Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Mônica Corso Pereira Unicamp PUC - Campinas
Investigação Diagnóstica da Hipertensão Pulmonar Mônica Corso Pereira Unicamp PUC - Campinas

2
Quando pensar no diagnóstico?
1 65 anos HAS, DM, Dispneia aos medios esforços 2 Mulher, 30 anos Sem doenças prévias 3 Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas

3
Quando pensar no diagnóstico?
1 65 anos HAS, DM, Dispneia aos medios esforços 2 Mulher, 30 anos Sem doenças prévias 3 Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg

4
Quando pensar no diagnóstico?
1 65 anos HAS, DM, Dispneia aos medios esforços 2 Mulher, 30 anos Sem doenças prévias 3 Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas Achado incidental!! Investigação de dispneia Rastreamento PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg

5
RVP = PAP – PAE = PAP – PcapP
Ecocardiograma com sinais de HP PAP m = Q(fluxo) x RVP RVP = PAP – PAE = PAP – PcapP Fluxo DC PAP = PcapP + (DC X RVP)
 x RVP. RVP = PAP – PAE = PAP – PcapP. Fluxo DC. PAP = PcapP + (DC X RVP)")
6
HP : condição hemodinâmica
PAP m = Q(fluxo) x RVP RVP = PAP – PAE = PAP – PcapP Fluxo DC PAP = PcapP + (DC X RVP)
 x RVP. RVP = PAP – PAE = PAP – PcapP. Fluxo DC. PAP = PcapP + (DC X RVP)")
7
HP : condição hemodinâmica
Doença pulmonar ou hipóxia Multifatorial Tromboembólica HP Arterial Doença cardíaca esquerda

