Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Manejo Clínico-Terapêutico e Pesquisa em Pacientes Multi-Experimentados à TARV
Seminário do Programa Franco-Brasileiro de AIDS. Fortaleza-Ce, Brasil. 22 a 24 de novembro de 2006. Érico Arruda. Diretor Clínico do Hospital São José de Doenças Infecciosas. Membro dos Comitês de Terapia Anti-retroviral de Adultos e Adolescentes e de Genotipagem do HIV do PN-DST/AIDS.

2
Drogas Anti-Retrovirais Aprovadas pelo FDA e ANVISA
ITRNs IPs Amprenavir (APV) descontinuado 2004 Atazanavir (ATV) Darunavir (DRV) Fosamprenavir (FPV) Indinavir (IDV) Lopinavir/ritonavir (LPV/RTV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV hgc) Tipranavir (TPV) Abacavir (ABC) Didanosina (ddI) Estavudina (d4T) Emtricitabina (FTC) Lamivudina (3TC) Tenofovir (TDF) Zalcitabina (ddC) descontinuado Zidovudina (ZDV) 3TC/ABC 3TC/ABC/ZDV 3TC/ZDV FTC/TDF I will start by reviewing the drugs that have been approved by the US Food and Drug Administration (FDA) for the treatment of HIV therapy. In 2006, we have 21 agents that are available for treatment regimens. There are 8 in the NRTI class, 3 in the NNRTI class, 1 fusion inhibitor, and 10 in the protease inhibitor class that are approved by the FDA. Amprenavir has been withdrawn from the market because the prodrug of amprenavir, fosamprenavir, has been approved and is available. There are also a number of fixed-dose formulations that encompass the 3 class of agents, except the fusion inhibitors. Inibidores de Fusão (IFs) Enfuvirtida (ENF) ITRNNs Combinação Multi-Class Delavirdina (DLV) descontinuado Efavirenz (EFV) Nevirapina (NVP) EFV/FTC/TDF
 descontinuado Atazanavir (ATV) Darunavir (DRV) Fosamprenavir (FPV) Indinavir (IDV) Lopinavir/ritonavir (LPV/RTV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV hgc) Tipranavir (TPV) Abacavir (ABC) Didanosina (ddI) Estavudina (d4T) Emtricitabina (FTC) Lamivudina (3TC) Tenofovir (TDF) Zalcitabina (ddC) descontinuado. Zidovudina (ZDV) 3TC/ABC. 3TC/ABC/ZDV. 3TC/ZDV. FTC/TDF. I will start by reviewing the drugs that have been approved by the US Food and Drug Administration (FDA) for the treatment of HIV therapy. In 2006, we have 21 agents that are available for treatment regimens. There are 8 in the NRTI class, 3 in the NNRTI class, 1 fusion inhibitor, and 10 in the protease inhibitor class that are approved by the FDA. Amprenavir has been withdrawn from the market because the prodrug of amprenavir, fosamprenavir, has been approved and is available. There are also a number of fixed-dose formulations that encompass the 3 class of agents, except the fusion inhibitors. Inibidores de Fusão (IFs) Enfuvirtida (ENF) ITRNNs. Combinação Multi-Class. Delavirdina (DLV) descontinuado. Efavirenz (EFV) Nevirapina (NVP) EFV/FTC/TDF.")
4
Coeficiente de Mortalidade por AIDS
Brasil, 0,00 2,00 4,00 6,00 8,00 10,00 12,00 90 91 92 93 94 95 96 97 98 99 Ano do óbito (por hab) Fonte: SIM/DATASUS
 Fonte: SIM/DATASUS.")
5
% com CV < 50 cópias/ml na 48a. semana
Resultados de estudos com HAART para pcts. virgens de TARV IP ITRNN ITRN IP-r 10 20 30 40 50 60 70 80 90 100 % com CV < 50 cópias/ml na 48a. semana Bartlett et al. 12th CROI, February Abstract 586.

6
Prevalência de resistência em 40 Cidades dos EUA em 2003 em pacientes naïve de TARV
Realizado FT/GT GT: 14% com mutação Sensibilidade reduzida é mais prevalente com a classe de ITRNN % com reduzida sensibilidade a qualquer droga 20 16 12 % Pacientes com Sensibilidade reduzida 8 Demographics Mean age years % male 92% Mean CD4+ (copies/mL) 277 Race White 55% Black 33% Hispanic/Asian/other 12% HIV-1 clade B 97% Transmission route Homosexual 74% Heterosexual 28% Iv use/transfusion/other 6% PUT SPECIFIC MUTATIONS IN NOTES 4 d4T ZDV DLV EFV NVP APV IDV NFV RTV SQV Ross L, et al. 44th ICAAC, Washington 2004, #H-173
 277. Race. White 55% Black 33% Hispanic/Asian/other 12% HIV-1 clade B 97% Transmission route. Homosexual 74% Heterosexual 28% Iv use/transfusion/other 6% PUT SPECIFIC MUTATIONS IN NOTES. 4. d4T. ZDV. DLV. EFV. NVP. APV. IDV. NFV. RTV. SQV. Ross L, et al. 44th ICAAC, Washington 2004, #H-173.")
7
Fatores associados à detecção de resistência
Risco de desenvolvimento de resistência após início de terapia na prática clínica Fatores associados à detecção de resistência Risco 95% IC Idade (p/incr de 10 a) CV>105 c/ml Diag. de AIDS 0.82 1.36 1.38 2 ITRNs com: IP IP-r ABC ITRNN 0.7 1.95 1.0 UK CHIC Study (n= 4.306) Coorte de 6 clínicas em Londres; Terapia ARV iniciada com 2 ITRN mais um terceiro agente. Risco total de falha terapêutica foi de 38% durante 6 anos. Risco de acúmulo de mutações de resistência para qualquer droga foi de 27% no total. % de resistência Tempo para Falha a Múltiplas Drogas Phillips, A et all. AIDS, :5,
 CV>105 c/ml. Diag. de AIDS ITRNs com: IP. IP-r. ABC. ITRNN UK CHIC Study (n= 4.306) Coorte de 6 clínicas em Londres; Terapia ARV iniciada com 2 ITRN mais um terceiro agente. Risco total de falha terapêutica foi de 38% durante 6 anos. Risco de acúmulo de mutações de resistência para qualquer droga foi de 27% no total. % de resistência. Tempo para Falha a Múltiplas Drogas. Phillips, A et all. AIDS, :5,")
8
Epidemiologia de resistência aos anti-retrovirais
Prevalência de resistência em pacientes ART-naïve no UK (n=2.410) Prevalência de resistência varia com a definição usada Prevalência de Resistência a drogas em pacientes naïve por ano: dados do RU (UK) Prevalência de resistência pela IAS e Algoritmo de Stanford 5 10 15 20 25 1996-7 1998 1999 2000 2001 2002-3 Amostras por ano Prevalência (%) 316 312 360 453 502 467 ITRN ITRNN PI Qualq classe Prevalência (%) Pillay D, et al. HIV 7, Glasgow 2004, #PL5.3
 Prevalência de resistência varia com a definição usada. Prevalência de Resistência a drogas em pacientes naïve por ano: dados do RU (UK) Prevalência de resistência pela IAS e Algoritmo de Stanford Amostras por ano. Prevalência (%) ITRN. ITRNN. PI. Qualq classe. Prevalência (%) Pillay D, et al. HIV 7, Glasgow 2004, #PL5.3.")
9
Primary Resistance in Santos, Brazil
Sucupira et al, AIDS Patient Care and STDs, in press.

11
Resposta ao Tratamento no 1º
Resposta ao Tratamento no 1º. Ano de HAART – Melhora com o Decorrer do Tempo 4.143 pacientes de 5 coortes da Europa e Canadá Virgens de tratamento, início de HAART de 1996 a 2002 ↓ risco de falha virológica, ↑ da média de CD4 nos últimos anos Atualmente a maioria das “falhas” ocorre por perda de acompanhamento ou interrupção do tratamento 15 30 45 60 75 90 105 120 135 150 Aumento da Mediana CD4+ 97 119 121 127 125 Aumento da Mediana de CD4+ 100 % com > 500 cópias/ml 90 80 70 60 % com CV > 500 em TARV 50 40 30 24.8 23.0 20 17.3 12.4 10 10 8 8.4 1996 1997 1998 1999 2000 2001 2002 Lampe S, et al. 12th CROI, 2005, Abstract 593

12
Causas de Falha Vírus Droga Paciente Alta taxa de replicação viral
Alta taxa de mutação resistência Reservatórios “latentes” do HIV Potência Absorção Farmacocinética Reservatórios Metabolização Toxicidade Incoveniências posológicas Interações medicamentosas Vírus Droga Paciente Tolerância Adesão Acesso à medicação Estágio da doença

13
Caminho da resistência e falha terapêutica
HIV Variantes resistentes Pré-existentes Transmitidos Polimorfismo Níveis sub-inibitórios das drogas ARV Falha imunológica do hospedeiro Replicação persistente do HIV Evolução para resistência Falha terapêutica Hirsch, et al. JAMA 1998; 279:1984.

