Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Caso Clínico Leticia Kawano Dourado
Grupo de Doenças Intersticiais Pulmonares Divisão de Pneumologia - InCor Faculdade de Medicina da Universidade de São Paulo

2
História Clínica 56 anos, sexo masculino, pedreiro
Consulta rotina Medicina do Trabalho: Nódulo em radiografia de tórax PPD 15mm 3 pesquisas BAAR escarro: negativas Tabagista 60 a.m.

3
História Clínica Queixas:
Artralgia punhos, joelhos e tornozelos há 1 ano (padrão mecânico??) Hiperemia e dor ocular bilateral há 2 meses
 Hiperemia e dor ocular bilateral há 2 meses.")
4
Exame Físico Bom estado geral Olhos vermelhos e dolorosos
56a, masculino TBG 60am, PPD 15 Nódulo pulmonar Poliartralgias (?) Exame Físico Bom estado geral Olhos vermelhos e dolorosos Edema de membro superior D SpO2 97% Ausência de alterações pulmonares
 Exame Físico. Bom estado geral. Olhos vermelhos e dolorosos. Edema de membro superior D. SpO2 97% Ausência de alterações pulmonares.")
5
História Clínica Aval Oftalmo: Esclerite nodular bilateral
56a, masculino TBG 60am, PPD 15 Nódulo pulmonar Poliartralgias (?) História Clínica Aval Oftalmo: Esclerite nodular bilateral Doppler MSD: Trombose venosa profunda
 História Clínica. Aval Oftalmo: Esclerite nodular bilateral. Doppler MSD: Trombose venosa profunda.")
6
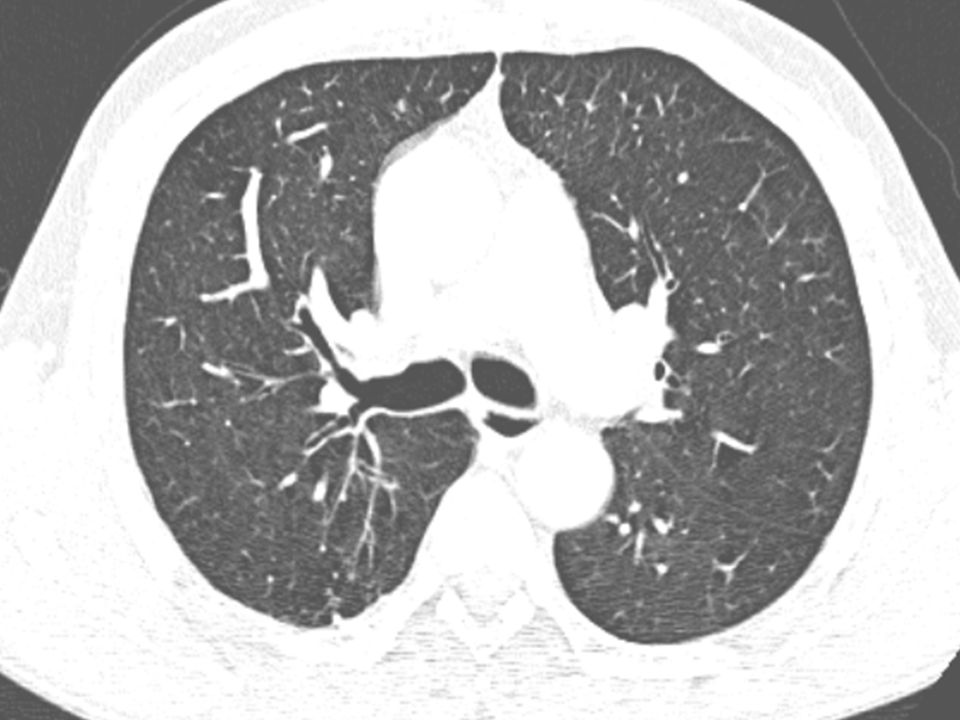
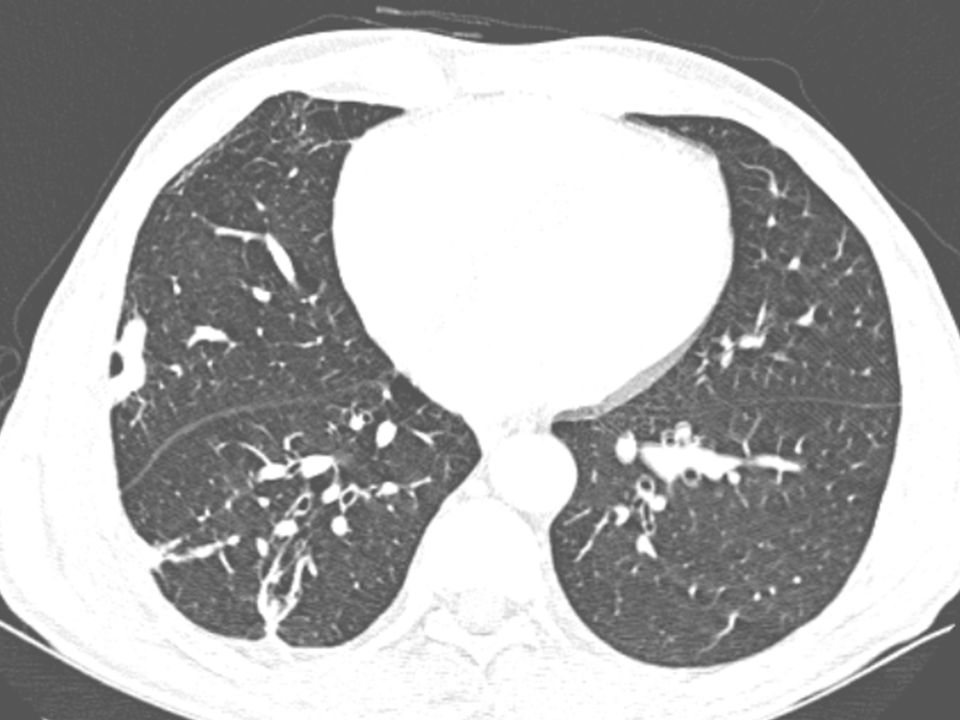
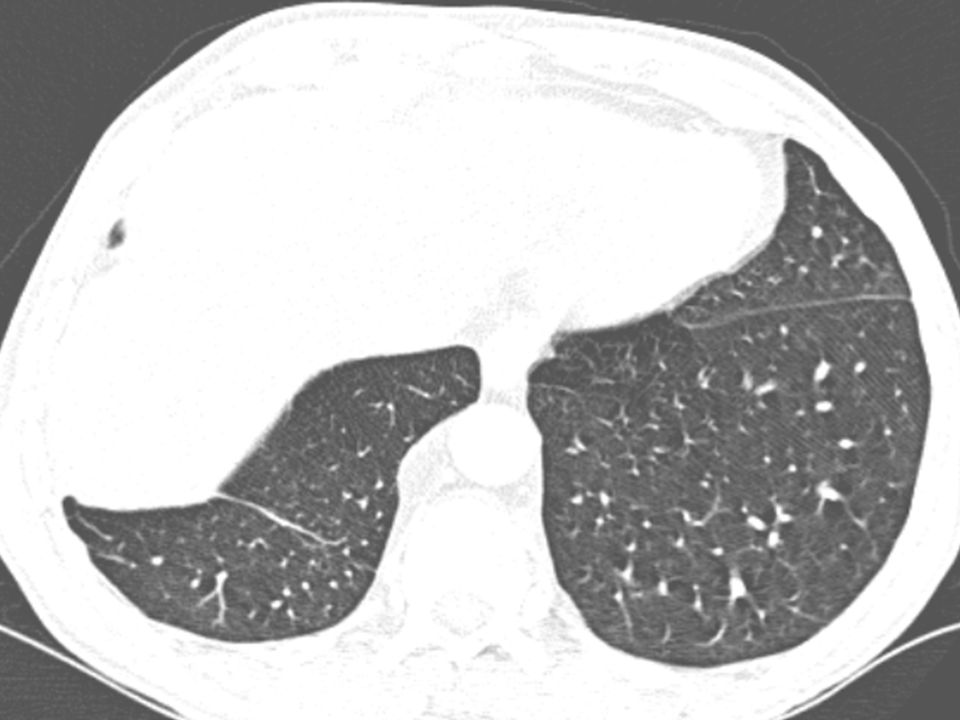
Tomografia de Tórax

