Carregar apresentação
A apresentação está carregando. Por favor, espere

2
Atualização em HIV/AIDS
Dr. Ricardo da Silva de Souza

3
Agenda O vírus do HIV Epidemiologia História da doença Diagnóstico
Exames Princípios terapêuticos Transmissão vertical Profilaxia Perguntas

4
Vírus HIV-1 Origem: várias teorias
Classificação: Retrovirus (FIV,SIV...) Subtipos Grupo M Grupo O Grupo N
 Subtipos. Grupo M. Grupo O. Grupo N.")
5
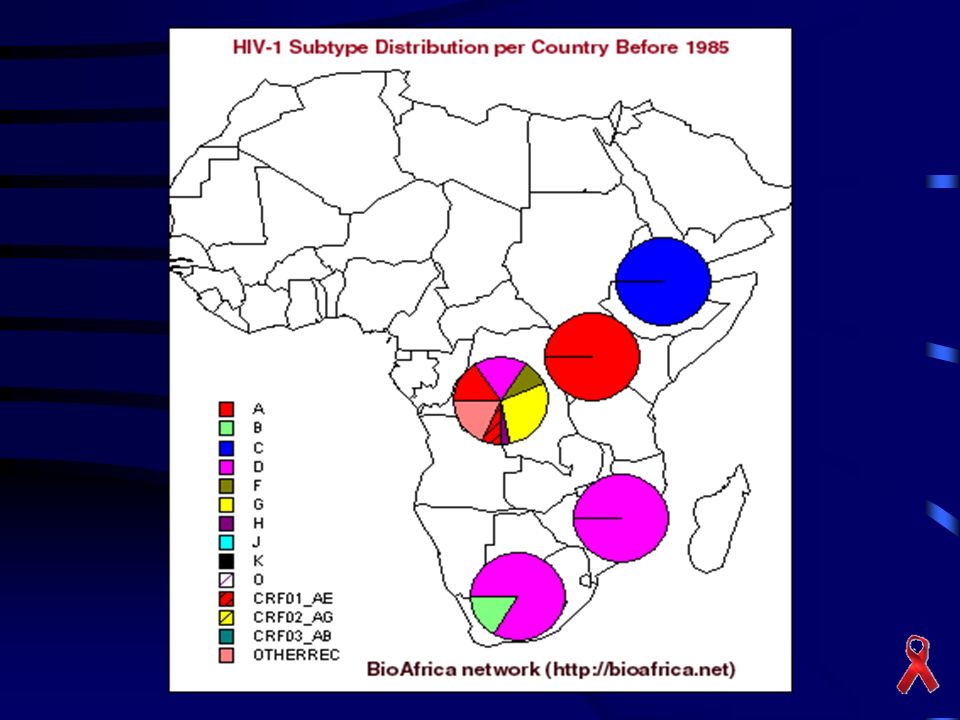
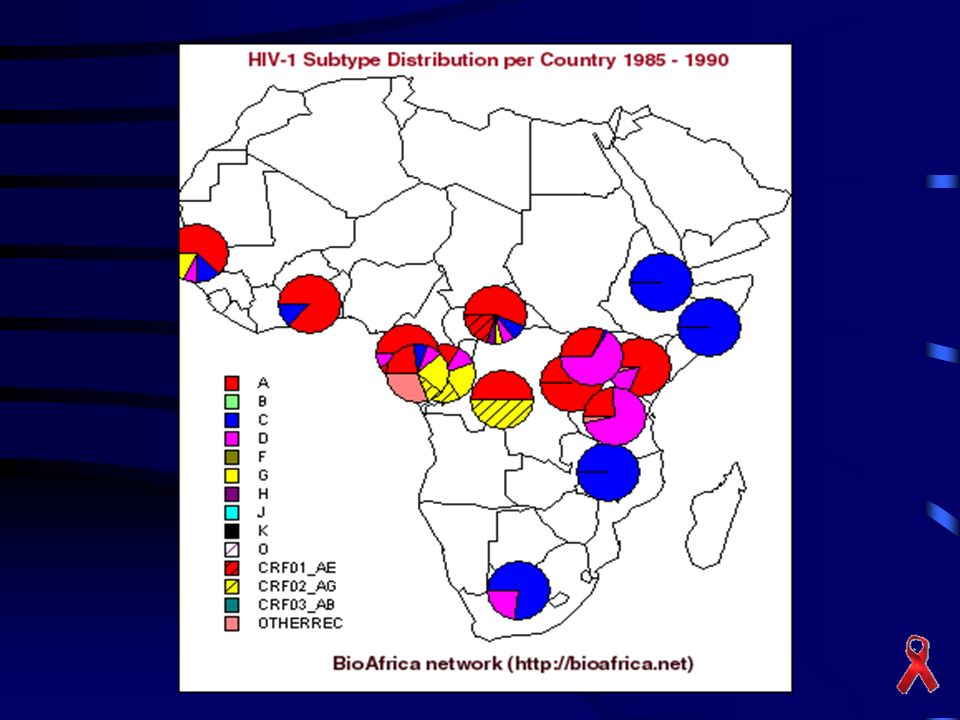
Subtipos Virais