14
Viremia e progressão Rápida Lenta Carga viral detectável
na presença do inibidor alta baixa Rápida Lenta Resistência CD4 diminui e doença progride

15
Proporção sem falha imunológica
Falha imunológica após falha virológica 1.0 0.8 0.6 Proporção sem falha imunológica 0.4 0.2 0.0 6 12 18 24 30 36 42 Meses após o início da falha virológica Deeks et al. AIDS 2002; 16:

16
Supressão virológica e sobrevida
% com CV detectável (0-18 meses após início de HAART) 0.25 100% 0.20 51% - 75% 76% - 99% 0.15 Mortalidade cumulativa 26% - 50% 1% - 25% 0.10 0% 0.05 0.00 18 36 54 72 Meses após o basal (basal foi 18 meses após início da HAART) Lohse et al. CID 2006; 42:136-44
 % % - 75% 76% - 99% Mortalidade cumulativa. 26% - 50% 1% - 25% % Meses após o basal (basal foi 18 meses após início da HAART) Lohse et al. CID 2006; 42:")
17
Progressão aumentada em resistência a múltiplas classes
1.0 0.9 0 RAC 1 RAC 0.8 Proporção cumulativa de sobrevida 2 RAC 0.7 3 RAC 0.6 10 20 30 40 50 60 Meses após teste de resistência Zaccarelli et al. AIDS 2005; 19:1081–1089 RAC = resistência ampla à classe

18
Probabilidade de sobrevida livre de evento (Morte)
Pacientes com Resistência a 3-classes e múltiplas falhas: Progressão Clínica com Terapia de Resgate (OPTIMA trial) Probabilidade de sobrevida (Cox model) Média de CD4: 134/mm3 Probabilidade de sobrevida livre de evento (AIDS ou morte) Probabilidade de sobrevida livre de evento (Morte) Resposta de CV (log10 c/ml) Resposta de CV (log10 c/ml) 1.0 1.0 1 - 2 log > 2 log 0.8 0.8 > 2 log 0.6 1 - 2 log 0.6 < 1 log Conclusion : Chez des patients SIDA en multi-échec et avec multi-résistance, la réponse virologique au traitement de sauvetage est associée à une diminution du risque de progression et de mortalité. Une réponse virologique > 1 log10 c/ml est associée à une amélioration du pronostic. Données importantes, dans la mesure où les essais cliniques dans cette population ont des critères de jugement virologiques et non cliniques. Cette étude apporte donc des informations complémentaires très contributives. 0.4 0.4 < 1 log 0.2 0.2 p < 0,001 p < 0,001 6 12 18 24 30 36 6 12 18 24 30 36 meses meses Angus B., EACS 2005, Abs. PS7.4/6
 Probabilidade de sobrevida (Cox model) Média de CD4: 134/mm3. Probabilidade de sobrevida livre de evento (AIDS ou morte) Probabilidade de sobrevida livre de evento (Morte) Resposta de CV (log10 c/ml) Resposta de CV (log10 c/ml) log. > 2 log > 2 log log < 1 log. Conclusion : Chez des patients SIDA en multi-échec et avec multi-résistance, la réponse virologique au traitement de sauvetage est associée à une diminution du risque de progression et de mortalité. Une réponse virologique > 1 log10 c/ml est associée à une amélioration du pronostic. Données importantes, dans la mesure où les essais cliniques dans cette population ont des critères de jugement virologiques et non cliniques. Cette étude apporte donc des informations complémentaires très contributives < 1 log p < 0,001. p < 0, meses. meses. Angus B., EACS 2005, Abs. PS7.4/6.")
19
% de pacientes com CV <400 cópias/ml
Relação da adesão com o sucesso terapêutico Adesão > 95% 90 80 70 60 % de pacientes com CV <400 cópias/ml 50 40 >95 90–95 80–90 70–80 <70 30 20 10 Razão de Aderência (MEMS) Paterson et al. Ann Intern Med. 2000;133:21-30
 Paterson et al. Ann Intern Med. 2000;133:")
21
Considerações Gerais Estratégias atuais para pacientes experimentados em TARV Metas para a terapia Considerações sobre resistência Use de drogas recentemente aprovadas Novas drogas em desenvolvimento