16
Hipóteses Diagnósticas e Conduta

17
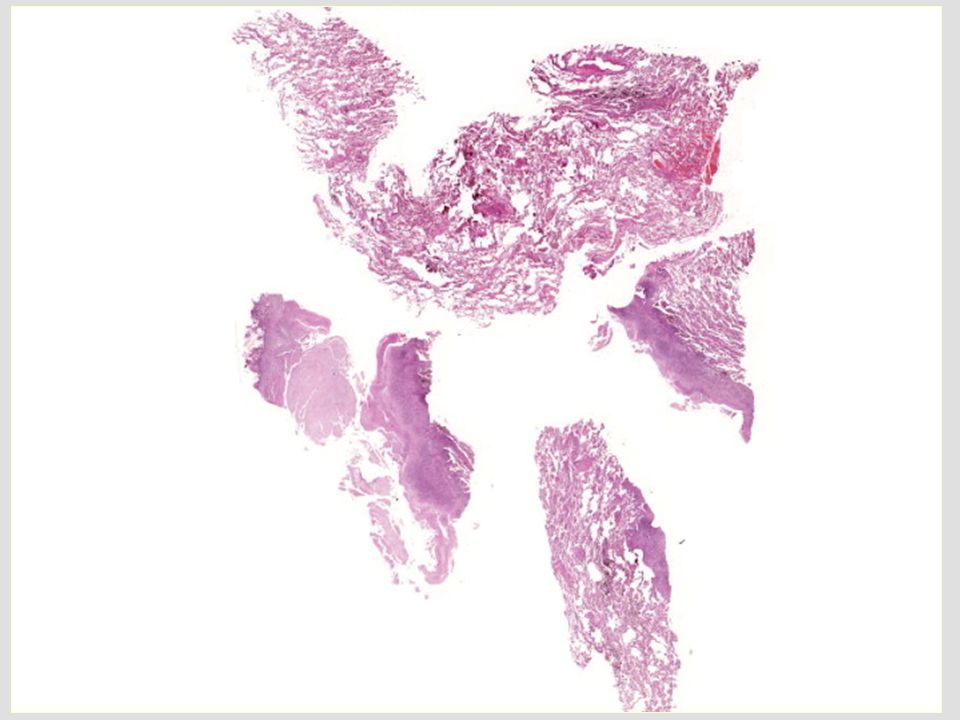
Biópsia cirúrgica nódulo LID
Revisão externa

