Carregar apresentação
A apresentação está carregando. Por favor, espere

1
ALTERAÇÕES HEMODINÂMICAS DURANTE O PROCEDIMENTO HEMODIALÍTICO
Prof. Dr. Sebastião Rodrigues Ferreira Filho Universidade Federal de Uberlândia, MG Eu gostaria de agradecer os organizadores do 13 congresso mineiro de Nefrologia e tambem o I encontro inter estadual de Nefrologia pelo convite. O meu tema é “ Alterações hemodinamicas durante o procedimento dialitico”. Este é um tópico bastante interessante pois, nós nefrologistas convivemos a maior parte do nosso tempo, cuidando de pacientes que estão em procedimento diálitico dentro dos nossos hospitais e clinicas. As variações hemodinamicas sistêmicas muitas vezes podem ser detectadas por aferiçoes simples de pressão arterial e frequencia cardiaca e ganham cada vez mais importancia na determinação das taxas de morbidade e mortalidade dos pacientes renais cronicos. VIII

2
Pressão Arterial Débito Cardíaco mmHg L/min Total de Fluidos Intra-Torácico Kohm-1 Resistência Periférica Para voces terem uma ideia, os pacientes renais cronicos podem apresentar com diferentes estados hemodinamicos para o inicio de uma diálise. Aqui, neste estudo que estamos iniciando, os pacientes se apresentam sem edemas, no seu chamado peso seco, sem dispneia e...mesmo assim apresentam-se diferentemente para a diálise. Citar os pacientes Dyne sec cm -5 Padrões hemodinâmicos encontrados em pacientes portadores de doença renal crônica. Pacientes em CAPD (sem edemas e/dispneia) Valéria C Ferreira, Carlos F M A Rodrigues, Sebastião R Ferreira-Filho Núcleo de Pesquisas Clínicas - Nefroclínica de Uberlândia. (Fevereiro-2009)
 Valéria C Ferreira, Carlos F M A Rodrigues, Sebastião R Ferreira-Filho. Núcleo de Pesquisas Clínicas - Nefroclínica de Uberlândia. (Fevereiro-2009)")
3
Causas de Instabilidade Hemodinâmica com Hipotensão Arterial
Rápida redução da osmolaridade plasmática; Remoção rápida de fluidos para atingir o peso seco; Determinação inadequada do peso seco; Disfunção autonômica Refeições durante a HD; Uso de acetato; Uso de anti hipertensivos; Arritmias, reações alérgicas, liberação de substancias vasodilatadoras.