22
Quando usar Teste de Resistência
IAS-EUA[1] DHHS-EUA[2] Europeu[3] Primária/aguda Recomendado Profilaxia Pós-exposicional — Crônica, Rx naive Considerar* Considerar Fortemente* Falha Gravidez Pediatria DHHS, US Department of Health and Human Services; IAS-USA, International AIDS Society-USA; Rx, treatment. Three major organizations provide resistance testing guidelines: the International AIDS Society (IAS)-USA, the US Department of Health and Human Services (DHHS), and the European HIV Drug Resistance Panel. In general, these organizations agree about when resistance testing should be done. All agree that it should be done in primary or acute infection. The European guidelines recommend resistance testing in postexposure prophylaxis, for treatment failure, and during pregnancy. However, there is some disagreement about resistance testing in chronically infected, treatment-naive patients. In recent changes to the DHHS guidelines (5/4/06), resistance testing is recommended for these patients. According to IAS‑USA, resistance testing is indicated only if the background rate of resistance is ≥ 5% or, according to the European guidelines, ≥ 10%. However, these guidelines are under review and are likely to be revised. *Especialmente se a exposição se deu de alguém que recebe drogas anti-retrovirais ou se a prevalência de resistência em pacientes não tratados é ≥ 5% (Europeu se ≥ 10%). 1. Hirsch MS, et al. Clin Infect Dis. 2003;37: 2. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de 2006. 3. Vandamme AM, et al. Antivir Ther. 2004;9:
-USA, the US Department of Health and Human Services (DHHS), and the European HIV Drug Resistance Panel. In general, these organizations agree about when resistance testing should be done. All agree that it should be done in primary or acute infection. The European guidelines recommend resistance testing in postexposure prophylaxis, for treatment failure, and during pregnancy. However, there is some disagreement about resistance testing in chronically infected, treatment-naive patients. In recent changes to the DHHS guidelines (5/4/06), resistance testing is recommended for these patients. According to IAS‑USA, resistance testing is indicated only if the background rate of resistance is ≥ 5% or, according to the European guidelines, ≥ 10%. However, these guidelines are under review and are likely to be revised. *Especialmente se a exposição se deu de alguém que recebe drogas anti-retrovirais ou se a prevalência de resistência em pacientes não tratados é ≥ 5% (Europeu se ≥ 10%). 1. Hirsch MS, et al. Clin Infect Dis. 2003;37: Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de Vandamme AM, et al. Antivir Ther. 2004;9:")
23
Guidelines for new ARV regimen (France, 2006)
Virologic failure Guidelines for new ARV regimen (France, 2006) Virologic failure and/or resistance to ARV combinations usually recommended NRTI(s) and NNRTI 2 NRTI (guided by genotype) + PI/r NRTI(s) and PI/r Preferred options Alternative option (especially if ≥ 3rd virologic failure) 2 NRTI + (ATV/r or fAPV/r or LPV/r or SQV/r), according to genotype 2 NRTI (guided by genotype) + NNRTI (the 2 NRTI need to be fully active) 2 NRTI (guided by genotype) + (fAPV/r or LPV/r) + NNRTI (TDM mandatory) NRTI(s) and NNRTI and PI/r Enfuvirtide + PI/r ± NRTI (based on actual and historical genotypes ) Selection of PI/r : active PI/r (genotype) ; TPV/r, to be preferred, or DRV/r, if resistance or possible resistance to other PI/r Dans les situations d’antériorité thérapeutique aux 3 classes et de multirésistance, l’utilisation de deux IP/r actifs peut être également discutée. Recommandations du groupe d’experts, Yéni P et al. Flammarion 2006
 Virologic failure and/or resistance to. ARV combinations usually recommended. NRTI(s) and NNRTI. 2 NRTI (guided by genotype) + PI/r. NRTI(s) and PI/r. Preferred options. Alternative option (especially if ≥ 3rd virologic failure) 2 NRTI + (ATV/r or fAPV/r or LPV/r or SQV/r), according to genotype. 2 NRTI (guided by genotype) + NNRTI (the 2 NRTI need to be fully active) 2 NRTI (guided by genotype) + (fAPV/r or LPV/r) + NNRTI (TDM mandatory) NRTI(s) and NNRTI and PI/r. Enfuvirtide + PI/r ± NRTI (based on actual and historical genotypes ) Selection of PI/r : active PI/r (genotype) ; TPV/r, to be preferred, or DRV/r, if resistance or possible resistance to other PI/r. Dans les situations d’antériorité thérapeutique aux 3 classes et de multirésistance, l’utilisation de deux IP/r actifs peut être également discutée. Recommandations du groupe d’experts, Yéni P et al. Flammarion")
24
Critérios para realização de Exame de Genotipagem no Brasil pelo PN-DST/Aids
1- Pacientes em uso regular de TARV há pelo menos 6 meses e com carga viral (CV) detectável acima de cópias/ml. 2- Gestantes em uso regular de TARV há pelo menos 3 meses e com CV acima de cópias/ml. 3- Pacientes candidatos ao uso de Enfuvirtida (T-20)”, desde que haja possibilidade de sua composição com pelo menos uma droga ativa. Não está indicada a genotipagem para pacientes nas seguintes situações: 1- Não-adesão ao tratamento (CV > cópias/ml sugere presença de cepa selvagem); 2- CV < cópias/ml; 3- Genotipagem anterior demonstrando ausência de drogas capazes de compor esquema eficaz com Enfuvirtida. Disponível em: Acessada em 15 de novembro de 2006.
 detectável acima de cópias/ml. 2- Gestantes em uso regular de TARV há pelo menos 3 meses e com CV acima de cópias/ml. 3- Pacientes candidatos ao uso de Enfuvirtida (T-20) , desde que haja possibilidade de sua composição com pelo menos uma droga ativa. Não está indicada a genotipagem para pacientes nas seguintes situações: 1- Não-adesão ao tratamento (CV > cópias/ml sugere presença de cepa selvagem); 2- CV < cópias/ml; 3- Genotipagem anterior demonstrando ausência de drogas capazes de compor esquema eficaz com Enfuvirtida. Disponível em: Acessada em 15 de novembro de")
25
Uso do teste de resistência associado a maior sobrevida
HOPS Coorte: pacientes que passaram por testes de resistência comparados com pacientes em que o teste não foi realizado Comparação adicional de casos pareados – 151 pacientes virêmicos e em tratamento que faleceram X 151 que sobreviveram, ajustado por: Contagem de CD4+ (nadir) Intervalo de contagem de CD4+ Seguro/convênio privado Risco relativo para óbito: 0,31 para pacientes que tiveram mais do que um teste de resistência (p < 0,001) Pode indicar melhora na qualidade do tratamento vs efeito do teste de resistência Fatores independentes preditivos de morte na coorte (N = 4.614) Fator RR Teste de resistência para HIV 0,41* Seguro ou convênio privados 0,55* Raça branca 0,65* > 40 anos de idade no nadir de CD4+ 1,37† Nadir de CD cél/mm3 2,41* Nadir de CD4+ < 50 cél/mm3 5,73* For more information, please see the Capsule Summary at *p < 0,01 †p < 0,05 Palella F, et al. CROI Abstract 654.
 Intervalo de contagem de CD4+ Seguro/convênio privado. Risco relativo para óbito: 0,31 para pacientes que tiveram mais do que um teste de resistência (p < 0,001) Pode indicar melhora na qualidade do tratamento vs efeito do teste de resistência. Fatores independentes preditivos de morte na coorte. (N = 4.614) Fator. RR. Teste de resistência para HIV. 0,41* Seguro ou convênio privados. 0,55* Raça branca. 0,65* > 40 anos de idade no nadir de CD4+ 1,37† Nadir de CD cél/mm3. 2,41* Nadir de CD4+ < 50 cél/mm3. 5,73* For more information, please see the Capsule Summary at *p < 0,01. †p < 0,05. Palella F, et al. CROI Abstract 654.")
26
Único teste de Genotipagem subestima resistência
Genotipagem Anterior Genotipagem mais recente Diferença Lamivudina (M184V/I) 58.8% 25.5% 33.3% Outros ITRN 46.0% 27.7% 18.3% ITRNN 38.5% 24.5% 14.0% IP 27.9% 15.6% 12.3% Harrigan et al., Infect Dis ;191(8):1325–30.
 58.8% 25.5% 33.3% Outros ITRN. 46.0% 27.7% 18.3% ITRNN. 38.5% 24.5% 14.0% IP. 27.9% 15.6% 12.3% Harrigan et al., Infect Dis ;191(8):1325–30.")
27
RENAGENO: Rede Nacional de Genotipagem
Em 2001, o PN-DST/Aids, implantou a Rede Nacional de Genotipagem: 21 Laboratórios em 12 estados da federação. 365 médicos de referência treinados (inclusive pediatras). Aproximadamente exames realizados. Fonte: Unidade de Laboratório do PN-DST/AIDS.
. Aproximadamente exames realizados. Fonte: Unidade de Laboratório do PN-DST/AIDS.")
28
Melissa Soares Medeiros
GENOTIPAGEM E PERFIL DE RESISTÊNCIA AOS ANTI-RETROVIRAIS DO VÍRUS DA IMUNODEFICIÊNCIA TIPO 1 EM ISOLADOS DE POPULAÇÃO COM FALHA TERAPÊUTICA NO CEARÁ, BRASIL – 2002 A 2004 Melissa Soares Medeiros Orientador: Prof. Dr. Aldo Ângelo Moreira Lima Co-Orientador: Dr. Érico Antonio Gomes de Arruda

29
Caracterização Epidemiológica, Clínicas e Imuno-Virológica da População em Estudo (N = 101).
Característica Valores (%) Sexo Masculino Feminino 77 (76,2%) 24 (23,8%) Idade Mediana = 38 anos (variação 6-66) Data do diagnóstico de HIV Julho/81 a Setembro/02 Doença Definidora de AIDS Pacientes Sintomáticos 67 (66,3%) 24 (23,8 %) CD4 Mediana = 251 cél/mm3 (2-1300) Carga Viral Log Mediana = cópias/ml ( ) Mediana = 4,5 (2,34 – 6,27)
 Sexo. Masculino Feminino. 77 (76,2%) 24 (23,8%) Idade. Mediana = 38 anos (variação 6-66) Data do diagnóstico de HIV. Julho/81 a Setembro/02. Doença Definidora de AIDS. Pacientes Sintomáticos. 67 (66,3%) 24 (23,8 %) CD4. Mediana = 251 cél/mm3 (2-1300) Carga Viral. Log. Mediana = cópias/ml ( ) Mediana = 4,5 (2,34 – 6,27)")
30
Perfil de Utilização Prévia de Anti-retrovirais e Esquemas Terapêuticos
Utilização de Anti-retrovirais: Número de esquemas terapêuticos utilizados: Classe Droga Valor (%) ITRN Zidovudina Lamivudina Estavudina Didanosina 83 (82,2) 80 (79,2) 65 (64,4) 78 (77,2) ITRNN Efavirenz Nevirapina 28 (27,7) 24 (23,8) IP Nelfinavir Indinavir Ritonavir Saquinavir Lopinavir Amprenavir 44 (43,6) 27 (26,7) 10 (9,9) 4 (4) 1 (1) No Esquemas % 1 22 2 36 3 4 13 5 7 Justificativa para Troca No Esquemas Falha terapêutica 90 Intolerância medicamentosa 66 Terapia para Tuberculose 8 Outros 88 Total 252
 ITRN. Zidovudina. Lamivudina. Estavudina. Didanosina. 83 (82,2) 80 (79,2) 65 (64,4) 78 (77,2) ITRNN. Efavirenz. Nevirapina. 28 (27,7) 24 (23,8) IP. Nelfinavir. Indinavir. Ritonavir. Saquinavir. Lopinavir. Amprenavir. 44 (43,6) 27 (26,7) 10 (9,9) 4 (4) 1 (1) No Esquemas. % Justificativa para Troca. No Esquemas. Falha terapêutica. 90. Intolerância medicamentosa. 66. Terapia para Tuberculose. 8. Outros. 88. Total")
31
Principais Mutações de Resistência Genotípica de Pacientes com Falha Terapêutica
8% sem mutações 10% com mutações para 1 classe 73% mutações para 2 classes 9% para as 3 classes.