24
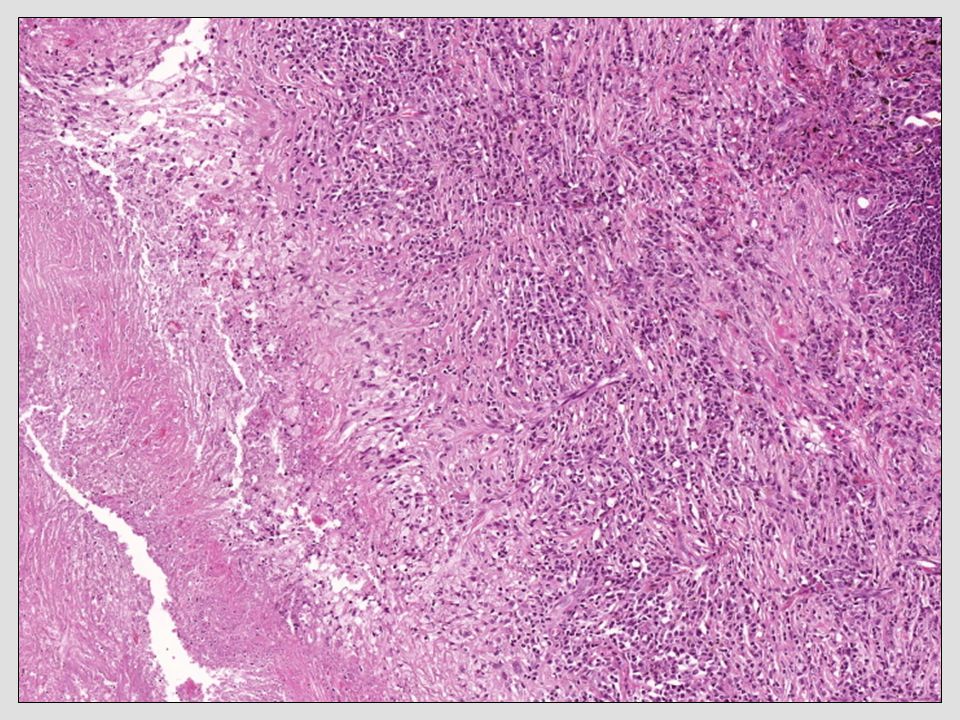
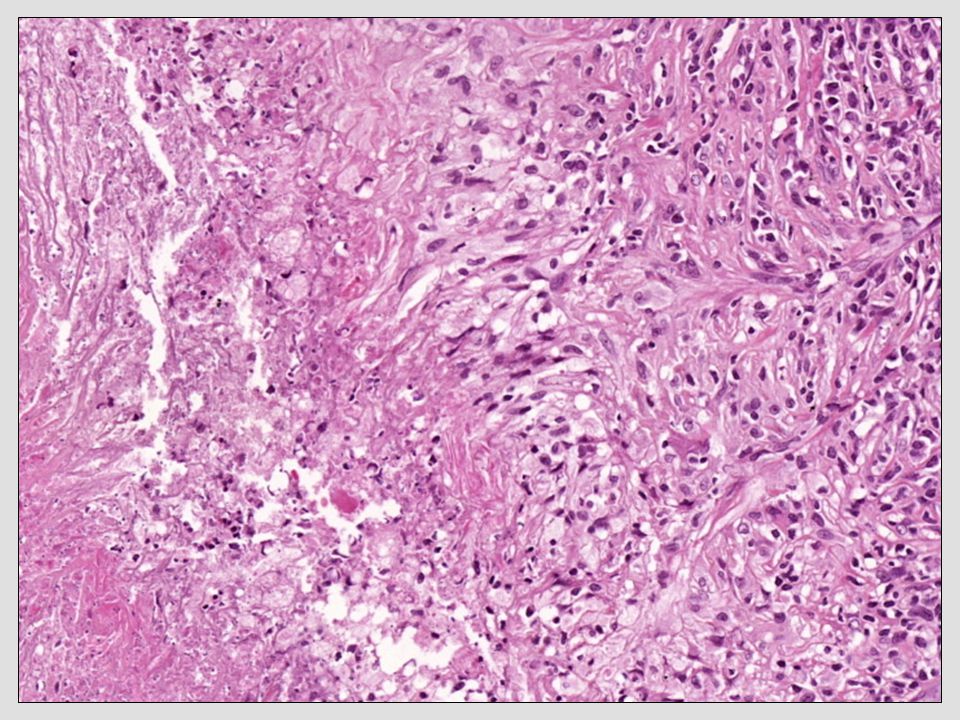
Processo inflamatório crônico granulomatoso necrotizante não-caseoso
Ausência de sinais de vasculite Possibilidades diagnósticas: . Infeccioso – pesquisas negativas . Nódulo reumatóide . Granulomatose de Wegener