4
Water movement during standard hemodialysis
Redução da Osmolaridade William L Henrich, MD, MACP version 16.3: Outubro 2008 Schematic representation of water movement during standard hemodialysis. Plasma at an osmolality of 320 mosmol/kg flows into the dialyzer (step 1) which is perfused with a dialysate having an osmolality of 280 mosmol/kg. Diffusive loss of urea (and other small solutes) lowers the osmolality of the fluid returning to the patient (step 2). The ensuing fall in extracellular osmolality creates an osmotic gradient favoring water movement into the cells. This effect plus water loss by ultrafiltration across the dialyzer leads to extracellular volume depletion and may cause hypotension. The rapid fall in plasma osmolality also may play a contributory role, perhaps by interfering with sympathetic responsiveness to volume depletion.
 which is perfused with a dialysate having an osmolality of 280 mosmol/kg. Diffusive loss of urea (and other small solutes) lowers the osmolality of the fluid returning to the patient (step 2). The ensuing fall in extracellular osmolality creates an osmotic gradient favoring water movement into the cells. This effect plus water loss by ultrafiltration across the dialyzer leads to extracellular volume depletion and may cause hypotension. The rapid fall in plasma osmolality also may play a contributory role, perhaps by interfering with sympathetic responsiveness to volume depletion.")
5
Remoção de fluidos Abstract—Volume excess is thought to be important in the pathogenesis of hypertension among hemodialysis patients. To determine whether additional volume reduction will result in improvement in blood pressure (BP) among hypertensive patients on hemodialysis and to evaluate the time course of this response, we randomly assigned long-term hypertensive hemodialysis patients to ultrafiltration or control groups. The additional ultrafiltration group (n100) had the dry weight probed without increasing time or duration of dialysis, whereas the control group (n50) only had physician visits. The primary outcome was change in systolic interdialytic ambulatory BP. Postdialysis weight was reduced by 0.9 kg at 4 weeks and resulted in 6.9 mm Hg (95% CI: 12.4 to 1.3 mm Hg; P0.016) change in systolic BP and 3.1 mm Hg (95% CI: 6.2 to 0.02 mm Hg; P0.048) change in diastolic BP. At 8 weeks, dry weight was reduced 1 kg, systolic BP changed 6.6 mm Hg (95% CI: 12.2 to 1.0 mm Hg; P0.021), and diastolic BP changed 3.3 mm Hg (95% CI: 6.4 to 0.2 mm Hg; P0.037) from baseline. The Mantel-Hanzel combined odds ratio for systolic BP reduction of 10 mm Hg was 2.24 (95% CI: 1.32 to 3.81; P0.003). There was no deterioration seen in any domain of the kidney disease quality of life health survey despite an increase in intradialytic signs and symptoms of hypotension. The reduction of dry weight is a simple, efficacious, and well-tolerated maneuver to improve BP control in hypertensive hemodialysis patients. Long-term control of BP will depend on continued assessment and maintenance of dry weight. r
 among hypertensive patients on hemodialysis and to evaluate the time course of this response, we randomly assigned long-term hypertensive. hemodialysis patients to ultrafiltration or control groups. The additional ultrafiltration group (n100) had the dry weight probed without increasing time or duration of dialysis, whereas the control group (n50) only had physician visits. The primary outcome was change in systolic interdialytic ambulatory BP. Postdialysis weight was reduced by 0.9 kg at 4 weeks and resulted in 6.9 mm Hg (95% CI: 12.4 to 1.3 mm Hg; P0.016) change in systolic BP and 3.1 mm Hg (95% CI: 6.2 to 0.02 mm Hg; P0.048) change in diastolic BP. At 8 weeks, dry weight was reduced 1 kg, systolic BP changed 6.6 mm Hg (95% CI: 12.2 to 1.0 mm Hg; P0.021), and diastolic BP changed 3.3 mm Hg (95% CI: 6.4 to 0.2 mm Hg; P0.037) from baseline. The Mantel-Hanzel combined odds ratio for systolic BP reduction of 10 mm Hg was 2.24 (95% CI: 1.32 to 3.81; P0.003). There was no deterioration seen in any domain of the kidney disease quality of life health survey despite an increase in intradialytic signs and symptoms of hypotension. The reduction of dry weight is a simple, efficacious, and well-tolerated maneuver to improve BP control in hypertensive hemodialysis patients. Long-term control of BP will depend on continued assessment and maintenance of dry weight. r.")
6
n: 89 Euvolemicos 75% Hipovolemicos 25% Hipervolemicos 54% 19% 10%