32
Perfil de Mutações de Resistência Associadas aos Inibidores de Protease (UPAMs) nos Subgrupos de Falha Terapêutica (N=101). Mutação 1ª falha (N=49) 2ª falha (N=37) Multifalha (N=15) L33W/F (%) 1 (6,6) V82A/F/L/T (%) 3 (6,1) 4 (10,8) 6 (49) I84V (%) 1 (2) 3 (20) L90M (%) 6 (12,2) 8 (21,6) 12 (80) * * * p < 0,01 para L90M entre 2ª e multifalhas e 1ª e multifalhas * p < 0,01para V82A/F/L/T e I84V entre 1ª e multifalhas
 2ª falha (N=37) Multifalha (N=15) L33W/F (%) 1 (6,6) V82A/F/L/T (%) 3 (6,1) 4 (10,8) 6 (49) I84V (%) 1 (2) 3 (20) L90M (%) 6 (12,2) 8 (21,6) 12 (80) * * * p < 0,01 para L90M entre 2ª e multifalhas e 1ª e multifalhas. * p < 0,01para V82A/F/L/T e I84V entre 1ª e multifalhas.")
33
Perfil de Mutações de Resistência nos Subgrupos de Falha Terapêutica para Inibidores da Transcriptase Reversa Análogos de Nucleosídeos (N=101). Mutação 1ª Falha (N=49) 2ª Falha (N=37) Multifalha (N=15) M41L (%) 16 (32,6) 13 (35) 12 (80) D67N (%) 15 (30,6) 11 (29,7) 6 (40) K70R (%) 13 (26,5) 8 (21,6) L210W (%) 12 (24,5) 10 (27) 13 (86,6) T215Y∕F (%) 21 (42,8) 17 (45,9) K219Q∕E (%) 11 (22,4) E44D (%) 3 (6,1) 1 (2,7) 3 (20) V118I (%) 7 (14,3) 7 (18,9) M184V (%) 27 (55,1) 26 (70,6) 8 (53,3) K65R (%) 4 (8,1) 2 (5,4) 69 (%) * * * * p<0,01 para M41L, L210W e T215Y/F entre 1ª e multifalha e 2ª e multifalha.
 2ª Falha (N=37) Multifalha (N=15) M41L (%) 16 (32,6) 13 (35) 12 (80) D67N (%) 15 (30,6) 11 (29,7) 6 (40) K70R (%) 13 (26,5) 8 (21,6) L210W (%) 12 (24,5) 10 (27) 13 (86,6) T215Y∕F (%) 21 (42,8) 17 (45,9) K219Q∕E (%) 11 (22,4) E44D (%) 3 (6,1) 1 (2,7) 3 (20) V118I (%) 7 (14,3) 7 (18,9) M184V (%) 27 (55,1) 26 (70,6) 8 (53,3) K65R (%) 4 (8,1) 2 (5,4) 69 (%) * * * * p<0,01 para M41L, L210W e T215Y/F entre 1ª e multifalha e 2ª e multifalha.")
34
Perfil de Suscetibilidade Anti-retroviral
Tenofovir (TDF) 40 (39,6) 1 (1) 60 (59,4) Zidovudina (AZT) 35 (34,7) 36 (35,6) 30 (29,7) ITRN Lamivudina (3TC) 34 (33,6) 62 (61,4) 5 (5) Estavudina (D4T) 29 (28,7) 26 (25,7) 46 (45,5) Didanosina (DDI) 20 (19,8) 55 (54,5) Abacavir (ABV) 19 (18,8) 56 (55,4) Entricitabina (FTC) ITRNN Dilavirdina (DLV) 58 (57,4) 3 (3) Efavirenz (EFV) Nevirapina (NVP) 45 (44,6) IP Amprenavir (APV) 4 (4) Atazanavir (ATV) 7 (6,9) 38 (37,6) Indinavir (IDV) 61 (60,4) 11 (10,9) Lopinavir (LPV) 66 (65,3) 2 (2) 33 (32,7) Nelfinavir (NFV) 52 (51,5) Ritonavir (RTV) 10 (9,9) Saquinavir (SQV) 64 (63,4) 8 (7,9) ITRN = Inibidor da transcriptase reversa análogo de nucleosídeos, ITRNN = Inibidor da transcriptase reversa não análogo de nucleosídeos, IP = Inibidor de Protease. R = resistente, I = sensibilidade intermediária e S = sensível.
 40 (39,6) 1 (1) 60 (59,4) Zidovudina (AZT) 35 (34,7) 36 (35,6) 30 (29,7) ITRN. Lamivudina (3TC) 34 (33,6) 62 (61,4) 5 (5) Estavudina (D4T) 29 (28,7) 26 (25,7) 46 (45,5) Didanosina (DDI) 20 (19,8) 55 (54,5) Abacavir (ABV) 19 (18,8) 56 (55,4) Entricitabina (FTC) ITRNN. Dilavirdina (DLV) 58 (57,4) 3 (3) Efavirenz (EFV) Nevirapina (NVP) 45 (44,6) IP. Amprenavir (APV) 4 (4) Atazanavir (ATV) 7 (6,9) 38 (37,6) Indinavir (IDV) 61 (60,4) 11 (10,9) Lopinavir (LPV) 66 (65,3) 2 (2) 33 (32,7) Nelfinavir (NFV) 52 (51,5) Ritonavir (RTV) 10 (9,9) Saquinavir (SQV) 64 (63,4) 8 (7,9) ITRN = Inibidor da transcriptase reversa análogo de nucleosídeos, ITRNN = Inibidor da transcriptase reversa não análogo de nucleosídeos, IP = Inibidor de Protease. R = resistente, I = sensibilidade intermediária e S = sensível.")
35
Efeitos das Mutações de Resistência na capacidade replicativa
11 9 5 17 capacidade replicativa Wrin T, 40th ICAAC 2000

36
Resistência aos ITRN: números de TAM e M184V
10,000 AZT 100 TDF 100 d4T 1000 10 10 Fold Change in ITRNI 100 10 1 1 1 -1 -1 -1 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 5 6 100 3TC 10 ddI 100 ABC Fold Change in ITRN 10 10 1 1 1 -1 -1 -1 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 5 6 Números de TAM M184wt M184V Whitcomb JM. 9th CRO; 2002; Seattle, Washington. Abstract 569.