8
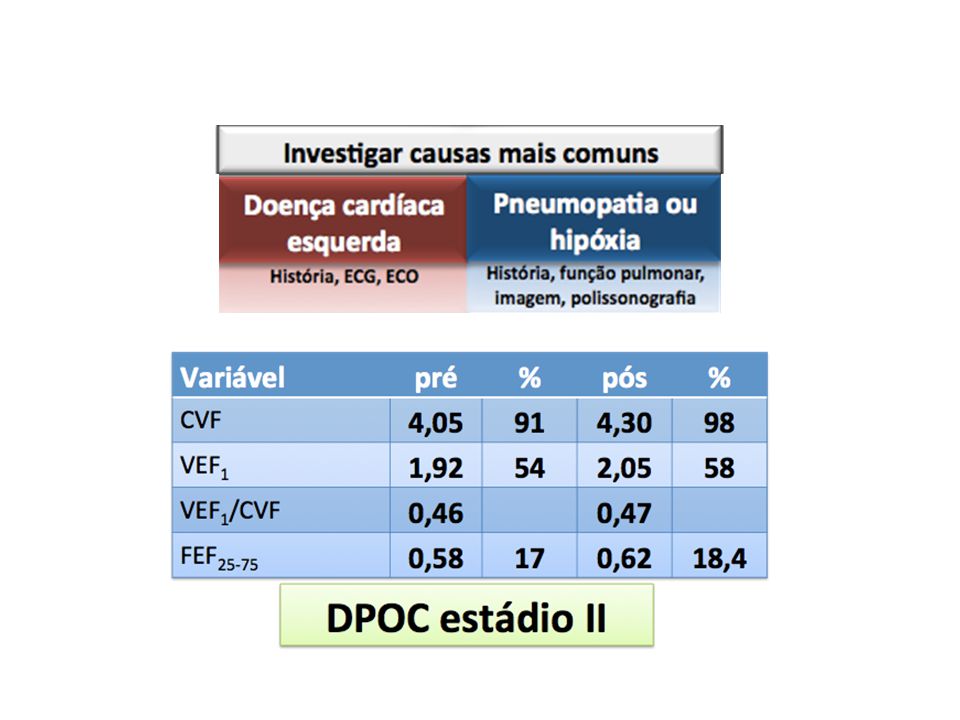
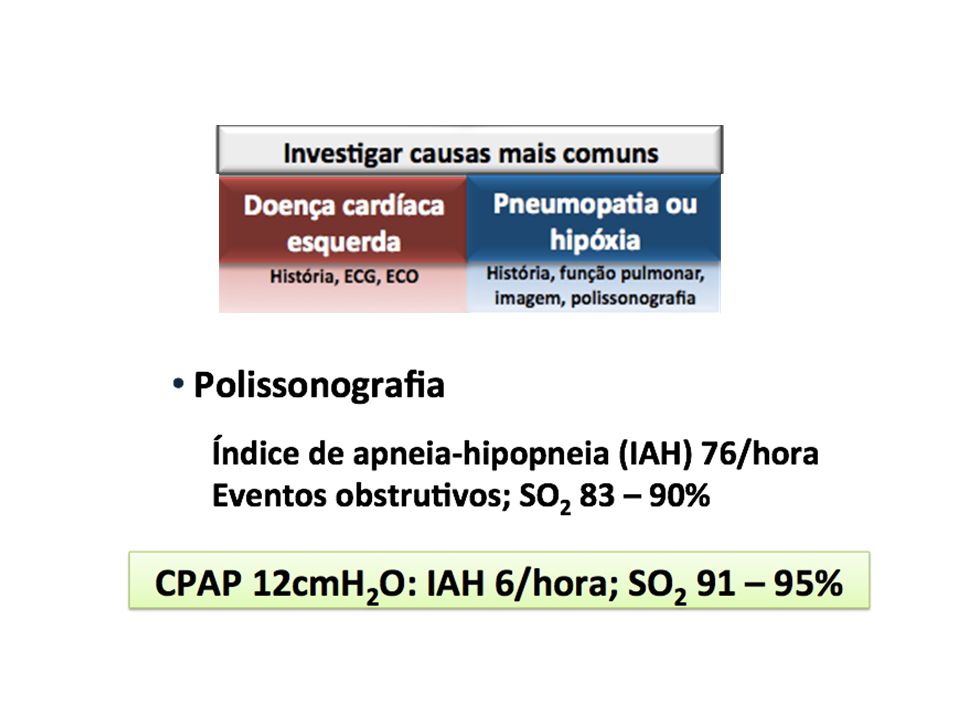
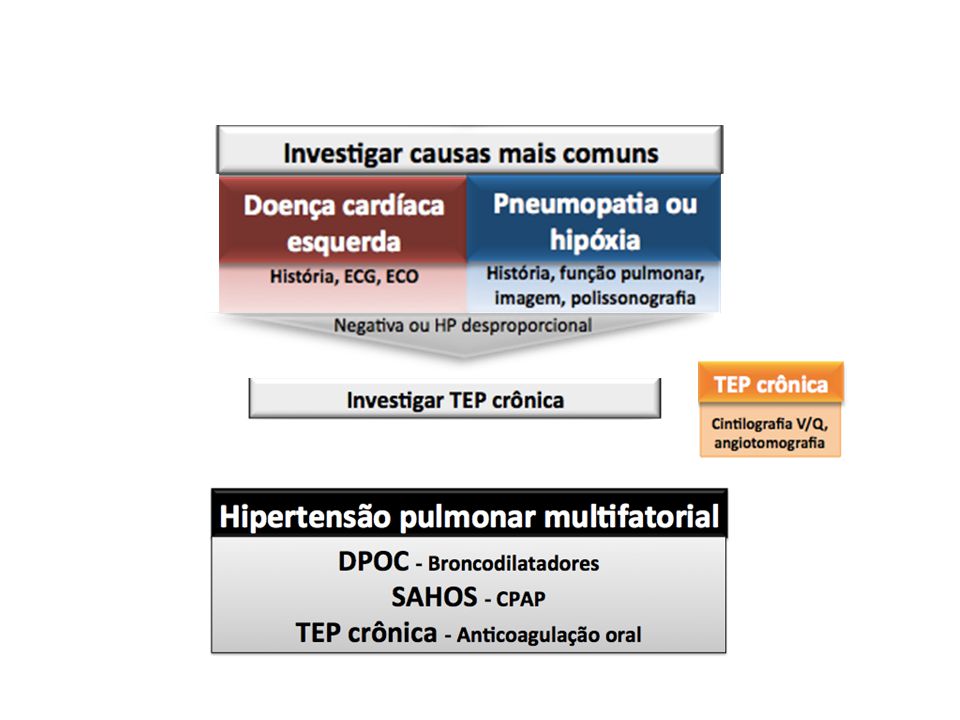
Investigação diagnóstica: sempre começar com as causas mais frequentes
I. Hipertensão arterial pulmonar HAP idiopática HAP hereditária Induzida por droga ou toxina Relacionadas a: Doença do colágeno HIV Cardiopatia congênita Hipertensão porto-pulmonar Esquistossomose Anemia hemolítica crônica HPPRN I’. Doença venooclusiva pulmonar Hemangiomatose capilar pulmonar II. HP dç cardíaca esquerda III. HP dç pulmonar/hipoxemia DPOC DIP Distúrbios do sono Altas altitudes Anormalidades de desenvolvimento IV. HP tromboembólica crônica V. HP miscelânea 4th World Symposium on Pulmonary Arterial Hypertension. Dana Point (Califórnia, 2008)
")
9
Investigação diagnóstica: sempre começar com as causas mais frequentes
I. Hipertensão arterial pulmonar HAP idiopática HAP hereditária Induzida por droga ou toxina Relacionadas a: Doença do colágeno HIV Cardiopatia congênita Hipertensão porto-pulmonar Esquistossomose Anemia hemolítica crônica HPPRN I’. Doença venooclusiva pulmonar Hemangiomatose capilar pulmonar II. HP dç cardíaca esquerda III. HP dç pulmonar/hipoxemia DPOC DIP Distúrbios do sono Altas altitudes Anormalidades de desenvolvimento IV. HP tromboembólica V. HP miscelânea 4th World Symposium on Pulmonary Arterial Hypertension. Dana Point (Califórnia, 2008)
")
10
Investigação diagnóstica