25
Sorologia para fungos negativa HIV negativo
56a, masculino TBG 60am, PPD 15 Nódulo (granuloma) Poliartralgias (?) Esclerite nodular TVP MSD Sorologia para fungos negativa HIV negativo
 Poliartralgias ( ) Esclerite nodular. TVP MSD. Sorologia para fungos negativa. HIV negativo.")
26
Prova terapêutica com esquema RIP?
Adequado ou não?

27
Nota Pcte vinha encaminhado de outro serviço:
Uso de esquema RIP há 2 meses HD: TB ocular/pulmonar sem melhora sintomas oculares surgimento de novo nódulo pulmonar

28
FAN 1/80 (nuclear pont fino) FR: 312 anti-CCP 125 c-ANCA: 1/20
56a, masculino TBG 60am Nódulo (granuloma) Poliartralgias (?) Esclerite nodular TVP MSD Ur e Crea normais Urina 1: normal VHS 36 mm PCR 18 mg/L Hb 15 g/dL Ht 46% Leuc: 8.400/mm3 FAN 1/80 (nuclear pont fino) FR: anti-CCP c-ANCA: 1/20
 Poliartralgias ( ) Esclerite nodular. TVP MSD. Ur e Crea normais. Urina 1: normal. VHS 36 mm PCR 18 mg/L. Hb 15 g/dL Ht 46% Leuc: 8.400/mm3. FAN 1/80 (nuclear pont fino) FR: 312 anti-CCP 125 c-ANCA: 1/20.")
29
?
30
Fio de Ariadne Na mitologia grega, o labirinto de Creta teria sido construído por Dédalo (arquitecto cujo nome tornou-se, depois, também sinônimo de labirinto) para alojar o Minotauro, monstro metade homem, metade touro, a quem eram oferecidos regularmente jovens que devorava. Segundo a lenda, Teseu conseguiu derrotá-lo e encontrar o caminho de volta do labirinto graças ao fio de um novelo, dado por Ariadne, que foi desenrolando ao longo do percurso. O Fio de Ariadne, assim chamado devido a lenda de Ariadne, é o termo usado para descrever a resolução de um problema que se pode proceder de diversas maneiras óbvias (como exemplo: um labirinto físico, um quebra-cabeça de lógica ou um dilema ético), através de uma aplicação exaustiva da lógica por todos os meios disponíveis. É o método singular utilizado que permite seguir completamente pelo vestígios das pistas ou assimilar gradativo e seguidamente uma série de verdades encontradas em um evento inesperado, ordenando a pesquisa, até que atinja um ponto de vista final desejado. Este processo pode assumir o método de um registro mental, uma marcação física ou mesmo um debate filosófico.
 para alojar o Minotauro, monstro metade homem, metade touro, a quem eram oferecidos regularmente jovens que devorava. Segundo a lenda, Teseu conseguiu derrotá-lo e encontrar o caminho de volta do labirinto graças ao fio de um novelo, dado por Ariadne, que foi desenrolando ao longo do percurso. O Fio de Ariadne, assim chamado devido a lenda de Ariadne, é o termo usado para descrever a resolução de um problema que se pode proceder de diversas maneiras óbvias (como exemplo: um labirinto físico, um quebra-cabeça de lógica ou um dilema ético), através de uma aplicação exaustiva da lógica por todos os meios disponíveis. É o método singular utilizado que permite seguir completamente pelo vestígios das pistas ou assimilar gradativo e seguidamente uma série de verdades encontradas em um evento inesperado, ordenando a pesquisa, até que atinja um ponto de vista final desejado. Este processo pode assumir o método de um registro mental, uma marcação física ou mesmo um debate filosófico.")
31
Ausência de resposta ao esquema RIP Indícios de auto-imunidade
Fio de Ariadne Ausência de resposta ao esquema RIP + Indícios de auto-imunidade

32
Qual doença auto-imune?
Nódulos granulomatosos com necrose no pulmão Esclerite nodular bilateral FR 312: anti-CCP: 125 Poliartralgias TVP

33
Diagnóstico Diferencial

34
Doença Inflamatória intestinal
Nódulos necrobióticos: Histologia semelhante ao pioderma gangrenoso Netrofílico, vasculite linfocitária ANCA-p Esclerite associada Peeters, M et al. Am J Gastroenterol, 2001 Kasuga, I et al. Respir Med, 1997

35
LH: Incomum a ausência de linfadenomegalia mediastinal
No caso relatado: Linfadenomegalia cervical e mediastinal + esclerite