37
ITRN: Atividade Residual
Suspenso IP, continuado ITRN (n = 15) Suspenso ITRN, continuado IP (n = 5) 1.5 100 Sem 8 Sem 12 Sem 16 50 1.0 Mudança na CV (log10 cópias/ml) Mudança no CD4+ (cél/mm3) NRTIs in particular have been shown to retain activity, even with drug resistance. In this landmark study conducted by Deeks and colleagues, patients with virologic failure on PI‑containing regimens either elected to discontinue their PIs and continue the NRTIs or vice versa. The figure shows that those who discontinued the PIs and continued the NRTIs had more stable HIV RNA levels and CD4+ cell counts than those who stopped the NRTIs but continued the PIs. This important study suggested that NRTIs may be critical to retain the benefit of antiviral therapy, even in the face of drug resistance. 0.5 -50 -100 -0.5 Sem 8 Sem 12 Sem 16 -150 Deeks SG, et al. J Infect Dis. 2005;192:
 Suspenso ITRN, continuado IP (n = 5) Sem 8. Sem 12. Sem Mudança na CV (log10 cópias/ml) Mudança no CD4+ (cél/mm3) NRTIs in particular have been shown to retain activity, even with drug resistance. In this landmark study conducted by Deeks and colleagues, patients with virologic failure on PI‑containing regimens either elected to discontinue their PIs and continue the NRTIs or vice versa. The figure shows that those who discontinued the PIs and continued the NRTIs had more stable HIV RNA levels and CD4+ cell counts than those who stopped the NRTIs but continued the PIs. This important study suggested that NRTIs may be critical to retain the benefit of antiviral therapy, even in the face of drug resistance Sem 8. Sem 12. Sem Deeks SG, et al. J Infect Dis. 2005;192:")
38
E-184V: Monoterapia com 3TC vs interrupção de tratamento (IT)
Prospectivo, aberto, randomizado (n=29 nos dois grupos) Pacientes em terapia contendo 3TC com CV >1.000 cópias/ml, CD4+ >500 cél/mm3 necessitando IT (todos com 184V) Randomizado: 3TC monoterapia ou IT Semanas 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00 4 8 12 16 20 24 36 48 p=0.0015 Mudança Média na CV log10 c/ml CV –300 –250 –200 –150 –100 –50 4 8 12 16 20 24 48 3TC IT 36 Semanas p=ns Mudança Média no CD4+ cél/mm3 CD4+ Inclusion criteria: "Subjects on 3TC-containing therapy with HIV RNA >1000 c/mL, CD4+ >500 cells/mm3 requesting TI (All with 184V)“ TI group (treatment interruption): randomized to stop all ARV drugs. Castagna A, et al. 3rd IAS, Rio de Janeiro 2005, #WeFo0204
 Pacientes em terapia contendo 3TC com CV >1.000 cópias/ml, CD4+ >500 cél/mm3 necessitando IT (todos com 184V) Randomizado: 3TC monoterapia ou IT. Semanas p= Mudança Média na CV log10 c/ml. CV. –300. –250. –200. –150. –100. – TC. IT. 36. Semanas. p=ns. Mudança Média no CD4+ cél/mm3. CD4+ Inclusion criteria: Subjects on 3TC-containing therapy with HIV RNA >1000 c/mL, CD4+ >500 cells/mm3 requesting TI (All with 184V) TI group (treatment interruption): randomized to stop all ARV drugs. Castagna A, et al. 3rd IAS, Rio de Janeiro 2005, #WeFo0204.")
39
Guidelines: Escolhendo um Esquema Não-supresivo de Contenção “Holding Regimen”
Tentar não usar um ITRNN Mutações para ITRNN não têm benefício no fitness Acúmulo de mutações adicionais podem resultar em resistência cruzada com ITRNN de segunda generação Tentar usar 3TC (ou FTC) Drogas bem toleradas M184V diminui o fitness Aumenta atividade de ZDV, d4T, TDF Escolher IPs e/ou ITRNs baseado na resistência e tolerabilidade/toxicidade Continuar terapia até disponibilidade de pelo menos 2 drogas ativas What are the general guidelines for choosing a nonsuppressive holding regimen? One guideline is to never use a NNNRTI, especially if the patient has failed an NNRTI-containing regimen. We know that NNRTI resistance mutations have no beneficial impact on viral fitness, and there are second-generation NNRTIs in development. We want to be able to use those drugs if and when they become available, so we do not want to have the virus evolve yet more NNRTI mutations. It is recommended that one always use lamivudine or emtricitabine, as they are simple and well-tolerated drugs with other benefits as well in this setting. We know that maintaining the M184V mutation, which is the signature lamivudine and emtricitabine mutation, will decrease the fitness of the virus. We also know that this mutation confers increased activity for other nucleoside analogues, specifically zidovudine, stavudine, and tenofovir, so there are a number of reasons why you would want to keep lamivudine or emtricitabine in the regimen. For the rest of the regimen, you want to choose PIs and nucleoside analogues based on resistance and tolerability or toxicity considerations. You want to continue this regimen until there is the availability of at least 2 new active drugs, so that you can put together a suppressive regimen for your patient.
 Drogas bem toleradas. M184V diminui o fitness. Aumenta atividade de ZDV, d4T, TDF. Escolher IPs e/ou ITRNs baseado na resistência e tolerabilidade/toxicidade. Continuar terapia até disponibilidade de pelo menos 2 drogas ativas. What are the general guidelines for choosing a nonsuppressive holding regimen One guideline is to never use a NNNRTI, especially if the patient has failed an NNRTI-containing regimen. We know that NNRTI resistance mutations have no beneficial impact on viral fitness, and there are second-generation NNRTIs in development. We want to be able to use those drugs if and when they become available, so we do not want to have the virus evolve yet more NNRTI mutations. It is recommended that one always use lamivudine or emtricitabine, as they are simple and well-tolerated drugs with other benefits as well in this setting. We know that maintaining the M184V mutation, which is the signature lamivudine and emtricitabine mutation, will decrease the fitness of the virus. We also know that this mutation confers increased activity for other nucleoside analogues, specifically zidovudine, stavudine, and tenofovir, so there are a number of reasons why you would want to keep lamivudine or emtricitabine in the regimen. For the rest of the regimen, you want to choose PIs and nucleoside analogues based on resistance and tolerability or toxicity considerations. You want to continue this regimen until there is the availability of at least 2 new active drugs, so that you can put together a suppressive regimen for your patient.")
40
Risco de retardar a Troca numa TARV “Estável”
SCOPE coorte: pacientes experimentados (n = 106)[1] HAART estável ≥ 120 dias CV > c/ml ≥ 1 mutação de resistência Teste resistência a cada 4 meses até a mudança da TARV Novas mutações com 1 ano Qualquer: 44% (95% IC: 33% a 56%) NAMs: 23% (95% IC: 15% a 34%) IP: 18% (95% IC: 9% a 34%) Persistência de viremia com TARV eleva o risco de limitar futuras opções Outros estudos mostram resultados similares[2-4] 1 nova mutação principal para IP* 1 nova NAM Qualq nova mutação 4 8 12 16 20 24 *IP-tratados (n = 71) 0.25 0.50 0.75 1.00 Proporção sem Novas Mutações 1.00 What is the “resistance penalty” of continuing antiviral therapy despite virologic failure? What happens in patients who have nonsuppressive treatment? Several studies have examined the resistance accumulation in this state of so‑called incomplete viral suppression. This is the Study of the Consequences of Protease-Inhibitor Era (SCOPE) cohort from San Francisco, California, of treatment-experienced subjects. These patients had been stable on antiviral therapy for 120 days, with virologic failure and at least 1 resistance mutation. Resistance testing was performed every 4 months until their treatment was modified. The Kaplan‑Meier curves show that patients developed new major PI mutations and new NRTI mutations over the 24 months of follow-up. Looking at it phenotypically, with the loss of 1 drug equivalent, at the end of 24 months of follow-up, approximately 50% of patients had lost at least 1 drug over time. In short, the cost of nonsuppressive therapy is the loss of future drug options. Other studies have showed similar results. In a study by Lafeuillade et al, 68% of patients developed new mutations after a median of 22 months; in a study by Margot et al, 33% developed new thymidine-associated mutations, including 2% who developed K65R during 96 weeks of follow‑up; and in a third study by Napravnik et al, 60% developed new mutations after a median of 9.3 months but with no shift on virtual phenotype. All 3 of these studies demonstrate that nonsuppressive therapy is associated with the accumulation of new resistance mutations. Importantly, a consistent finding was that new resistance mutations were more likely to be selected in patients who had relatively few mutations at baseline. However, these studies lacked data on the results of subsequent switches, and no fully powered randomized studies have evaluated the strategy of early vs deferred switching. Tempo para perda de 1 droga 0.75 Proporção sem perda de 1 Droga 0.50 0.25 Número de ART disponíveis: ZDV, 3TC, ddI, ABC,TDF, EFV, IDV, NFV, SQV, RTV, APV, LPV 4 8 12 16 20 24 Tempo (Meses) 1. Hatano H, et al. CROI Abstract Lafeuillade A, et al. IAC Abstract WeOrB Margot NA, et al. J Acquir Immune Defic Syndr. 2003;33: Napravnik S, et al. J Acquir Immune Defic Syndr. 2005;40:34-40.
[1] HAART estável ≥ 120 dias. CV > c/ml. ≥ 1 mutação de resistência. Teste resistência a cada 4 meses até a mudança da TARV. Novas mutações com 1 ano. Qualquer: 44% (95% IC: 33% a 56%) NAMs: 23% (95% IC: 15% a 34%) IP: 18% (95% IC: 9% a 34%) Persistência de viremia com TARV eleva o risco de limitar futuras opções. Outros estudos mostram resultados similares[2-4] 1 nova mutação principal para IP* 1 nova NAM. Qualq nova mutação *IP-tratados (n = 71) Proporção sem Novas Mutações What is the resistance penalty of continuing antiviral therapy despite virologic failure What happens in patients who have nonsuppressive treatment Several studies have examined the resistance accumulation in this state of so‑called incomplete viral suppression. This is the Study of the Consequences of Protease-Inhibitor Era (SCOPE) cohort from San Francisco, California, of treatment-experienced subjects. These patients had been stable on antiviral therapy for 120 days, with virologic failure and at least 1 resistance mutation. Resistance testing was performed every 4 months until their treatment was modified. The Kaplan‑Meier curves show that patients developed new major PI mutations and new NRTI mutations over the 24 months of follow-up. Looking at it phenotypically, with the loss of 1 drug equivalent, at the end of 24 months of follow-up, approximately 50% of patients had lost at least 1 drug over time. In short, the cost of nonsuppressive therapy is the loss of future drug options. Other studies have showed similar results. In a study by Lafeuillade et al, 68% of patients developed new mutations after a median of 22 months; in a study by Margot et al, 33% developed new thymidine-associated mutations, including 2% who developed K65R during 96 weeks of follow‑up; and in a third study by Napravnik et al, 60% developed new mutations after a median of 9.3 months but with no shift on virtual phenotype. All 3 of these studies demonstrate that nonsuppressive therapy is associated with the accumulation of new resistance mutations. Importantly, a consistent finding was that new resistance mutations were more likely to be selected in patients who had relatively few mutations at baseline. However, these studies lacked data on the results of subsequent switches, and no fully powered randomized studies have evaluated the strategy of early vs deferred switching. Tempo para perda de 1 droga Proporção sem perda de 1 Droga Número de ART disponíveis: ZDV, 3TC, ddI, ABC,TDF, EFV, IDV, NFV, SQV, RTV, APV, LPV Tempo (Meses) 1. Hatano H, et al. CROI Abstract Lafeuillade A, et al. IAC Abstract WeOrB Margot NA, et al. J Acquir Immune Defic Syndr. 2003;33: Napravnik S, et al. J Acquir Immune Defic Syndr. 2005;40:")
41
Evidências dos Ensaios Clínicos: Enfuvirtida + IP/r ativo
Estudo ENF + 1 IP/r ativo + EO TORO 1 & 2 ENF + LPV/r + EO1 RESIST 1 & 2 ENF + TPV/r + EO2 POWER 1 & 2 ENF + DRV + EO3 Haubrich et al. IDSA Abstract 785 Cooper et al. CROI Abstract 560 Katlama et al. CROI Abstract 164LB