11
Ecocardiograma com sinais de HP
Although PH can only be con- firmed by means of a RHC, this test is only mandatory when therapeutic consequences are expected. for this reason, the diagnostic work-up does not start with performing a RHC, but with the exclusion of the most common causes of PH, repre- sented by WHO groups 2 and 3. The adapted diagnostic algo- rithm of the ERS/ESC guidelines for the diagnosis and treatment of PH is shown in figure 2.

12
Ecocardiograma com sinais de HP
PMAP ≥ 25 mmHg e Pressão oclusão de pulmonar > 15 mmHg Because left heart failure is characterised by increased filling pressures of the left ventricle (LV), the most characteristic hallmark of this disease is an increased wedge pressure. How- ever, in most cases of overt valvular heart failure and systolic left heart failure, echocardio- graphy will suffice. Perhaps the most difficult cause of PH to diagnose is PH secondary to diastolic heart failure (heart failure with preserved ejection fraction (HFPEF)). Clinical features that should raise suspicion of HFPEF are older age, obesity and a history of diabetes mellitus, atrial fibrillation or systemic hypertension. Signs of LV hypertrophy on ECG and an enlarged left atrium on echocardiography further increase the likelihood of this diagnosis. Although more advanced cardiac ultrasound techniques, such as strain imaging and determination of Doppler parameters of diastolic heart failure, frequently allow diagnosis of this disease, a right or left heart catheterisation is still required in many patients. In the current guidelines, a pulmonary artery wedge pressure or LV end-diastolic pressure greater than 15 mmHg is used to discriminate between pre-capillary (15 mmHg or lower) and post-capillary (more than 15 mmHg) PH. Given the decisive nature of wedge pressure in these cases, its accurate measurement is of paramount importance. Although in the past, excellent relationships between wedge pressures and LV end-diastolic pressures have been described, more recent reports challenge the accuracy of wedge pressure as a surrogate for LV end- diastolic pressure [6]. Methodological errors may underlie the inaccuracy. An example is given in figure 3. In addition, fluid volume conditions directly affect LV filling pressures and, therefore, wedge pressures. A patient with PH secondary to left heart failure may exhibit normal wedge pressures after appropriate or too vigorous treatment with diuretics. Withdrawal of diuretics and fluid loading may be required during heart catheterisation to determine the correct diagnosis. A standardised protocol and criteria for volume loading do not exist.
, the most characteristic hallmark of this disease is an increased wedge pressure. How- ever, in most cases of overt valvular heart failure and systolic left heart failure, echocardio- graphy will suffice. Perhaps the most difficult cause of PH to diagnose is PH secondary to diastolic heart failure (heart failure with preserved ejection fraction (HFPEF)). Clinical features that should raise suspicion of HFPEF are older age, obesity and a history of diabetes mellitus, atrial fibrillation or systemic hypertension. Signs of LV hypertrophy on ECG and an enlarged left atrium on echocardiography further increase the likelihood of this diagnosis. Although more advanced cardiac ultrasound techniques, such as strain imaging and determination of Doppler parameters of diastolic heart failure, frequently allow diagnosis of this disease, a right or left heart catheterisation is still required in many patients. In the current guidelines, a pulmonary artery wedge pressure or LV end-diastolic pressure greater than 15 mmHg is used to discriminate between pre-capillary (15 mmHg or lower) and post-capillary (more than 15 mmHg) PH. Given the decisive nature of wedge pressure in these cases, its accurate measurement is of paramount importance. Although in the past, excellent relationships between wedge pressures and LV end-diastolic pressures have been described, more recent reports challenge the accuracy of wedge pressure as a surrogate for LV end- diastolic pressure [6]. Methodological errors may underlie the inaccuracy. An example is given in figure 3. In addition, fluid volume conditions directly affect LV filling pressures and, therefore, wedge pressures. A patient with PH secondary to left heart failure may exhibit normal wedge pressures after appropriate or too vigorous treatment with diuretics. Withdrawal of diuretics and fluid loading may be required during heart catheterisation to determine the correct diagnosis. A standardised protocol and criteria for volume loading do not exist.")
13
Ecocardiograma com sinais de HP
PMAP ≥ 25 mmHg e Pressão oclusão de pulmonar > 15 mmHg Achados indiretos Clínicos Idade > 65 anos HAS Sd metabólica Obesidade Doença coronariana Diabetes Fibrilação atrial Ecocardiográficos Aumento do átrio esquerdo Hipertrofia do VE Remodelamento concêntrico do VE Aumento da pressão de enchimento do VE Outros Melhora com diurético Aumento significativo da PA com exercício RX compatível Because left heart failure is characterised by increased filling pressures of the left ventricle (LV), the most characteristic hallmark of this disease is an increased wedge pressure. How- ever, in most cases of overt valvular heart failure and systolic left heart failure, echocardio- graphy will suffice. Perhaps the most difficult cause of PH to diagnose is PH secondary to diastolic heart failure (heart failure with preserved ejection fraction (HFPEF)). Clinical features that should raise suspicion of HFPEF are older age, obesity and a history of diabetes mellitus, atrial fibrillation or systemic hypertension. Signs of LV hypertrophy on ECG and an enlarged left atrium on echocardiography further increase the likelihood of this diagnosis. Although more advanced cardiac ultrasound techniques, such as strain imaging and determination of Doppler parameters of diastolic heart failure, frequently allow diagnosis of this disease, a right or left heart catheterisation is still required in many patients. In the current guidelines, a pulmonary artery wedge pressure or LV end-diastolic pressure greater than 15 mmHg is used to discriminate between pre-capillary (15 mmHg or lower) and post-capillary (more than 15 mmHg) PH. Given the decisive nature of wedge pressure in these cases, its accurate measurement is of paramount importance. Although in the past, excellent relationships between wedge pressures and LV end-diastolic pressures have been described, more recent reports challenge the accuracy of wedge pressure as a surrogate for LV end- diastolic pressure [6]. Methodological errors may underlie the inaccuracy. An example is given in figure 3. In addition, fluid volume conditions directly affect LV filling pressures and, therefore, wedge pressures. A patient with PH secondary to left heart failure may exhibit normal wedge pressures after appropriate or too vigorous treatment with diuretics. Withdrawal of diuretics and fluid loading may be required during heart catheterisation to determine the correct diagnosis. A standardised protocol and criteria for volume loading do not exist. ERS Guidelines 2009
, the most characteristic hallmark of this disease is an increased wedge pressure. How- ever, in most cases of overt valvular heart failure and systolic left heart failure, echocardio- graphy will suffice. Perhaps the most difficult cause of PH to diagnose is PH secondary to diastolic heart failure (heart failure with preserved ejection fraction (HFPEF)). Clinical features that should raise suspicion of HFPEF are older age, obesity and a history of diabetes mellitus, atrial fibrillation or systemic hypertension. Signs of LV hypertrophy on ECG and an enlarged left atrium on echocardiography further increase the likelihood of this diagnosis. Although more advanced cardiac ultrasound techniques, such as strain imaging and determination of Doppler parameters of diastolic heart failure, frequently allow diagnosis of this disease, a right or left heart catheterisation is still required in many patients. In the current guidelines, a pulmonary artery wedge pressure or LV end-diastolic pressure greater than 15 mmHg is used to discriminate between pre-capillary (15 mmHg or lower) and post-capillary (more than 15 mmHg) PH. Given the decisive nature of wedge pressure in these cases, its accurate measurement is of paramount importance. Although in the past, excellent relationships between wedge pressures and LV end-diastolic pressures have been described, more recent reports challenge the accuracy of wedge pressure as a surrogate for LV end- diastolic pressure [6]. Methodological errors may underlie the inaccuracy. An example is given in figure 3. In addition, fluid volume conditions directly affect LV filling pressures and, therefore, wedge pressures. A patient with PH secondary to left heart failure may exhibit normal wedge pressures after appropriate or too vigorous treatment with diuretics. Withdrawal of diuretics and fluid loading may be required during heart catheterisation to determine the correct diagnosis. A standardised protocol and criteria for volume loading do not exist. ERS Guidelines")
14
Investigação diagnóstica
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços Investigação de dispneia Mulher, 30 anos Sem doenças prévias Rastreamento Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg FEVE 0,56 AE aumentado VD normal

