2O + CO2 H2CO3 H HCO3- Anídrase carbónica
 H2O + CO2. H2CO3. H+ HCO3- Anídrase carbónica.")
35
Inibidores da anídrase carbónica (acetazolamida)
DIURÉTICO Inibidores da anídrase carbónica (acetazolamida) H2O + CO2 H2CO3 H HCO3- Anídrase carbónica
 H2O + CO2. H2CO3. H+ HCO3- Anídrase carbónica.")
36
DIURÉTICOs Hipercloremia Na+ Acidose Na+ K+ 2 Cl- Cl- Na+ H+
Urina alcalina Na+ K+

37
DIURÉTICOs Na+ K+ 2 Cl- Na+ H+ Na+ K+ Hipercalemia K+

38
DIURÉTICO Poupadores de potássio 1. Espironolactona eplerenona 2. Amilorido e triantereno

39
Diuréticos

40
K-SPARING DIURETICS MECHANISM OF ACTION
Eliminate < 5% of filtered Na+ Inhibit exchange of Na+ for K+ or H+ Spironolactone = competitive antagonist for the aldosterone receptor Amiloride and triamterene block Na+ channels controlled by aldosterone Treatment of heart failure. Diuretics: Mechanism of action of potassium-sparing diuretics Potassium-sparing diuretics inhibit reabsorption of Na+ at the level of the distal convoluted tubule and the collecting duct and its exchange for K+ or H+. Their diuretic strength is slight, as the fraction of Na eliminated is no more than 5%. Spironolactone is a competitive antagonist of aldosterone, interfering with its induction of synthesis of proteins which specifically facilitate Na reabsorption. As a result, its diuretic action depends on the role that aldosterone plays in the retention of water and Na. Triamterene and amiloride block the exchange of Na+-K+/H+, but their effect is independent of the levels of aldosterone. All of these drugs moderately increase the renal excretion of Na+, Cl- and HCO-3, at the same time that they diminish the excretion of K+, H +and ammonium, and may therefore cause hyperkalemia and hypochloremic acidosis.

41
ALDOSTERONE INHIBITORS
Spironolactone ALDOSTERONE Competitive antagonist of the aldosterone receptor (myocardium, arterial walls, kidney) Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Retention Na+ Retention H2O Excretion K+ Excretion Mg2+ Collagen deposition Fibrosis - myocardium - vessels Edema Arrhythmias
 Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action. Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Retention Na+ Retention H2O. Excretion K+ Excretion Mg2+ Collagen. deposition. Fibrosis. - myocardium. - vessels. Edema. Arrhythmias.")
42
DIURÉTICO Poupadores de potássio 1. Espironolactona (ginecomastia) eplerenona 2. Amilorido e triantereno (alter. auditivas)
 .")
43
• Severe renal insufficiency • Metabolic acidosis
ALDOSTERONE INHIBITORS CONTRAINDICATIONS • Hyperkalemia • Severe renal insufficiency • Metabolic acidosis Treatment of congestive heart failure. Aldosterone inhibitors: Contraindications The contraindications for spironolactone use include hyperkalemia and chronic renal insufficiency.

44
Diuréticos

45
DIURETICS Cortex Medulla Thiazides K-sparing Loop diuretics
Inhibit active exchange of Cl-Na in the cortical diluting segment of the ascending loop of Henle Cortex K-sparing Inhibit reabsorption of Na in the distal convoluted and collecting tubule Treatment of heart failure. Diuretics: Classification and mechanisms of action Diuretics are drugs which eliminate Na and water by acting directly on the kidney. This category does not include other drugs with principle actions different from the diuretics, but which increase diuresis by improving heart failure or by mechanisms on the kidney which are incompletely understood. The diuretics are the primary line of therapy for the majority of patients with heart failure and pulmonary congestion. Diuretics (loop, thiazides and potassium-sparing) produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Loop diuretics Inhibit exchange of Cl-Na-K in the thick segment of the ascending loop of Henle Medulla Loop of Henle Collecting tubule
 produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Loop diuretics. Inhibit exchange of Cl-Na-K in. the thick segment of the ascending. loop of Henle. Medulla. Loop of Henle. Collecting tubule.")
46
DIURÉTICO USO 1. Estados edematosos (insuficiência renal, cardíaca, hepática) 2. Hipertensão
 2. Hipertensão")
Apresentações semelhantes




>")









>")
>")