42
Evidência dos Ensaios Clínicos: Enfuvirtida + IP/r ativo
TORO 1 & 2 RESIST 1 & 2 POWER 1 & 2 64% Pacientes (%) 55% 54% Pacientes (%) Pacientes (%) 46% 30% 24% <400 cópias/ml <400 cópias/ml <50 cópias/ml LPV/r TPV/r TMC114/r ENF + LPV/r ENF + TPV/r ENF + TMC114/r Haubrich et al. IDSA Abstract 785; Hill et al. BHIVA Abstract P1.
 55% 54% Pacientes (%) Pacientes (%) 46% 30% 24% <400 cópias/ml. <400 cópias/ml. <50 cópias/ml. LPV/r. TPV/r. TMC114/r. ENF + LPV/r. ENF + TPV/r. ENF + TMC114/r. Haubrich et al. IDSA Abstract 785; Hill et al. BHIVA Abstract P1.")
43
POWER 1 e 2: CV < 50 cópias/ml na Semana 48 (ITT-TLOVR)
Estudo de 96-sem, em andamento, randomizado com pacts experimentado nas 3-classes ≥ 1 mutação primária p/ IP CV > cópias/ml DRV/RTV 600/100 BID (dose ideal escolhida na semana 24) Eficácia Superior na semana 48 sobre o IP/r comparador 100 DRV/RTV 600/100 mg BID IPC/RTV 80 45%* 46%* 60 Pacts com CV < 50 c/ml (%) 40 12% 10% 20 ITT, intent-to-treat; TLOVR, time to loss of virologic response For more information on this study, go online to: 8 16 24 32 40 48 Semanas *p < 0,001 vs IPC/RTV. Nem todos os pacientes alcançaram a semana 48 nesta análise. Lazzarin A, et al. IAC Abstract TUAB0104
 Eficácia Superior na semana 48 sobre o IP/r comparador DRV/RTV 600/100 mg BID. IPC/RTV %* 46%* 60. Pacts com CV < 50 c/ml (%) % 10% 20. ITT, intent-to-treat; TLOVR, time to loss of virologic response. For more information on this study, go online to: Semanas. *p < 0,001 vs IPC/RTV. Nem todos os pacientes alcançaram a semana 48 nesta análise. Lazzarin A, et al. IAC Abstract TUAB0104.")
44
TORO: Preditores de Supressão Viral
% Pacientes com CV < 400 c/ml pelo Número de Fatores Prognósticos Positivos Fatores Basais OR p CD4+ > 100 cél/mm3 2,4 < 0,0001 CV < c/ml 1,8 < 0,0032 ≤ 10 ARVs prévios ≥ 2 ARVs ativos 2,3 100 ENF + EO EO 80 *p < 0,05 67 60 * Pacientes (%) 43 * 40 * 20 ENF, enfuvirtide; OB, optimized background. The T-20 vs Optimized Regimen Only (TORO) studies began to clarify the predictors of virologic response in patients with high‑level, multiclass resistance. This multivariate analysis looked at the predictors of virologic suppression in the TORO studies and found that having ≥ 2 active antiretrovirals in the background was an important predictor. Other important predictors were a higher CD4+ cell count as well as a lower HIV RNA level. As shown in the figure on the right, the greater the number of positive prognostic factors, the higher the likelihood that both the enfuvirtide regimen and the optimized background regimen alone would achieve virologic suppression. 11 * * 1 2 3 4 N de Fatores Prognósticos Positivos n = 121 67 49 28 Montaner J, et al. HIV Clin Trials. 2005;6:
 43. * 40. * 20. ENF, enfuvirtide; OB, optimized background. The T-20 vs Optimized Regimen Only (TORO) studies began to clarify the predictors of virologic response in patients with high‑level, multiclass resistance. This multivariate analysis looked at the predictors of virologic suppression in the TORO studies and found that having ≥ 2 active antiretrovirals in the background was an important predictor. Other important predictors were a higher CD4+ cell count as well as a lower HIV RNA level. As shown in the figure on the right, the greater the number of positive prognostic factors, the higher the likelihood that both the enfuvirtide regimen and the optimized background regimen alone would achieve virologic suppression. 11. * * N de Fatores Prognósticos Positivos. n = Montaner J, et al. HIV Clin Trials. 2005;6:")
45
RESIST: Maior Resposta com Mais Drogas Ativas no Esquema
100 TPV/RTV IPC/RTV 80 Pacientes com 1 log10 Redução na CV (%) 60 54.7 46.2 41.2 37.4 40 34.3 A number of analyses were performed to try and help clinicians figure out which patients might benefit most from tipranavir/ritonavir. One analysis looked at the number of active agents in the regimen and how this related to treatment response. The analysis found that the more active agents in the regimen, the greater the likelihood that the patient was able to achieve greater than a 1 log10 reduction in viral load. This was true both for patients who were randomized to tipranavir/ritonavir and those randomized to optimized background therapy alone; however, patients randomized to tipranavir/ritonavir had an increased likelihood of achieving a viral load reduction of greater than 1 log10 copies/mL. For more information, go online to: 19.9 18.9 20 13.1 12.9 9.1 1 2 3 Overall Número de ARVs Sensíveis Cooper D, et al. CROI Abstract 560.
 A number of analyses were performed to try and help clinicians figure out which patients might benefit most from tipranavir/ritonavir. One analysis looked at the number of active agents in the regimen and how this related to treatment response. The analysis found that the more active agents in the regimen, the greater the likelihood that the patient was able to achieve greater than a 1 log10 reduction in viral load. This was true both for patients who were randomized to tipranavir/ritonavir and those randomized to optimized background therapy alone; however, patients randomized to tipranavir/ritonavir had an increased likelihood of achieving a viral load reduction of greater than 1 log10 copies/mL. For more information, go online to: 3. Overall. Número de ARVs Sensíveis. Cooper D, et al. CROI Abstract 560.")
46
POWER 1, 2 & 3: Número de mutações associadas com diminuição da resposta a DRV/r e resposta virológica CV <50 cópias/ml (todos os pacientes) 100 80 60 Pacientes com CV < 50 cópias/ml na semana 24 (%) 40 64 50 20 42 42 22 10 0 (67) 1 (94) 2 (113) 3 (58) ≥4 (41) Todos (373) Número de mutações para DRV (Número de pacientes) * Mutações do DRV = V11I, V32I, L33F, I47V, I50V, I54L/M, G73S, L76V, I84V, L89V De Meyer S, XV IHDRW, 13–17 June 2006, Sitges, Spain. Poster 73.
 (67) 1 (94) 2 (113) 3 (58) ≥4 (41) Todos (373) Número de mutações para DRV (Número de pacientes) * Mutações do DRV = V11I, V32I, L33F, I47V, I50V, I54L/M, G73S, L76V, I84V, L89V. De Meyer S, XV IHDRW, 13–17 June 2006, Sitges, Spain. Poster 73.")
47
Disponível em: http://www. AIDS. gov. br
Disponível em: Acessada em 15 de novembro de 2006.