6
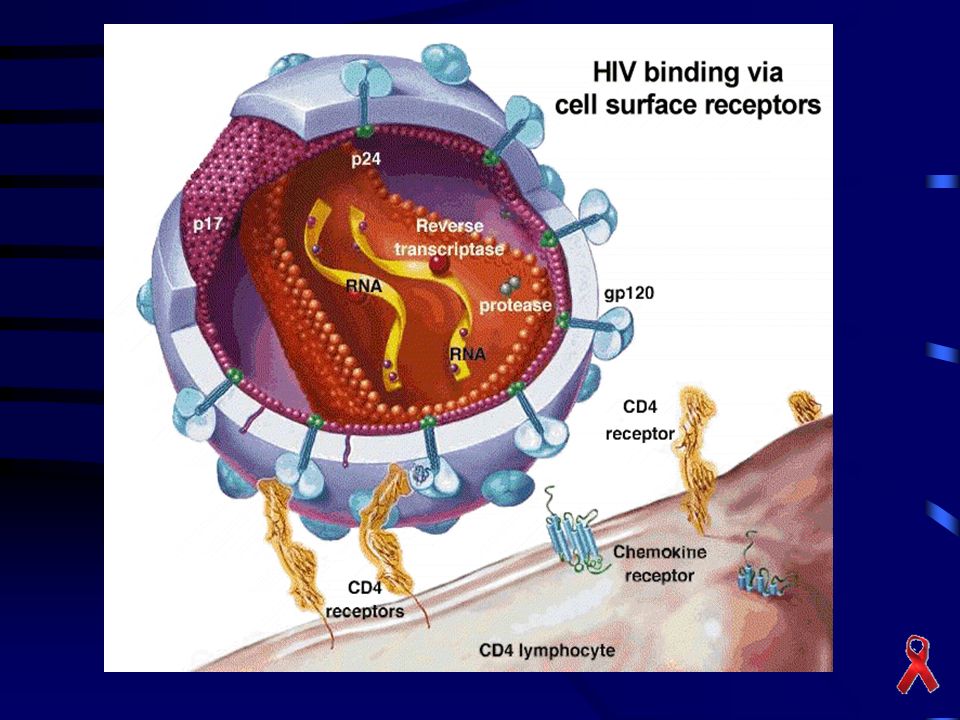
Estrutura do HIV

7
Estrutura Genética do HIV-1

9
Ciclo de Vida do HIV

11
Adultos e Criançãs com HIV/AIDS no Mundo
Eastern Europe 1.8 million Western Europe 680,000 N. America 1.2 million Asia & Pacific 9.5 million North Africa 730,000 Caribbean 590,000 This slide shows the geographical burden of HIV which many of you are familiar with. By far the largest burden is in Subsaharan Africa where the first wave of the epidemic occurred and we now have a devastating pandemic with 28 million people living with HIV. The second biggest burden in terms of absolute numbers is in the Asia Pacific region with 9.5 million infections, followed by Latin America with 1.9 million infections, and Eastern Europe with 1.8 million infections. AIDS is truly a global pandemic of vast proportions. Sub-Saharan Africa million Latin America 1.9 million Australia & New Zealand 18,000 Total: 40 million (34-46 million) UNAIDS 2003
 UNAIDS")
12
Número anual de novos casos em adultos e crianças
Eastern Europe 280,000 N. America 54,000 Western Europe 40,000 Asia & Pacific 1.4 million Caribbean 80,000 Sub-Saharan Africa 3.4 million Where the estimated 5 million new infections are occuriing is shown in this slide million or 68% of the world’s new infections in 2003 occurred in Subsahran Africa. A further 1.4 million infections or 28% occurred in the Asia and Pacific region, 6% Eastern Europe and 5% in Latin America and the Carribean combined. Latin America 180,000 Australia & New Zealand 1,000 Total: 5.0 million UNAIDS 2003

13
Crescimento de Casos e Mortes por HIV/AIDS, 1999-2003
According to the latest UNAIDS 2003 estimates, the number of people living with HIV in the world continues to increase each year as does the number of estimated deaths. UNAIDS 2003

14
Adult Prevalence in HIV Infection
15%-36% 5%-15% 1%-5% 0.5%-1% 0.1%-0.5% 0%-0.1% Not available Adult prevalence rate But these absolute numbers I have just described translate into relatively different burdens of disease when we look at what proportion of the adult population is affected. Based on the best available UNAIDS data and estimates, the adult prevalence in Subsahran Africa has now reached nearly 40% in some areas such as South Africa, Botswana and Swaziland shown here in this slide in the dark red. In contrast, despite the large absolute numbers in Asia, the adult prevalence rate remains 1% or less for most of the region. Similarly the adult prevalence in Brazil and much of the rest of Latin America is 1% or less. UNAIDS 2003

15
Perda de expectativa de vida por HIV/AIDS
Life expectancy without HIV/AIDS 65 60 55 50 -28 years Botswana -24 years Lesoto In Africa, the story of AIDS has been through at least three chapters. The first chapter was one where HIV spread largely silently – and the voices of people living with HIV were almost totally silent. Africa’s second chapter was one of increasing illness and death – the decade that has just been witnessed. We are entering the third chapter now. It is a chapter where we see the first large scale impact of AIDS on entire societies, their prosperity and their security. Life expectancy is the most basic measure of human progress, and by this measure, many African countries have seen half a century of progress wiped out by AIDS. -28 years Swaziland -35 years Zimbabwe Decline in life expectancy by Source: UNDP

16
Portadores do HIV no Brasil
17
Modos de Transmissão Contato sexual Contato direto com sangue
Semem Secreção vaginal Contato direto com sangue Transfusão Agulhas contaminadas Transmissão vertical Leite materno