15
Investigação diagnóstica
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços Investigação de dispneia Mulher, 30 anos Sem doenças prévias Rastreamento Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg FEVE 0,56 AE aumentado VD normal FEVE 0,75 AE normal VD aumentado FEVE 0,75 AE normal VD aumentado

16
Investigação diagnóstica
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços Investigação de dispneia Mulher, 30 anos Sem doenças prévias Rastreamento Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg FEVE 0,56 AE aumentado VD normal FEVE 0,75 AE normal VD aumentado FEVE 0,75 AE normal VD aumentado

17
HP do Grupo II (Pós-capilar)
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços É proporcional? PSAP= 50 mmHg FEVE 0,56 AE aumentado VD normal

18
HP do Grupo II (Pós-capilar): É proporcional?
Cateterismo cardíaco Resistência vascular Débito cardíaco PCP Gradiente transpulmonar (PAPm-PAE) Sobrecarga de volume Teste com diurético
 Sobrecarga de volume. Teste com diurético.")
19
Definição hemodinâmica da HP secundária à doença cardíaca esquerda
Características HP PMAP ≥ 25 mmHg HP pós-capilar PCP > 15 mmHg Passiva GTP ≤ 12 mmHg Fora de proporção (reativa) GTP > 12 mmHg Adir Y, Amir O. Eur Repir Monogr,
 GTP > 12 mmHg. Adir Y, Amir O. Eur Repir Monogr,")
20
Ecocardiograma com sinais de HP
É proporcional??? DPOC, BRONQUECTASIAS DOENÇAS INTERSTICIAIS SAOS DEFORMIDADES TORÁCICAS Although PH can only be con- firmed by means of a RHC, this test is only mandatory when therapeutic consequences are expected. for this reason, the diagnostic work-up does not start with performing a RHC, but with the exclusion of the most common causes of PH, repre- sented by WHO groups 2 and 3. The adapted diagnostic algo- rithm of the ERS/ESC guidelines for the diagnosis and treatment of PH is shown in figure 2.