36
Les Demoiselles d'Avignon. Picasso, 1907

37
Granulomatose com Poliangeíte
(WEGENER) Artrite Reumatóide vs
 Artrite Reumatóide. vs.")
38
Granulomatose com poliangeíte
Granulomatose com poliangeíte (Wegener) – forma localizada Aspecto tomográfico e histologia compatíveis Esclerite ANCA-c 1/20 No entanto…
 – forma localizada. Aspecto tomográfico e histologia compatíveis. Esclerite. ANCA-c 1/20. No entanto…")
39
Anti-CCP não é descrito Wegener
22 pacientes com Granulomatose com poliangeíte (Wegener): 30% FR positivo 0% anti-CCP
: 30% FR positivo. 0% anti-CCP.")
40
Anti-CCP ~90% especificidade para Artrite Reumatóide Falsos positivos:
LES Sjogren Tuberculose ativa Deficiência de alfa-1-anti-tripsina DPOC Nishimura K et al. Ann Intern Med. 2007 Elkayam, O et al. Ann Rheum Dis, 2006 Fabien, N et al. Clin Rev Allergy Immunol, 2008

41
Esclerite 50% dos casos esclerite tem associação com doença sistêmica
Mais comum associação: Artrite Reumatóide Outras: Vasculites ANCA Doença Inflamatória Intestinal LES Policondrite recidivante Jabs, DA et al. Am J Ophthalmol, 2000

42
Qual o impacto em diferenciar Artrite Reumatóide da Granulomatose com Poliangeíte (Wegener)?
")
43
Determinada pela manifestação mais grave da doença!
Seleção do Tratamento? Determinada pela manifestação mais grave da doença! Esclerite nodular Denominador comum

44
Granulomatose com poliangeíte (Wegener)
Importância Granulomatose com poliangeíte (Wegener) Acometimento renal Colonização nasal por S. aureus mantém doença MTX opção casos mais leves ou em fase manutenção Artrite Reumatóide Raro acometimento renal Elevado risco de Osteoporose Acometimento hematológico MTX droga inicial de escolha
 Acometimento renal. Colonização nasal por S. aureus mantém doença. MTX opção casos mais leves ou em fase manutenção. Artrite Reumatóide. Raro acometimento renal. Elevado risco de Osteoporose. Acometimento hematológico. MTX droga inicial de escolha.")
45
Finalmente: um pouco sobre nódulos reumatóides no pulmão

46
Nódulo Reumatóide típico
Mais comum Artrite Reumatóide + sintomas clássicos articulares FR e anti-CCP em altos títulos Associação com nódulos subcutâneos Doença ativa Geralmente assintomáticos Complicações: Pneumotorax, derrame pleural, fístula broncopleural Turesson C et al. Curr Opin Rheumatol, 2013