18
Mitos sobre Transmissão
Ar Manuseio de objetos Picadas de insetos Uso de vasos sanitários

19
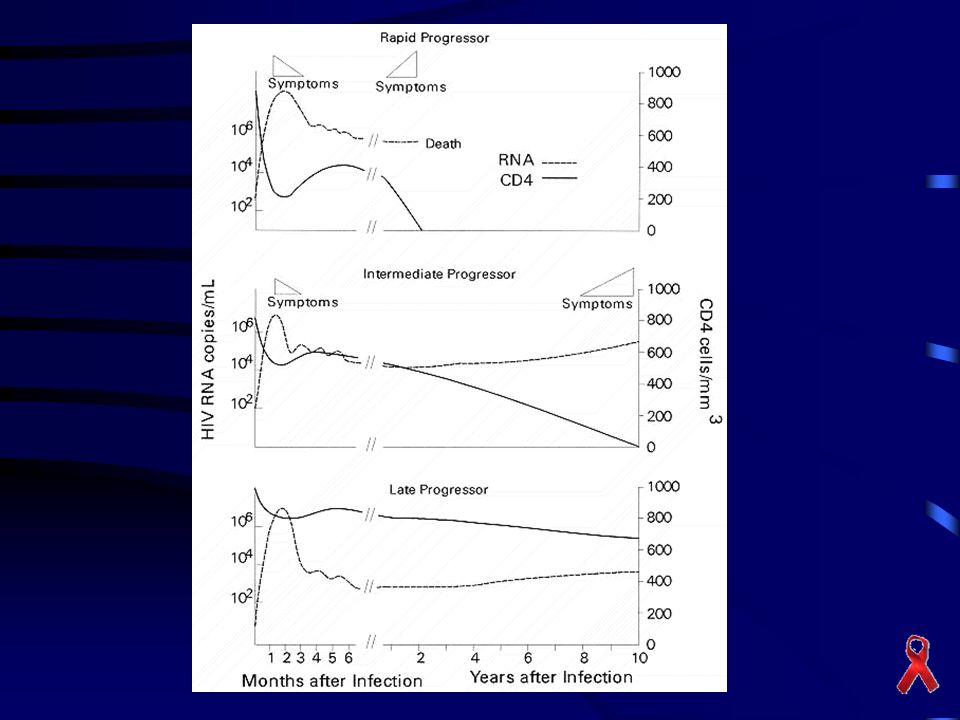
Progressão da Doença Infecção
Síndrome aguda ou infecção primária (período janela) Período assintomático (7 a 10 anos) AIDS (infecções oportunistas, CD4 < 200)
 Período assintomático (7 a 10 anos) AIDS (infecções oportunistas, CD4 < 200)")
20
Linfócito infectado com HIV

21
Síndrome Aguda Suores noturnos Febre de origem desconhecida
Rash eritematoso maculopapular Faringite Linfoadenopatia Hepatoesplenomegalia Mialgias

22
Exanthematous skin rash commonly associated with primary HIV infection
Exanthematous skin rash commonly associated with primary HIV infection. This patient's rash is concentrated on his upper back. Source: Diagnostic Picture Tests in Clinical Infectious Disease (1996, p 19, Fig. 36), Copyright © 1996 Times Mirror International Publishers Limited.
, Copyright © 1996 Times Mirror International Publishers Limited.")
23
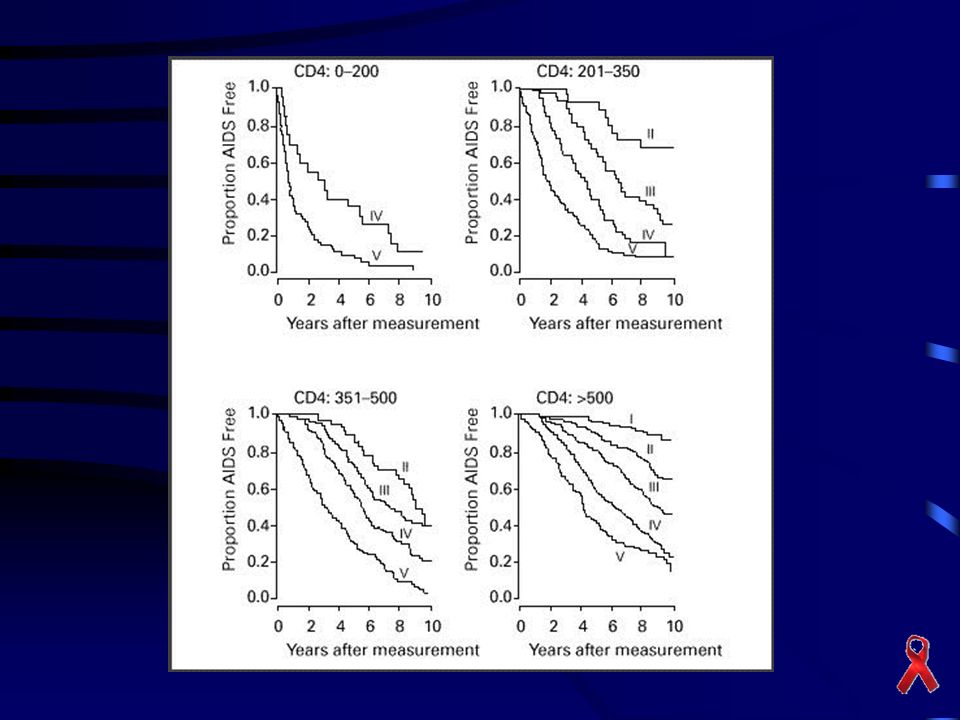
História Natural da Doença