Determinação inadequada do peso seco Clin J Am Soc Nephrol 1: 749–753, 2006 n: 89 19% Euvolemicos 75% 54% Hipovolemicos 25% Accurate intravascular volume assessment is critical in the treatment of patients who receive chronic hemodialysis (HD) therapy. Clinically assessed dry weight is a poor surrogate of intravascular volume; however, ultrasound assessment of the inferior vena cava (IVC) is an effective tool for volume management. This study sought to determine the feasibility of using operators with limited ultrasound experience to assess IVC dimensions using hand-carried ultrasounds (HCU) in the outpatient clinical setting. The IVC was assessed in 89 consecutive patients at two outpatient clinics before and after HD. Intradialytic IVC was recorded during episodes of hypotension, chest pain, or cramping. High-quality IVC images were obtained in 79 of 89 patients. Despite that 89% of patients presented at or above dry weight, 39% of these patients were hypovolemic by HCU. Of the 75% of patients who left HD at or below goal weight, 10% were still hypervolemic by HCU standards. Hypovolemic patients had more episodes of chest pain and cramping (33 versus 14%, P 0.06) and more episodes of hypotension (22 versus 3%, P 0.02). The clinic with a higher prevalence of predialysis hypovolemia had significantly more intradialytic adverse events (58 versus 27%; P 0.01). HCU measurement of the IVC is a feasible option for rapid assessment of intravascular volume status in an outpatient dialysis setting by operators with limited formal training in echocardiography. There is a poor relationship between dry weight goals and IVC collapsibility. Practice variation in the maintenance of volume status is correlated with significant differences in intradialysis adverse events. Clin J Am Soc Nephrol 1: 749–753, doi: /CJN After dialysis, similar discrepancies between dry weight and HCU also were noted. By weight criteria, 75% of patients had sufficient fluid removed to get to goal weight. However, only 13 to 19% of these patients were actually euvolemic using IVC measurements. A small proportion of HD patients who were at or below goal weight were still hypervolemic (9 to 10%), and nearly half (47 to 54%) were hypovolemic. No significant correlation was found between change in body weight and change in VCDi (r 0.14, NS), and there was a weak correlation between change in weight and change in IVCCI (r0.25, P 0.03). Hipervolemicos 10% r
 therapy. Clinically assessed dry weight is a poor surrogate of intravascular volume; however, ultrasound assessment of the. inferior vena cava (IVC) is an effective tool for volume management. This study sought to determine the feasibility of using. operators with limited ultrasound experience to assess IVC dimensions using hand-carried ultrasounds (HCU) in the. outpatient clinical setting. The IVC was assessed in 89 consecutive patients at two outpatient clinics before and after HD. Intradialytic IVC was recorded during episodes of hypotension, chest pain, or cramping. High-quality IVC images were. obtained in 79 of 89 patients. Despite that 89% of patients presented at or above dry weight, 39% of these patients were. hypovolemic by HCU. Of the 75% of patients who left HD at or below goal weight, 10% were still hypervolemic by HCU. standards. Hypovolemic patients had more episodes of chest pain and cramping (33 versus 14%, P 0.06) and more episodes. of hypotension (22 versus 3%, P 0.02). The clinic with a higher prevalence of predialysis hypovolemia had significantly more. intradialytic adverse events (58 versus 27%; P 0.01). HCU measurement of the IVC is a feasible option for rapid assessment. of intravascular volume status in an outpatient dialysis setting by operators with limited formal training in echocardiography. There is a poor relationship between dry weight goals and IVC collapsibility. Practice variation in the maintenance of volume. status is correlated with significant differences in intradialysis adverse events. Clin J Am Soc Nephrol 1: 749–753, doi: /CJN After dialysis, similar discrepancies between dry weight and. HCU also were noted. By weight criteria, 75% of patients had. sufficient fluid removed to get to goal weight. However, only. 13 to 19% of these patients were actually euvolemic using IVC. measurements. A small proportion of HD patients who were at. or below goal weight were still hypervolemic (9 to 10%), and. nearly half (47 to 54%) were hypovolemic. No significant correlation. was found between change in body weight and change. in VCDi (r 0.14, NS), and there was a weak correlation. between change in weight and change in IVCCI (r0.25, P. 0.03). Hipervolemicos. 10% r.")
7
Disfunção autonômica r