47
Subpleurais Ambulatório de Doenças Intersticiais Pulmonares. HC-FMUSP

48
Podem cavitar Ambulatório de Doenças Intersticiais Pulmonares. HC-FMUSP

49
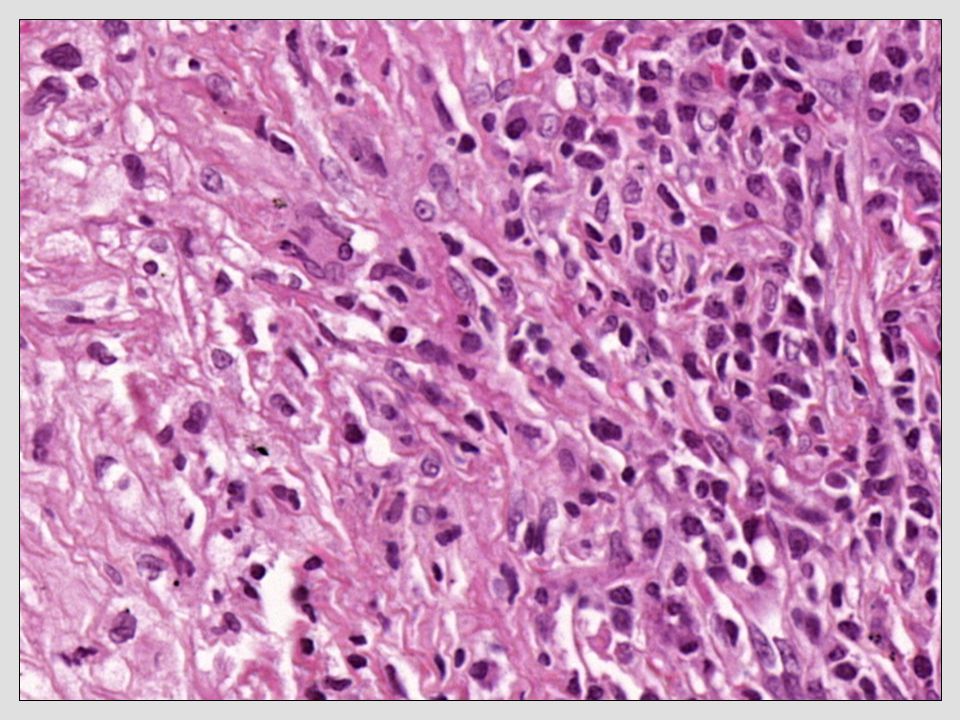
Histologia Clássica Não é patognomônica
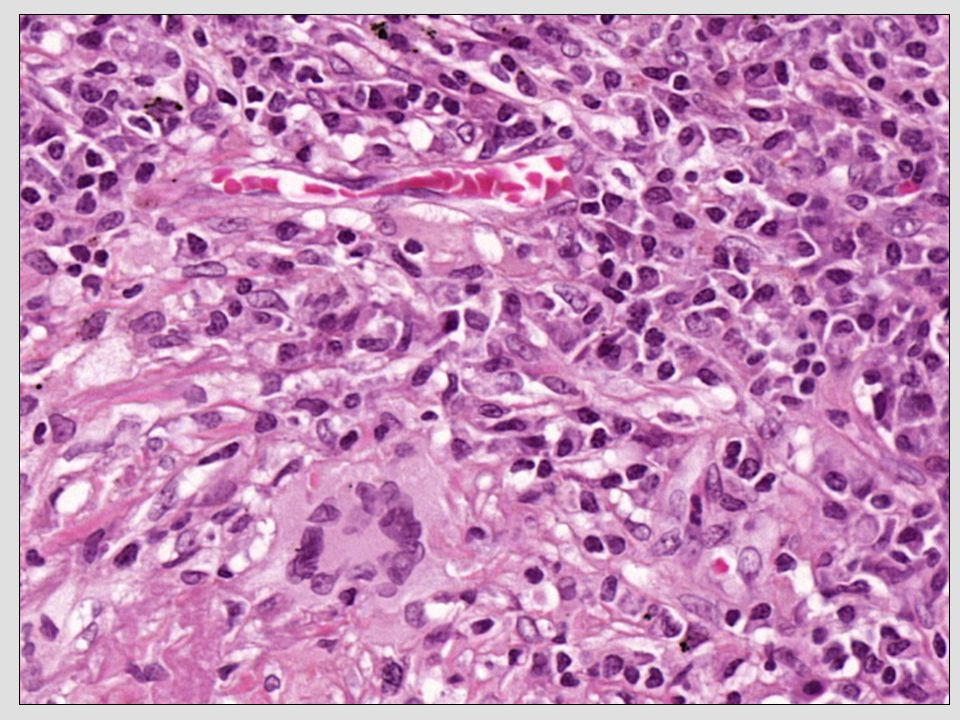
Nódulo com necrose central e paliçada de histiócitos, podendo conter células gigantes esparsas Vasculite (não necrotizante) Céls gigantes FIGURE Stages of pulmonary rheumatoid nodules. A. Pulmonary rheumatoid nodule with palisading histiocytes surrounding a central zone of necrobiosis. Early cavitation is evident (upper left). Reis-Filho, S et al. Diagnostic Cytopathology, 2001 Katzenstein, AL. Surgical Pathology of Non neoplastic Lung Disease, 2006
 Céls gigantes. FIGURE Stages of pulmonary rheumatoid nodules. A. Pulmonary. rheumatoid nodule with palisading histiocytes surrounding. a central zone of necrobiosis. Early cavitation is. evident (upper left). Reis-Filho, S et al. Diagnostic Cytopathology, Katzenstein, AL. Surgical Pathology of Non neoplastic Lung Disease,")
50
Evolução do caso