26
Doenças Definidoras de AIDS
Candidíase do esôfago PCP Sarcoma de Kaposi Câncer cervical invasivo Criptococose extrapulmonar Criptosporidiose com diarréia>1 mês Citomegalovirose Histoplasmose extrapulmonar Tuberculose pulmonar disseminada Toxoplasmose de órgãos internos ...

27
Diagnóstico Laboratorial
Elisa Western Blot DNA PCR Testes Rápidos

28
Teste Rápido

29
Princípios Terapêuticos
Iniciar terapia antes de danos irreversíveis ao sistema imunológico (Cd4>400). Supressão da replicação viral a níveis não detectáveis pelo PCR (500 cópias - 50 cópias). Evitar resistência viral. Monitoramento com carga viral e Cd4.
. Supressão da replicação viral a níveis não detectáveis pelo PCR (500 cópias - 50 cópias). Evitar resistência viral. Monitoramento com carga viral e Cd4.")
30
Antiretrovirais Inibidores da Transcriptase Reversa
Nucleosídeos Não nucleosídeos Inibidores da Protease

31
Atuação dos Antiretrovirais

32
Objetivo Terapêutico

33
Fontes de Vírus Plasmático
Infected activated CD4+ T lymphoblasts Resting CD4+ T cells with unintegrated HIV-1 DNA Virions on FDC Resting CD4+ T cells with integrated provirus Infected macrophages Multiple cell types and sites contribute to plasma viremia. These cells have different rates of turnover. The activated CD4+ 1 2 3 4 44 months Half-life (months)
")
34
Infected Activated CD4 Cells: Predominant Sources of Plasma Virus
†

35
Life Cycle of HIV-1 in Activated CD4+ T Cells
Attachment to CD4 and CCR Entry of viral genomic RNA into cytoplasm Reverse transcription of viral RNA into DNA In the absence of antiretroviral therapy, the virus replication is continuous…in activated CD4+ Integration of viral DNA into host chromosome Production of viral RNA and protein Assembly, release and maturation of virus particles Generation time: 1.5 days

36
Evolutionary history of HIV and other lentivirues
Based on phylogenetic analysis of HIV and SIV, a close relationship between HIV1 and SIV from chimpanzee strains has been established and a close genetic relationship between HIV-2 and SIV from sooty mangabees Rambaut et al 2004