21
HP associada à doença respiratória: O que é HP proporcional???
PMAP até 35 mmHg ou 40 mmHg Thabut, Chest, 2005. Chaouat, Am J Respir Crit Care Med, 2005 Outra sugestão: Utilização de dois critérios presença de qualquer hipertensão pulmonar em pacientes com doença respiratória leve ou moderada (VEF1>50% prev) PMAP ≥ 40 mmHg, independentemente da gravidade da doença respiratória Although PH can only be con- firmed by means of a RHC, this test is only mandatory when therapeutic consequences are expected. for this reason, the diagnostic work-up does not start with performing a RHC, but with the exclusion of the most common causes of PH, repre- sented by WHO groups 2 and 3. The adapted diagnostic algo- rithm of the ERS/ESC guidelines for the diagnosis and treatment of PH is shown in figure 2. Chaouat, A., Minai, O.A.. Eur Repir Monogr,
 PMAP ≥ 40 mmHg, independentemente da gravidade da doença respiratória. Although PH can only be con- firmed by means of a RHC, this test is only mandatory when therapeutic consequences are expected. for this reason, the diagnostic work-up does not start with performing a RHC, but with the exclusion of the most common causes of PH, repre- sented by WHO groups 2 and 3. The adapted diagnostic algo- rithm of the ERS/ESC guidelines for the diagnosis and treatment of PH is shown in figure 2. Chaouat, A., Minai, O.A.. Eur Repir Monogr,")
22
Pulmonary hypertension (PH) is a progressive disease with a poor prognosis. Identifying chronic thromboembolic pulmonary disease as a cause of PH has major clinical implications as these patients could be potentially offered a surgical cure. Ventilation–perfusion (V/Q) scintigraphy has a high sensitivity to detect embolic disease but its value has been challenged with the emergence of multidetector CT pulmonary angiography (CTPA). We compared the value of V/Q scintigraphy with CTPA in detecting chronic thromboembolic pulmonary disease. Methods: We retrospectively reviewed the results of V/Q scintigraphy and CTPA performed on patients who had been referred to the Pulmonary Hypertension Service at Hammersmith Hospital between 2000 and A total of 227 patients (85 males, 142 females; age range, 18–81 y; mean age, 42 y) had all tests done at Hammersmith Hospital and were included in the study. Interpretation of scans was according to the modified PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) criteria. CTPA was considered as suggestive of chronic thromboembolic pulmonary disease if it showed visualization of the thrombus or webs, recanalization, perfusion abnormalities, stenosis, or strictures. Standard pulmonary angiography was performed via femoral approach. In 90% of the cases, CTPA and V/Q scintigraphy were performed within 10 d. Results: Seventy-eight patients (group A) had a final diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) and 149 (group B) had non-CTEPH etiology. Among group A, V/Q scintigraphy was reported as high probability in 75 patients, intermediate probability in 1 patient, and low probability in 2 patients. CTPA was positive in 40 patients and negative in 38 patients. Among group B, V/Q scintigraphy was reported as low probability in 134, intermediate probability in 7, and high probability in 8 patients. CTPA was negative in 148 patients and false-positive in 1 patient. Statistical analysis showed V/Q scintigraphy to have a sensitivity of 96%–97.4% and a specificity of 90%–95%. CTPA showed a sensitivity of 51% and a specificity of 99%. Conclusion: Our results demonstrate that V/Q scintigraphy has a higher sensitivity than CTPA in detecting CTEPH as a potential curable cause of PH.
 scintigraphy has a high sensitivity to detect embolic disease but its value has been challenged with the emergence of multidetector CT pulmonary angiography (CTPA). We compared the value of V/Q scintigraphy with CTPA in detecting chronic thromboembolic pulmonary disease. Methods: We retrospectively reviewed the results of V/Q scintigraphy and CTPA performed on patients who had been referred to the Pulmonary Hypertension Service at Hammersmith Hospital between 2000 and A total of 227 patients (85 males, 142 females; age range, 18–81 y; mean age, 42 y) had all tests done at Hammersmith Hospital and were included in the study. Interpretation of scans was according to the modified PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) criteria. CTPA was considered as suggestive of chronic thromboembolic pulmonary disease if it showed visualization of the thrombus or webs, recanalization, perfusion abnormalities, stenosis, or strictures. Standard pulmonary angiography was performed via femoral approach. In 90% of the cases, CTPA and V/Q scintigraphy were performed within 10 d. Results: Seventy-eight patients (group A) had a final diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) and 149 (group B) had non-CTEPH etiology. Among group A, V/Q scintigraphy was reported as high probability in 75 patients, intermediate probability in 1 patient, and low probability in 2 patients. CTPA was positive in 40 patients and negative in 38 patients. Among group B, V/Q scintigraphy was reported as low probability in 134, intermediate probability in 7, and high probability in 8 patients. CTPA was negative in 148 patients and false-positive in 1 patient. Statistical analysis showed V/Q scintigraphy to have a sensitivity of 96%–97.4% and a specificity of 90%–95%. CTPA showed a sensitivity of 51% and a specificity of 99%. Conclusion: Our results demonstrate that V/Q scintigraphy has a higher sensitivity than CTPA in detecting CTEPH as a potential curable cause of PH..")
23
Pulmonary hypertension (PH) is a progressive disease with a poor prognosis. Identifying chronic thromboembolic pulmonary disease as a cause of PH has major clinical implications as these patients could be potentially offered a surgical cure. Ventilation–perfusion (V/Q) scintigraphy has a high sensitivity to detect embolic disease but its value has been challenged with the emergence of multidetector CT pulmonary angiography (CTPA). We compared the value of V/Q scintigraphy with CTPA in detecting chronic thromboembolic pulmonary disease. Methods: We retrospectively reviewed the results of V/Q scintigraphy and CTPA performed on patients who had been referred to the Pulmonary Hypertension Service at Hammersmith Hospital between 2000 and A total of 227 patients (85 males, 142 females; age range, 18–81 y; mean age, 42 y) had all tests done at Hammersmith Hospital and were included in the study. Interpretation of scans was according to the modified PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) criteria. CTPA was considered as suggestive of chronic thromboembolic pulmonary disease if it showed visualization of the thrombus or webs, recanalization, perfusion abnormalities, stenosis, or strictures. Standard pulmonary angiography was performed via femoral approach. In 90% of the cases, CTPA and V/Q scintigraphy were performed within 10 d. Results: Seventy-eight patients (group A) had a final diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) and 149 (group B) had non-CTEPH etiology. Among group A, V/Q scintigraphy was reported as high probability in 75 patients, intermediate probability in 1 patient, and low probability in 2 patients. CTPA was positive in 40 patients and negative in 38 patients. Among group B, V/Q scintigraphy was reported as low probability in 134, intermediate probability in 7, and high probability in 8 patients. CTPA was negative in 148 patients and false-positive in 1 patient. Statistical analysis showed V/Q scintigraphy to have a sensitivity of 96%–97.4% and a specificity of 90%–95%. CTPA showed a sensitivity of 51% and a specificity of 99%. Conclusion: Our results demonstrate that V/Q scintigraphy has a higher sensitivity than CTPA in detecting CTEPH as a potential curable cause of PH. Tunariu N, J Nucl Med 2007