51
Evolução do Caso Iniciado Ciclofosfamida e CES: pela Esclerite
Anticoagulação para TVP Immunosuppressive medications — Immunosuppressive therapy in addition to glucocorticoids is generally given if: there is persistent inflammation after two to three weeks of treatment there is progression of disease to a more severe variant (eg, the evolution of diffuse anterior scleritis into the necrotizing subtype) There are no randomized trials in scleritis on which to base the choice of the specific immunosuppressive medication. However, because of the proven effectiveness of both rituximab and cyclophosphamide in patients with granulomatosis with polyangiitis (Wegener’s), the first-line immunosuppressive medication in the treatment of scleritis is typically one of these agents. (See "Initial immunosuppressive therapy in granulomatosis with polyangiitis (Wegener's) and microscopic polyangiitis".) Options other than rituximab or cyclophosphamide for patients with milder disease in need of a steroid-sparing agent include cyclosporine, mycophenolate mofetil, and methotrexate. Mycophenolate mofetil has primarily been studied as a steroid-sparing agent, with variable efficacy [4,5], and may also be used as maintenance therapy; methotrexate has been used in a similar fashion [6]. Rituximab — Two rituximab regimens are effective in the treatment of rheumatic conditions. Either of these rituximab regimens is an acceptable first-line approach for the treatment of patients with scleritis refractory to glucocorticoids alone. The administration of 1 gram of rituximab twice (with the two doses separated by approximately 15 days) is the regimen approved by the US FDA for the treatment of rheumatoid arthritis. In addition, the use of four 375 mg/m2 doses administered one week apart have been approved by the FDA for the treatment of ANCA-associated vasculitis. (See "Treatment of cyclophosphamide-resistant granulomatosis with polyangiitis (Wegener’s) and microscopic polyangiitis", section on 'Rituximab'.) Cyclophosphamide — For patients with disease refractory to rituximab, we suggest cyclophosphamide (2 mg/kg per day, with dose adjustments for patients with decreased renal function). We suggest initiating oral cyclophosphamide therapy at a dose of 2 mg/kg per day, with dose adjustments for patients with decreased renal function [7]. With the use of cyclophosphamide, the general approach is to establish disease control as quickly as possible through combination therapy with prednisone and then to discontinue cyclophosphamide after three to six months. Cyclophosphamide is replaced by a medication with a lower risk of toxicity, usually azathioprine or methotrexate. Cyclosporine — Cyclosporine has been used in place of cyclophosphamide in a small case series of patients with severe scleritis [8,9]. The typical dose ranges from 2 to 3 mg/kg per day in two divided doses. Maintenance therapy — Because of the toxicity of long-term cyclophosphamide therapy, a number of less toxic drugs have been used for maintenance thera
 There are no randomized trials in scleritis on which to base the choice of the specific immunosuppressive medication. However, because of the proven effectiveness of both rituximab and cyclophosphamide in patients with granulomatosis with polyangiitis (Wegener’s), the first-line immunosuppressive medication in the treatment of scleritis is typically one of these agents. (See Initial immunosuppressive therapy in granulomatosis with polyangiitis (Wegener s) and microscopic polyangiitis .) Options other than rituximab or cyclophosphamide for patients with milder disease in need of a steroid-sparing agent include cyclosporine, mycophenolate mofetil, and methotrexate. Mycophenolate mofetil has primarily been studied as a steroid-sparing agent, with variable efficacy [4,5], and may also be used as maintenance therapy; methotrexate has been used in a similar fashion [6]. Rituximab — Two rituximab regimens are effective in the treatment of rheumatic conditions. Either of these rituximab regimens is an acceptable first-line approach for the treatment of patients with scleritis refractory to glucocorticoids alone. The administration of 1 gram of rituximab twice (with the two doses separated by approximately 15 days) is the regimen approved by the US FDA for the treatment of rheumatoid arthritis. In addition, the use of four 375 mg/m2 doses administered one week apart have been approved by the FDA for the treatment of ANCA-associated vasculitis. (See Treatment of cyclophosphamide-resistant granulomatosis with polyangiitis (Wegener’s) and microscopic polyangiitis , section on Rituximab .) Cyclophosphamide — For patients with disease refractory to rituximab, we suggest cyclophosphamide (2 mg/kg per day, with dose adjustments for patients with decreased renal function). We suggest initiating oral cyclophosphamide therapy at a dose of 2 mg/kg per day, with dose adjustments for patients with decreased renal function [7]. With the use of cyclophosphamide, the general approach is to establish disease control as quickly as possible through combination therapy with prednisone and then to discontinue cyclophosphamide after three to six months. Cyclophosphamide is replaced by a medication with a lower risk of toxicity, usually azathioprine or methotrexate. Cyclosporine — Cyclosporine has been used in place of cyclophosphamide in a small case series of patients with severe scleritis [8,9]. The typical dose ranges from 2 to 3 mg/kg per day in two divided doses. Maintenance therapy — Because of the toxicity of long-term cyclophosphamide therapy, a number of less toxic drugs have been used for maintenance thera.")
52
Após 01 ano