37
AIDS as a zoonosis SIVcpz and HIV-1 SIVsm and HIV-2
This led to the hypothesis that the HIV-1 virus was in fact a zoonotic pathiogen that had emerged from West/Central Africa. The virus crossed species from chimpanzees to Humans at some point in the past and this may have occurred as a result of bushmeat hunting practices. Similarily, HIV-2 is thought to have originated in West Africa and resulted from SIV from sooty mangabeys crossing species probably from similar hunting practices. Pan troglodytes (chimpanzee) Cercobrus atys (sooty mangabey)
 Cercobrus atys (sooty mangabey)")
38
HIV classification A B C D Type 2 “E” HIV F Group M G Type 1 H Group O
This genomic diversity has led to the following classification scheme: Two types: HIV-1 HIV-2 HIV-1 has been further classified based on the basis of differences in the envelope nucleotide sequences: 3 groups M (main) O (outlier) N (non-M/non-O) The envelope protiens for example of M and O differ by as much as 30-50% as does the N group. Group M, which accounts for >90% of reported HIV cases is further subdivided into at 9 least disctinct subtypes. The E, I subtypes are not true subtypes based on the full genome sequencing “I” J Group N K ? L
 O (outlier) N (non-M/non-O) The envelope protiens for example of M and O differ by as much as 30-50% as does the N group. Group M, which accounts for >90% of reported HIV cases is further subdivided into at 9 least disctinct subtypes. The E, I subtypes are not true subtypes based on the full genome sequencing. I J. Group N. K. L.")
39
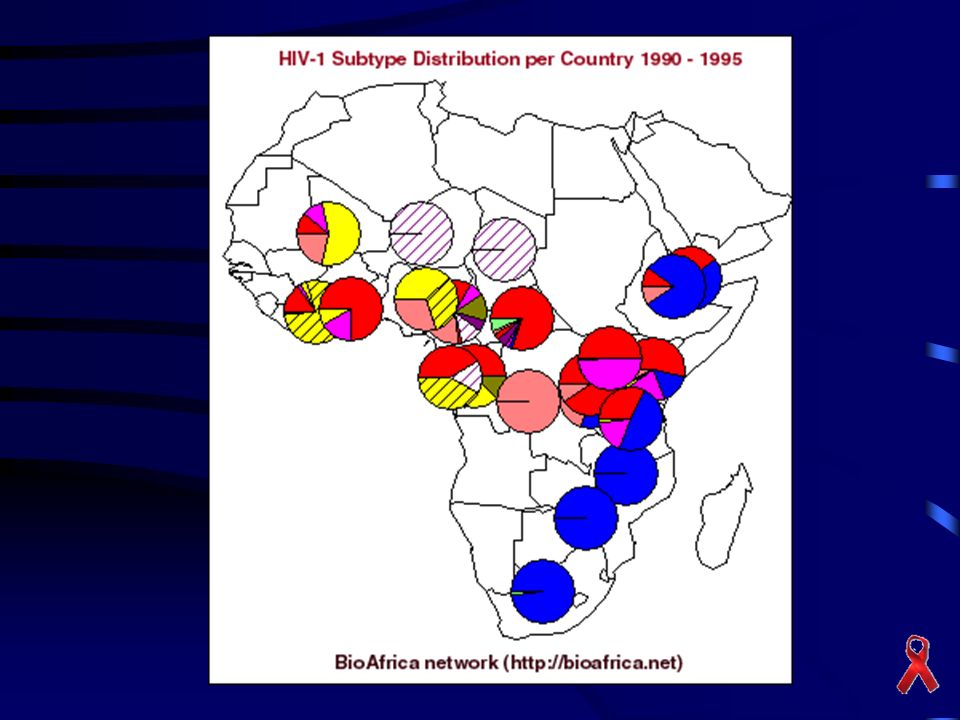
Distribuição Global do HIV-1 env subtipos, 2000
5% 5% 47% 27% 12% Osmanov et al, JAIDS 2002

40
Quais as implicações da diversidade genética ( subtipos)?
")
41
Impacto da diversidade no diagnóstico