24
Cintilografia pulmonar de perfusão
TEP crônico: falhas de enchimento segmentares, grandes e usualmente bilaterais, com a cintilografia de inalação normal Hipertensão Pulmonar Idiopática: cintilo geralmente é normal, ou apresenta falhas de enchimento pequenas e subsegmentares Dartevelle P et al. Chronic thromboembolic pulmonary hypertension. Eur Respir J 2004; 23:

26
Investigação diagnóstica
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços Investigação de dispneia Mulher, 30 anos Sem doenças prévias Rastreamento Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg Espirometria normal Negativa para SAOS Exames de imagem sem alterações

27
Investigação diagnóstica
Achado Incidental 65 anos HAS, DM, Dispneia aos medios esforços Investigação de dispneia Mulher, 30 anos Sem doenças prévias Rastreamento Mulher, 40 anos Cirrose HepB Candidata TX Sem sintomas PSAP= 50 mmHg PSAP= 50 mmHg PSAP= 50 mmHg Cinitilografia normal

28
Ecocardiograma com sinais de HP

29
Investigação diagnóstica
Cateterismo – PAPm ≥ 25 mmHg & Confirmação diagnóstica de HP arterial (PCP<15 mmHg) Teste de vasorreatividade Avaliação de gravidade Avaliação de resposta ao tratamento Avaliação hemodinâmica no TEP crônico Outras situações: Tx hepático
 Teste de vasorreatividade. Avaliação de gravidade. Avaliação de resposta ao tratamento. Avaliação hemodinâmica no TEP crônico. Outras situações: Tx hepático.")
30
PAP = PcapP + (DC X RVP) PAP (mmHg) 60/20 (35)
 PAP (mmHg) 60/20 (35)")
31
PAP = PcapP + (DC X RVP) PAP (mmHg) 60/20 (35) HAPI DPOC DVE
Crise tireotóxica