48
O que diz o Documento Nacional
Após a primeira ou até a segunda falha terapêutica, o objetivo do tratamento continuará sendo a supressão máxima da viremia (carga viral indetectável). A mudança do esquema anti-retroviral deve ser feita o mais precocemente possível para que se previna a seleção adicional de mutações, baseada, sempre que possível, no teste de genotipagem (melhor estratégia). Nos casos de múltiplas falhas terapêuticas ou evidências de resistência a múltiplas drogas, a supressão viral dificilmente será alcançada com as opções terapêuticas atualmente disponíveis. O objetivo passará ser prevenir ou minimizar o dano imunológico e a progressão clínica. Disponível em: Acessada em 15 de novembro de 2006.
. A mudança do esquema anti-retroviral deve ser feita o mais precocemente possível para que se previna a seleção adicional de mutações, baseada, sempre que possível, no teste de genotipagem (melhor estratégia). Nos casos de múltiplas falhas terapêuticas ou evidências de resistência a múltiplas drogas, a supressão viral dificilmente será alcançada com as opções terapêuticas atualmente disponíveis. O objetivo passará ser prevenir ou minimizar o dano imunológico e a progressão clínica. Disponível em: Acessada em 15 de novembro de")
50
Guidelines: Metas da Terapia Anti-retroviral em Pacientes Experimentados
Experiência Limitada: resistência, mas com opções de tratamento adequadas Máxima supressão viral Considerar a troca precoce do esquema para prevenir novas mutações de resistência Experiência Intermediária e Extensa: resistência, com algumas opções de tratamento Máxima supressão viral, se possível Preservação da função imune e prevenção da progressão clínica Balancear os benefícios de uma supressão viral parcial com os riscos de acúmulo de mutações adicionais For patients who have limited prior treatment history and limited drug resistance on resistance testing and have adequate treatment options, the goal of therapy should be to achieve maximal suppression of viral load (ie, viral load less than the limits of detection). In these patients, consider changing the antiretroviral regimen early if the viral load rebounds to prevent the development of further resistance mutations. For patients who have intermediate prior treatment histories and evidence of drug resistance, there may be some treatment options, especially with some of the newer agents that have been FDA approved or are in the clinical development pipeline. In general, the goal of therapy should still be to maximally suppress viral load, and even in this case, it may be possible to achieve viral loads below the limits of detection. Another goal is to preserve immune function and to prevent clinical prevention, if at all possible. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de 2006.
. In these patients, consider changing the antiretroviral regimen early if the viral load rebounds to prevent the development of further resistance mutations. For patients who have intermediate prior treatment histories and evidence of drug resistance, there may be some treatment options, especially with some of the newer agents that have been FDA approved or are in the clinical development pipeline. In general, the goal of therapy should still be to maximally suppress viral load, and even in this case, it may be possible to achieve viral loads below the limits of detection. Another goal is to preserve immune function and to prevent clinical prevention, if at all possible. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de")
51
Princípios Gerais para Seleção de um Novo Esquema
Para pacientes com ≥ 2 drogas ativas, a meta da terapia deve ser a completa supressão viral Novos medicamentos já aprovados aumentam a chance de alcançar a meta IP ativo reforçado com RTV mais uma droga de nova classe, pode oferecer uma potente atividade anti-retroviral As the DHHS and IAS guidelines mention and with new agents becoming available, we have an evolving goal for antiretroviral therapy for all HIV-positive patients, regardless of the extent of previous treatment experience, and that is to achieve and maintain an undetectable HIV-1 RNA level, when possible. In a practical, real-world setting, for patients who have access to at least 2 active agents, the goal of therapy should be to completely suppress viral load. There are a number of approaches to achieving suppression, and as discussed earlier, a boosted PI regimen, especially if combined with a novel agent like an entry inhibitor, can provide potent antiretroviral activity and help you achieve the goal of completely suppressing viral load. In general, we now know that we can achieve that goal in an increasing number of salvage patients, and we will discuss how some of the newest PIs may help us achieve that ultimate goal. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de 2006.

52
Opções para Pacientes com < 2 Drogas Ativas
Avaliar a necessidade de troca, baseada no estado clínico Investigar e estimar quando novos medicamentos vão estar disponíveis (acesso expandido) Adição de um único medicamento ativo pode ser necessário em pacientes com doença muito avançada com alto risco de progressão Continuar a terapia não-supressiva Trocar por um esquema de contenção “holding regimen” Manter um vírus com baixa capacidade replicativa Evitar novas mutações que podem diminuir futuras opções Em geral, parar a terapia aumenta os riscos de progressão clínica e não é recomendado, exceto, talvez, para pacientes com alto CD4+ What are the treatment options when we cannot achieve suppression? There are a number of questions here and I do not think there are definitive answers to any of these. Do we want to continue nonsuppressive therapy? The answer depends on where patients are in terms of their CD4+ cell count and the level of their viral load. Do we want to switch to a holding regimen? What does a holding regimen do? It can maintain low viral fitness for the virus that the patient is harboring and perhaps avoid new mutations that could decrease future treatment options. Sometimes we may need to add a single active agent because the patient is at high risk of disease progression, but in general, that is discouraged. Again, unless one has a patient who is at immediate risk of disease progression or who has already demonstrated that he or she is developing opportunistic infections, this is not the best option. Do we want to stop therapy and wait for new agents? We have seen on the basis of clinical trials that perhaps that is not a good idea, especially for patients who have advanced disease and low CD4+ cell counts. If we stop treatment, we see a return of wild-type virus in that setting with further reductions in CD4+ cell count, which would put the patient at increased risk for developing opportunistic infection. In general, it is not recommended to stop antiretroviral therapy. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de 2006.
 Adição de um único medicamento ativo pode ser necessário em pacientes com doença muito avançada com alto risco de progressão. Continuar a terapia não-supressiva. Trocar por um esquema de contenção holding regimen Manter um vírus com baixa capacidade replicativa. Evitar novas mutações que podem diminuir futuras opções. Em geral, parar a terapia aumenta os riscos de progressão clínica e não é recomendado, exceto, talvez, para pacientes com alto CD4+ What are the treatment options when we cannot achieve suppression There are a number of questions here and I do not think there are definitive answers to any of these. Do we want to continue nonsuppressive therapy The answer depends on where patients are in terms of their CD4+ cell count and the level of their viral load. Do we want to switch to a holding regimen What does a holding regimen do It can maintain low viral fitness for the virus that the patient is harboring and perhaps avoid new mutations that could decrease future treatment options. Sometimes we may need to add a single active agent because the patient is at high risk of disease progression, but in general, that is discouraged. Again, unless one has a patient who is at immediate risk of disease progression or who has already demonstrated that he or she is developing opportunistic infections, this is not the best option. Do we want to stop therapy and wait for new agents We have seen on the basis of clinical trials that perhaps that is not a good idea, especially for patients who have advanced disease and low CD4+ cell counts. If we stop treatment, we see a return of wild-type virus in that setting with further reductions in CD4+ cell count, which would put the patient at increased risk for developing opportunistic infection. In general, it is not recommended to stop antiretroviral therapy. Adaptado do DHHS Guidelines 10/06. Disponível em: Acessada em 15 de novembro de")
53
Guideline IAS-USA: Metas da Terapia Anti-retroviral em Pacientes Experimentados
Supressão Viral para < 50 cópias/ml pode ser alcançável e deve ser uma meta da terapia em pacientes experimentados. “Os dados dos estudos RESIST e POWER ajudaram a definir o momento ideal para uso de enfuvirtida. Se várias drogas ativas estão disponíveis, além da ENF, é melhor retardar a sua utilização até que seja 1 de 2 drogas plenamente ativas disponíveis (AII). Contudo, desde que a meta da terapia é alcançar CV < 50 cópias/ml, ENF sempre é necessária para alcançar um grau de sucesso entre pacientes fortemente experimentados em TARV (AI).” Hammer SM, et al. JAMA. 2006;296:
. Contudo, desde que a meta da terapia é alcançar CV < 50 cópias/ml, ENF sempre é necessária para alcançar um grau de sucesso entre pacientes fortemente experimentados em TARV (AI). Hammer SM, et al. JAMA. 2006;296:")
54
Recomendações para uso de Enfuvirtida (ENF)
A Enfuvirtida é indicada para os pacientes que se encontrem dentro de todos os critérios abaixo: Teste de genotipagem do HIV nos últimos 12 meses. Pelo menos uma droga sem resistência detectada na genotipagem. Considerar com muita cautela as drogas com baixa barreira genética à resistência (3TC e ITRNN), se já tiverem sido utilizadas previamente. Para compor o novo esquema, considerar o histórico de terapia anti-retroviral, a opinião do médico assistente quanto à possibilidade de adesão e a opinião do MRG (Médico de Referência em Genotipagem). Disponível em: Acessada em 15 de novembro de 2006.
, se já tiverem sido utilizadas previamente. Para compor o novo esquema, considerar o histórico de terapia anti-retroviral, a opinião do médico assistente quanto à possibilidade de adesão e a opinião do MRG (Médico de Referência em Genotipagem). Disponível em: Acessada em 15 de novembro de")
55
Recomendações para uso de Enfuvirtida (ENF)
Os pacientes usando ENF devem ser acompanhados da seguinte forma: 1. Reavaliar após três e seis meses: CD4, Carga Viral e Bioquímica sanguínea. 2. Notificar à ANVISA ( os eventos adversos sérios. 3. Enviados dados para as coordenações estaduais, após as consultas regulares do paciente. 4. Após avaliação de três e seis meses, reavaliar com intervalo de quatro meses seguindo os mesmos critérios definidos anteriormente, nos itens de 1 a 3; 5. Reavaliar a cada consulta a adesão e a resposta ao esquema de resgate. Disponível em: Acessada em 15 de novembro de 2006.