Maioria dos testes de baseado no subtipo B. Subtipo O pode apresentar problemas. E.x. detecção de infecção recente utilizando STARHS depende do subtipo: Subtype B in USA : 180 days Subtype AE in Thailand: 347 days

42
Impact of HIV subtype diversity on HIV-1 virulence
Some studies suggest AIDS progression differs as a function of subtype Patients with subtype A or G lived symptom free longest, followed by subtype D and C was associated with rapid disease progression (Kanki JID 1999) Patients with subtype D had lower CD4 and faster disease progression and death than subtype A (Kaleebu JID 2002) Patients with subtype C were found to have higher rates of viremia and lowest CD4 and progression to AIDS compared to patinets with A and D subtypes Relationship between HIV-1 subtypes and disease transmissibility and progression is poorly understood
 Patients with subtype D had lower CD4 and faster disease progression and death than subtype A (Kaleebu JID 2002) Patients with subtype C were found to have higher rates of viremia and lowest CD4 and progression to AIDS compared to patinets with A and D subtypes. Relationship between HIV-1 subtypes and disease transmissibility and progression is poorly understood.")
43
Impact of HIV genetic diversity on treatment
Limited data for non-B subtype Do ARV drugs have the same activity against non-B subtypes? NRTI Some studies have found lower rates of some NRTI resistance mutations in non-B but primary drug resistance mutations seem similar to B NNRTI natural resistance of HIV-2 and HIV-1 subtype O Higher rate of NVP resistance in subtype D than A (Eshelman JAIDS 2004)
")
44
Impact of HIV genetic diversity on treatment
PIs There may be different pathways of drug resistance based on subtype L90M instead of D30N in non-B patients exposed to nelfinavir Many secondary PI mutations identified at higher frequency in non-B The significance of these findings is still not clear