8
Refeições durante a HD minutes 60 minutes

9
Hemodialysis-associated hypotension as an independent risk factor
for two-year mortality in hemodialysis patients. Shoji T, Tsubakihara Y, Fujii M, Imai E. Kidney Int Sep;66(3):
:")
10
Hemodialysis-associated hypotension as an independent risk factor
for two-year mortality in hemodialysis patients. Shoji T, Tsubakihara Y, Fujii M, Imai E. Kidney Int Sep;66(3):
:")
11
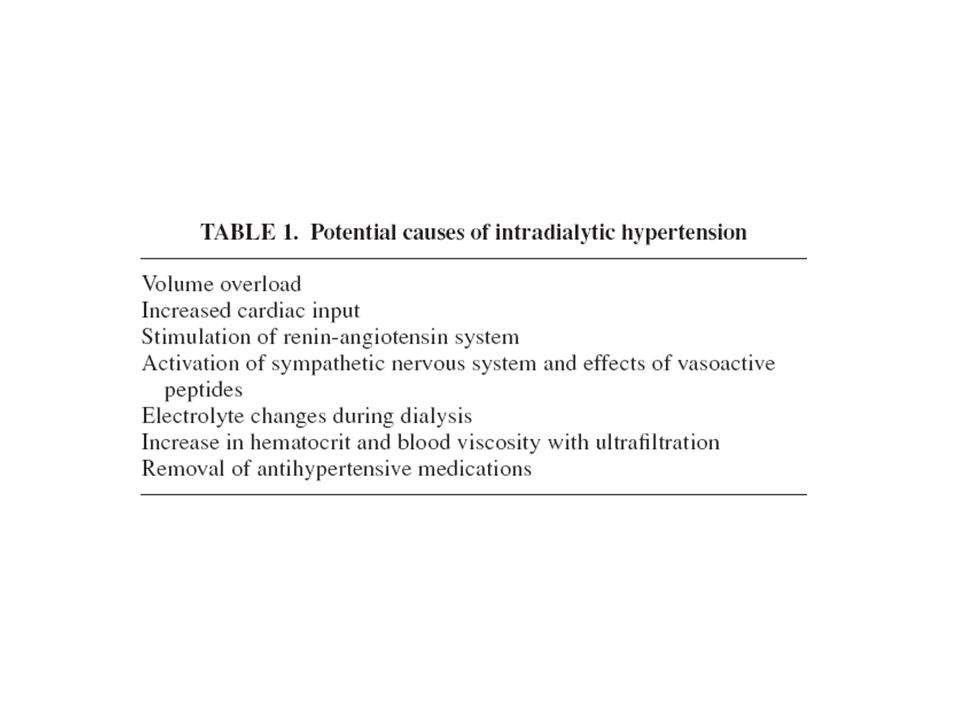
Hipertensão Arterial Intradialítica

12
Qualquer aumento da pressão arterial média acima de 15 mmHg,
Definição Qualquer aumento da pressão arterial média acima de 15 mmHg, durante ou imediatamente após a HD (1) Hipertensão durante a segunda ou terceira hora de HD, após significante ultra filtração (2) Aumento da pressão arterial resistente à ultra filtração (3) 1: Amerling RCG, Dubrow A, Levin N, Osheroff R: Complications during hemodialysis. In: Nissenson A, Gentile D (eds).Clinical Dialysis. Stamford,CT: Appleton & Lange, 1995:236–267 2: Fellner S: Intradialytic hypertension II.Semin Dial 6:371–373, 1993 3: Cirit M, Akcicek F, Terzioglu E, Soydas C, Ok E, Ozbasli CF, Basci A, Mees EJ: “Paradoxical” rise in blood pressure during ultrafiltration in dialysis patients. Nephrol Dial Transplant 10:1417–1420, 1995
 Hipertensão durante a segunda ou terceira hora de HD, após significante ultra filtração (2) Aumento da pressão arterial resistente à ultra filtração (3) 1: Amerling RCG, Dubrow A, Levin N, Osheroff R: Complications during. hemodialysis. In: Nissenson A, Gentile D (eds).Clinical Dialysis. Stamford,CT: Appleton & Lange, 1995:236–267. 2: Fellner S: Intradialytic hypertension II.Semin Dial 6:371–373, : Cirit M, Akcicek F, Terzioglu E, Soydas C, Ok E, Ozbasli CF, Basci A, Mees EJ: Paradoxical rise in blood pressure during ultrafiltration in dialysis patients. Nephrol Dial Transplant 10:1417–1420,")
14
Paradoxical rise in blood pressure during ultrafiltration is caused by increased cardiac output
Gunal, AI cols: J NEPHROL 2002; 15: 42-47 Isto aconteceu na primeira parte da dialise, na segunda houve queda da PAM b a r