53
Evolução do Caso Artrite Reumatóide No desmame do tratamento:
Artrite simétrica de IFP e MCP 9 dosagens de ANCA negativas Nunca acometeu seios face ou rins Artrite Reumatóide Immunosuppressive medications — Immunosuppressive therapy in addition to glucocorticoids is generally given if: there is persistent inflammation after two to three weeks of treatment there is progression of disease to a more severe variant (eg, the evolution of diffuse anterior scleritis into the necrotizing subtype) There are no randomized trials in scleritis on which to base the choice of the specific immunosuppressive medication. However, because of the proven effectiveness of both rituximab and cyclophosphamide in patients with granulomatosis with polyangiitis (Wegener’s), the first-line immunosuppressive medication in the treatment of scleritis is typically one of these agents. (See "Initial immunosuppressive therapy in granulomatosis with polyangiitis (Wegener's) and microscopic polyangiitis".) Options other than rituximab or cyclophosphamide for patients with milder disease in need of a steroid-sparing agent include cyclosporine, mycophenolate mofetil, and methotrexate. Mycophenolate mofetil has primarily been studied as a steroid-sparing agent, with variable efficacy [4,5], and may also be used as maintenance therapy; methotrexate has been used in a similar fashion [6]. Rituximab — Two rituximab regimens are effective in the treatment of rheumatic conditions. Either of these rituximab regimens is an acceptable first-line approach for the treatment of patients with scleritis refractory to glucocorticoids alone. The administration of 1 gram of rituximab twice (with the two doses separated by approximately 15 days) is the regimen approved by the US FDA for the treatment of rheumatoid arthritis. In addition, the use of four 375 mg/m2 doses administered one week apart have been approved by the FDA for the treatment of ANCA-associated vasculitis. (See "Treatment of cyclophosphamide-resistant granulomatosis with polyangiitis (Wegener’s) and microscopic polyangiitis", section on 'Rituximab'.) Cyclophosphamide — For patients with disease refractory to rituximab, we suggest cyclophosphamide (2 mg/kg per day, with dose adjustments for patients with decreased renal function). We suggest initiating oral cyclophosphamide therapy at a dose of 2 mg/kg per day, with dose adjustments for patients with decreased renal function [7]. With the use of cyclophosphamide, the general approach is to establish disease control as quickly as possible through combination therapy with prednisone and then to discontinue cyclophosphamide after three to six months. Cyclophosphamide is replaced by a medication with a lower risk of toxicity, usually azathioprine or methotrexate. Cyclosporine — Cyclosporine has been used in place of cyclophosphamide in a small case series of patients with severe scleritis [8,9]. The typical dose ranges from 2 to 3 mg/kg per day in two divided doses. Maintenance therapy — Because of the toxicity of long-term cyclophosphamide therapy, a number of less toxic drugs have been used for maintenance thera
 There are no randomized trials in scleritis on which to base the choice of the specific immunosuppressive medication. However, because of the proven effectiveness of both rituximab and cyclophosphamide in patients with granulomatosis with polyangiitis (Wegener’s), the first-line immunosuppressive medication in the treatment of scleritis is typically one of these agents. (See Initial immunosuppressive therapy in granulomatosis with polyangiitis (Wegener s) and microscopic polyangiitis .) Options other than rituximab or cyclophosphamide for patients with milder disease in need of a steroid-sparing agent include cyclosporine, mycophenolate mofetil, and methotrexate. Mycophenolate mofetil has primarily been studied as a steroid-sparing agent, with variable efficacy [4,5], and may also be used as maintenance therapy; methotrexate has been used in a similar fashion [6]. Rituximab — Two rituximab regimens are effective in the treatment of rheumatic conditions. Either of these rituximab regimens is an acceptable first-line approach for the treatment of patients with scleritis refractory to glucocorticoids alone. The administration of 1 gram of rituximab twice (with the two doses separated by approximately 15 days) is the regimen approved by the US FDA for the treatment of rheumatoid arthritis. In addition, the use of four 375 mg/m2 doses administered one week apart have been approved by the FDA for the treatment of ANCA-associated vasculitis. (See Treatment of cyclophosphamide-resistant granulomatosis with polyangiitis (Wegener’s) and microscopic polyangiitis , section on Rituximab .) Cyclophosphamide — For patients with disease refractory to rituximab, we suggest cyclophosphamide (2 mg/kg per day, with dose adjustments for patients with decreased renal function). We suggest initiating oral cyclophosphamide therapy at a dose of 2 mg/kg per day, with dose adjustments for patients with decreased renal function [7]. With the use of cyclophosphamide, the general approach is to establish disease control as quickly as possible through combination therapy with prednisone and then to discontinue cyclophosphamide after three to six months. Cyclophosphamide is replaced by a medication with a lower risk of toxicity, usually azathioprine or methotrexate. Cyclosporine — Cyclosporine has been used in place of cyclophosphamide in a small case series of patients with severe scleritis [8,9]. The typical dose ranges from 2 to 3 mg/kg per day in two divided doses. Maintenance therapy — Because of the toxicity of long-term cyclophosphamide therapy, a number of less toxic drugs have been used for maintenance thera.")
54
E a presença inicial do ANCA-c?

55
ANCA-c na Artrite Reumatóide
18%: ANCA títulos < 1/50 – não valorizados 19,8%: ANCA+ (mais comum ANCA-p) 13% casos: c-ANCA baixos títulos
 13% casos: c-ANCA baixos títulos.")
56
ANCA-c na Artrite Reumatóide
Pctes com Artrite Reumatóide ANCA+: FR altos títulos Maior positividade do FAN Maior comprometimento funcional

57
Reação a drogas da AR? Artrite Reumatóide (FR+) há 5 anos
Surgimento de vasculite ANCA-c (PR3 – altos títulos): GNRP e vasculite cutânea 3 meses pós-infliximab
: GNRP e vasculite cutânea 3 meses pós-infliximab.")
58
ANCA-c: falso positivo?
A sensibilidade e especificidade da IF varia pois depende do extrato utilizado ANCA-c baixos títulos: Associado a vasculite ANCA em 50% casos testados Observado em outras condições clínicas Principalmente colagenoses Stone, JH et al. Arthritis Care Res, 2000

59
Grupo de Doenças Intersticiais Pulmonares InCor- HC-FMUSP
Obrigada Grupo de Doenças Intersticiais Pulmonares InCor- HC-FMUSP

Apresentações semelhantes













, e que pode levar a incapacitação funcional.>")



>")

>")



 Westergren homem 1H mm mulher 1H>")