45
Relevância Clínica da Existência dos Subtipos Virais
Diagnóstico: formas recombinantes dificultam o resultado dos testes Elisa (falso negativo) Monitoramento dos pacientes: nem todas as metodologias de carga viral (RNA) são sensíveis a subtipos não-B Não sensíveis: Roche Amplicor 1.0, RT-PCR 1.0 Sensíveis de baixa reproducibilidade: b-DNA, Nuclisens, Ultra Direct Monitor Genotipagem (painéis específicos para o subtipo B)
 Monitoramento dos pacientes: nem todas as metodologias de carga viral (RNA) são sensíveis a subtipos não-B. Não sensíveis: Roche Amplicor 1.0, RT-PCR 1.0. Sensíveis de baixa reproducibilidade: b-DNA, Nuclisens, Ultra Direct Monitor. Genotipagem (painéis específicos para o subtipo B)")
46
Relevância Clínica da Existência dos Subtipos Virais
Tratamento antiretroviral Mutações específicas (subtipo C protease) Não utilizar Nevirapina para HIV-2 Desenvolvimento de vacinas Superinfeção
 Não utilizar Nevirapina para HIV-2. Desenvolvimento de vacinas. Superinfeção.")
47
Aumento do Subtipo C Nos últimos 10 anos o subtipo C está crescendo mais que outros subtipos Hoje 56% das infeções no mundo Principais áreas de crescimento: sul da China, India, Africa do Sul e sul do Brasil Identificado subtipo C específico do Brasil (2003) Mutações específicas para alguns antiretrovirais
 Mutações específicas para alguns antiretrovirais.")
51
Diversidade Genética do HIV-1 na América do Sul 2001

52
Diversidade Genética do HIV-1 na Brasil 2003

53
Porto Alegre - Hospital das Clínicas 2002

54
Exposição Ocupacional

55
Prevenção Precaução universal Material de proteção SEMPRE USAR LUVAS
Qualquer sangue ou fluído corporal é potencialmente infeccioso e deve ser manuseado de acordo Material de proteção Para pele, olhos, boca, membranas mucosas, roupa SEMPRE USAR LUVAS

56
Exposição Ocupacional
Fatores de risco Tipo de contato Local Volume de sangue Status do paciente fonte Condições de saúde do profissional

57
Exposição Ocupacional
Profissões com maior ocorrências Enfermeiros Técnicos de Laboratório Risco por exposição: Aprox %

58
Causas de Acidentes Percutâneos

59
Risco de Exposição e Fluídos Corporais

60
Profilaxia Pós-exposição

61
Gerenciamento Pós-exposição
Limpeza do ferimento Avaliação da exposição Aconselhamento Testagem (Teste Rápido) Profilaxia ( Iniciar em até 48 horas)
 Profilaxia ( Iniciar em até 48 horas)")
62
Mensagem final HIV não tem cura mas é tratável
12 antiretrovirais oferecidos pelo governo Problemas com aderência Identificar paciente na fase assintomática – testagem Profilaxia para exposição ocupacional e não ocupacional

Apresentações semelhantes







 REDUZIR RISCO DE TRANSMISSÃO>")



 HEPATITE B (HVB) HEPATITE.>")





 foi alertado para o aparecimento de uma nova doença. Em oito meses apareceram, na.>")