15
Kidney International, (2007) 71, 454-461
∆ SBP = SBPi -SBPf

16
Kidney International, (2007) 71, 454-461
Combined outcome of 6-month mortality and non-access-related hospitalization among hypertensive (defined by KDOQI standards) ESRD subjects (n=343/431) mm Hg
 ESRD subjects (n=343/431) mm Hg.")
17
“U" curve association of blood pressure and mortality in hemodialysis patients.
Zager PG, Nikolic J, Brown RH, Campbell MA, Hunt WC, Peterson D, Van Stone J, Levey A, Meyer KB, Klag MJ, Johnson HK, Clark E, Sadler JH, Teredesai P. Kidney Int Aug;54(2):561-9. RR Pressão Arterial Sistólica Pós HD (mmHg) n = 5433 5 anos BACKGROUND: Hypertension may play an important role in the pathogenesis of the excess cardiovascular and cerebrovascular (CV) morbidity observed in hemodialysis patients (HD). However, the optimal blood pressure (BP) range for HD patients has not been defined. We postulated that there is a "U" curve relationship between BP and CV mortality. To explore this hypothesis we studied 5,433 HD patients in Dialysis Clinic Inc., a large not-for-profit chain, over a five year period. METHODS: Cox regression, with fixed and time-varying covariates, was used to assess the effect of systolic blood pressure (SBP) and diastolic blood pressure (DBP), pre- and post-dialysis, on CV mortality, while adjusting for age, gender, ethnicity, primary cause of end-stage renal disease, Kt/V, serum albumin, and antihypertensive medications. RESULTS: The overall impact of BP on CV mortality was modest. Pre-dialysis, neither systolic nor diastolic hypertension were associated with an increase in CV mortality. Post-dialysis, SBP > or = 180 mm Hg (RR = 1.96, P < 0.015) and DBP > or = 90 mm Hg (RR = 1.73, P < 0.05) were associated with increased CV mortality. Low SBP (SBP < 110 mm Hg) was associated with increased CV mortality, pre- and post-dialysis. CONCLUSIONS: The results suggest the presence of a "U" curve relationship between SBP post-dialysis and CV mortality in HD patients
: RR. Pressão Arterial Sistólica. Pós HD (mmHg) n = anos. BACKGROUND: Hypertension may play an important role in the pathogenesis of the excess cardiovascular and cerebrovascular (CV) morbidity observed in hemodialysis patients (HD). However, the optimal blood pressure (BP) range for HD patients has not been defined. We postulated that there is a U curve relationship between BP and CV mortality. To explore this hypothesis we studied 5,433 HD patients in Dialysis Clinic Inc., a large not-for-profit chain, over a five year period. METHODS: Cox regression, with fixed and time-varying covariates, was used to assess the effect of systolic blood pressure (SBP) and diastolic blood pressure (DBP), pre- and post-dialysis, on CV mortality, while adjusting for age, gender, ethnicity, primary cause of end-stage renal disease, Kt/V, serum albumin, and antihypertensive medications. RESULTS: The overall impact of BP on CV mortality was modest. Pre-dialysis, neither systolic nor diastolic hypertension were associated with an increase in CV mortality. Post-dialysis, SBP > or = 180 mm Hg (RR = 1.96, P < 0.015) and DBP > or = 90 mm Hg (RR = 1.73, P < 0.05) were associated with increased CV mortality. Low SBP (SBP < 110 mm Hg) was associated with increased CV mortality, pre- and post-dialysis. CONCLUSIONS: The results suggest the presence of a U curve relationship between SBP post-dialysis and CV mortality in HD patients.")
18
Conclusão As alterações hemodinâmicas ocorridas durante a hemodiálise são importantes fatores de risco na morbi e mortalidade desta população; Classificação quanto ao risco de desenvolver hiper ou hipotensão podem ajudar a tratar estes pacientes sem que tais modificações hemodinâmicas aconteçam durante a HD; Não podem ser tratadas como um fatos isolados e sem conseqüências futuras.

Apresentações semelhantes








 Dr. Eric J. Topol N. Engl.>")