32
PAP = PcapP + (DC X RVP) PAP (mmHg) Pcap (mmHg) DC (L/m) RVP (UW)
60/20 (35) HAPI 10 3 6,2 DPOC DVE 20 5 Crise tireotóxica 15 2
 HAPI ,2. DPOC. DVE Crise tireotóxica")
33
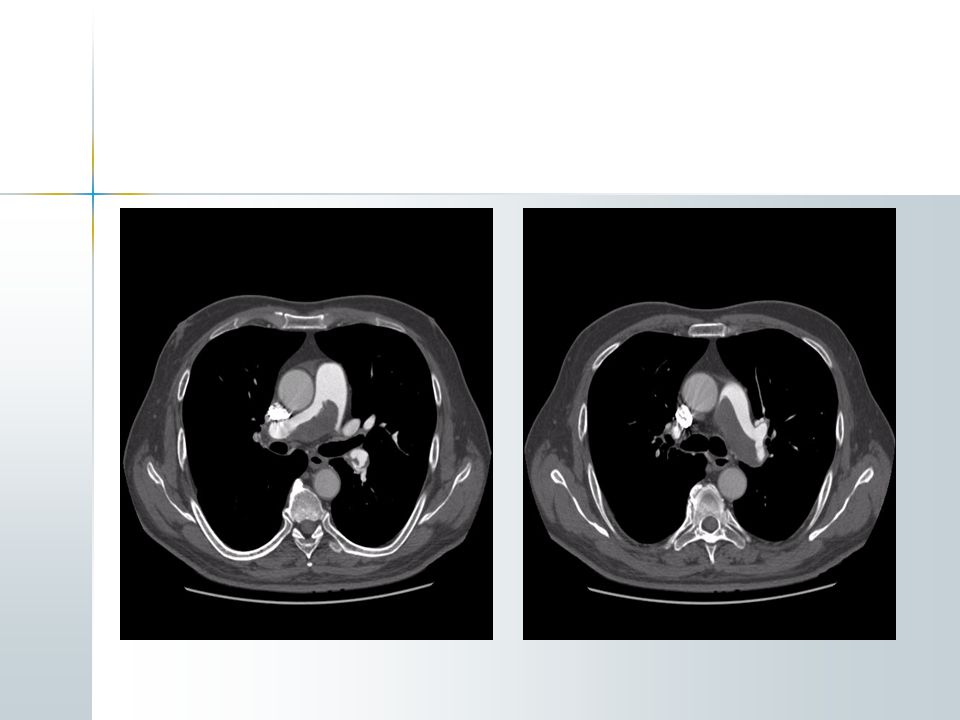
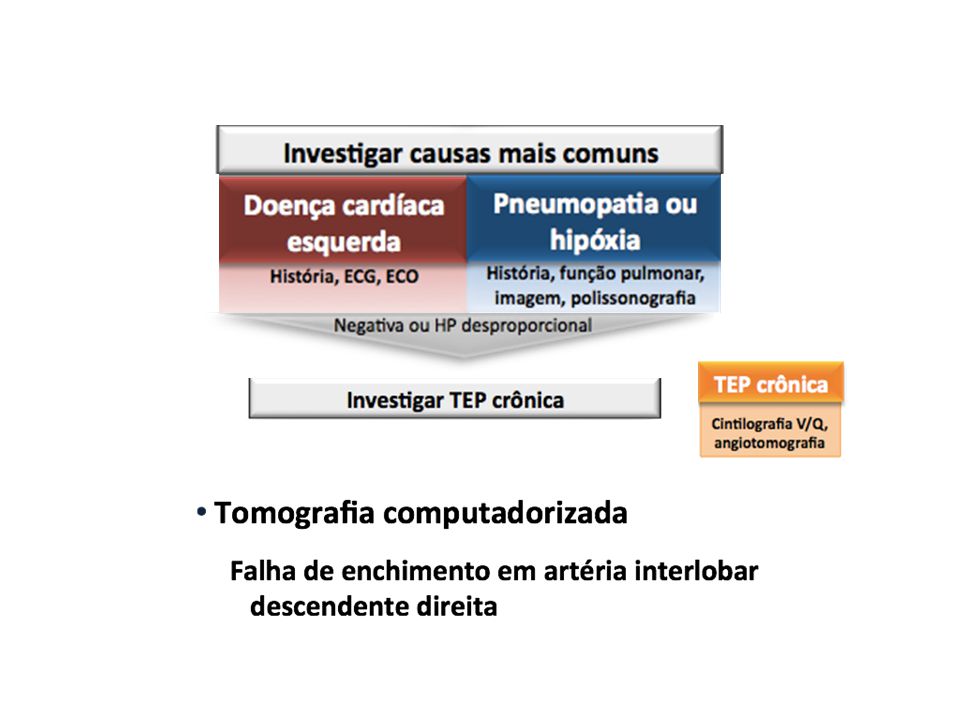
Investigação diagnóstica
Caso clínico Investigação diagnóstica 55 anos, masculino, natural de SP DPOC há 5 anos, usa formoterol 2x/dia Piora da dispneia no último ano; Teve duas exacerbaçoes no período, tratadas como infecções respiratórias

34
Investigação diagnóstica
Caso clínico Investigação diagnóstica Dispneia aos moderados esforços (MRC3) Pré-síncope, edema periférico Presença de roncos noturnos Sem outras comorbidades Cessou tabagismo há 3 anos (40 anos-maço)
 Pré-síncope, edema periférico. Presença de roncos noturnos. Sem outras comorbidades. Cessou tabagismo há 3 anos (40 anos-maço)")
35
Investigação diagnóstica
Movimento paradoxal do septo interventricular Ausência de derrame pericárdico ou pleural

40
Realizar exames para os diversos diagnósticos de HAP (grupo 1)
Sinais, sintomas, historia sugestiva de HP Avaliação não invasiva compatível com HP? Sim Excluir doença cardíaca esquerda Excluir doença pulmonar parenquimatosa, de vias aéreas e outras condições hipóxicas Excluir HPTEC Realizar exames para os diversos diagnósticos de HAP (grupo 1) Realizar CAT direito para confirmar o diagnóstico
 Realizar CAT direito para confirmar o diagnóstico.")
41
Caros Colegas Reservem em sua agenda o período de 14 a 17 de novembro de 2013 para participar do tradicional congresso regional da pneumologia brasileira. O site do 15°Congresso Paulista de Pneumologia e Tisiologia já está no ar!

Apresentações semelhantes