56
ITRNN: Etravirina (TMC125-C223) Resposta Virólogica na Semana 48
N = 199 pacientes com resistência a ITRNN e ≥ 3 mutações primárias para IP Mediana do FC para ITRNN NVP: 61,3 EFV: 41,4 Etravirina: 1,6 Pacientes randomizados para Etravirina (400 mg BID ou 800mg BID) + ITRNs ± LPV/RTV ± ENF Controle Ativo: melhor esquema disponível com drogas licenciadas (excuíndo ITRNNs) 100 90 80 70 60 Pacts com CV < 50 c/ml na semana 48 (%) 50 40 VL, viral load. Etravirine is a second-generation NNRTI. In this pivotal study, 199 treatment-experienced patients with NNRTI resistance and at least 3 primary PI mutations were randomized to receive either an optimized background regimen alone or 2 different doses of etravirine. At baseline, these patients had high median fold changes in susceptibility to nevirapine and efavirenz. Both doses of etravirine induced a greater decline in HIV RNA levels than the optimized background regimen alone. 30 23% 22% 20 10 0% Etravirina 400 mg BID Etravirina 800 mg BID Controle Cohen C, et al IAC Abstract TUPE0061.
 + ITRNs ± LPV/RTV ± ENF. Controle Ativo: melhor esquema disponível com drogas licenciadas (excuíndo ITRNNs) Pacts com CV < 50 c/ml na semana 48 (%) VL, viral load. Etravirine is a second-generation NNRTI. In this pivotal study, 199 treatment-experienced patients with NNRTI resistance and at least 3 primary PI mutations were randomized to receive either an optimized background regimen alone or 2 different doses of etravirine. At baseline, these patients had high median fold changes in susceptibility to nevirapine and efavirenz. Both doses of etravirine induced a greater decline in HIV RNA levels than the optimized background regimen alone % 22% % Etravirina 400 mg BID. Etravirina 800 mg BID. Controle. Cohen C, et al IAC Abstract TUPE0061.")
57
Etravirina (TMC125-C223): Mutações Basais e Resposta na Semana 48
Controle Ativo Resposta a ETV 800 BID pelo No. de Mutações para ITRNN no Basal ETV 800 BID 0* 1 2 ≥ 3 n = 79 n = 40 n = 14 n = 19 n = 16 n = 30 -0.14 -0.5 -0.54 Mudança Média na CV (log10 cópias/ml) -1.0 -0.9 -1.01 -1.5 -1.38 -1.67 ITT, NC = F -2.0 *Todos os pacientes tinham mutações para ITRNN em genotipagens anteriores. Cohen C, et al IAC Abstract TUPE0061.
 ITT, NC = F *Todos os pacientes tinham mutações para ITRNN em genotipagens anteriores. Cohen C, et al IAC Abstract TUPE0061.")
58
Inibidor de Integrase: MK-0518 - Estudo fase IIb
Multi-cêntrico, duplo-cego, randomizado Característica dos Pacientes Média de duração de HAART: 9-11 anos Média de CV: log10 cópias/ml Média de CD4+: cél/mm3 Uso de ENF em EO: 33% a 38% Pacientes sem IP ativo no EO: 84% a 98% PSS = 0: 40% a 57% Semana 16 Placebo + EO (n = 43) Preliminary phase IIb data were presented at CROI that assessed the safety and efficacy of MK-0518 in triple-class–experienced patients with resistance confirmed by genotype or phenotype. This was a randomized, double-blind, multicenter trial. Inclusion criteria included CD4+ cell count > 50 cells/mm3 and HIV-1 RNA > 5000 copies/mL. So far, 167 patients were randomized to either placebo plus optimized background or 1 of 3 doses of MK-0518 (200, 400, or 600 mg twice daily) plus optimized background. Patients in this study had been on HAART for a mean of 9-11 years, depending on the study arm. Approximately one third of the patients used enfuvirtide in the optimized background. For 40% to 57% of patients, the phenotypic susceptibility score was 0, meaning none of the drugs in their background regimen had activity by phenotypic susceptibility score. The mean HIV-1 RNA at baseline was between 4.6 and 4.8 log10 copies/mL and the mean CD4+ cell count was between 220 and 283 cells/mm3. For more information, please go online to: Resistência “Triple-class” por genotipagem/fenotipagem; CD4+ > 50 cél/mm3; CV > cópias/ml (N = 167) MK BID + EO (n = 40) MK BID + EO (n = 42) MK BID + EO (n = 42) Grinsztejn B, et al. CROI Abstract 159LB.
 Preliminary phase IIb data were presented at CROI that assessed the safety and efficacy of MK-0518 in triple-class–experienced patients with resistance confirmed by genotype or phenotype. This was a randomized, double-blind, multicenter trial. Inclusion criteria included CD4+ cell count > 50 cells/mm3 and HIV-1 RNA > 5000 copies/mL. So far, 167 patients were randomized to either placebo plus optimized background or 1 of 3 doses of MK-0518 (200, 400, or 600 mg twice daily) plus optimized background. Patients in this study had been on HAART for a mean of 9-11 years, depending on the study arm. Approximately one third of the patients used enfuvirtide in the optimized background. For 40% to 57% of patients, the phenotypic susceptibility score was 0, meaning none of the drugs in their background regimen had activity by phenotypic susceptibility score. The mean HIV-1 RNA at baseline was between 4.6 and 4.8 log10 copies/mL and the mean CD4+ cell count was between 220 and 283 cells/mm3. For more information, please go online to: Resistência Triple-class por genotipagem/fenotipagem; CD4+ > 50 cél/mm3; CV > cópias/ml. (N = 167) MK BID + EO (n = 40) MK BID + EO (n = 42) MK BID + EO (n = 42) Grinsztejn B, et al. CROI Abstract 159LB.")
59
MK-0518: Supressão Virológica na Semana 16
Pacientes com CV < 400 cópias/ml (%) MK mg BID (n = 42) 100 80 60 40 20 2 4 8 12 16 Semana MK mg BID (n = 40) EO sozinho (n = 43) MK mg BID (n = 42) Pacientes com CV < 50 cópias/ml (%) Observed data showed that between 70% and 80% of patients randomized to MK-0518 plus optimized background reached an HIV-1 RNA level < 400 copies/mL. For patients randomized to placebo, the proportion with an HIV-1 RNA level < 400 copies/mL was only 20%. It should be noted that only 2 patients discontinued the study, so data were collected on virtually all patients, although not all patients had reached 16 weeks at the time of this data analysis. With MK-0518, between 50% and 70% of patients had an HIV-1 RNA level < 50 copies/mL at Week 16 while < 20% of patients who received placebo achieved such viral suppression. It is important to note that these are only 16-week data and, therefore, represent only the initial preliminary observations. For more information, please go online to: *Somente 2 pacientes descontinuaram o estudo. Grinsztejn B, et al. CROI Abstract 159LB.
 MK mg BID (n = 42) Semana. MK mg BID (n = 40) EO sozinho (n = 43) MK mg BID (n = 42) Pacientes com CV < 50 cópias/ml (%) Observed data showed that between 70% and 80% of patients randomized to MK-0518 plus optimized background reached an HIV-1 RNA level < 400 copies/mL. For patients randomized to placebo, the proportion with an HIV-1 RNA level < 400 copies/mL was only 20%. It should be noted that only 2 patients discontinued the study, so data were collected on virtually all patients, although not all patients had reached 16 weeks at the time of this data analysis. With MK-0518, between 50% and 70% of patients had an HIV-1 RNA level < 50 copies/mL at Week 16 while < 20% of patients who received placebo achieved such viral suppression. It is important to note that these are only 16-week data and, therefore, represent only the initial preliminary observations. For more information, please go online to: *Somente 2 pacientes descontinuaram o estudo. Grinsztejn B, et al. CROI Abstract 159LB.")
60
MK-0518 vs EFV: Supressão Virológica em Pacientes Naïve (ITT)
203 pacientes naïve randomizados para 1 das 4 doses de MK-0518 ou EFV + TDF + 3TC 85% a 100% dos pacientes do grupo do MK-0518 alcançaram CV < 50 na semana 24 Supressão Viral foi alcançada mais rapidamente em todos os braços do MK-0518 vs o braço do EFV MK mg BID (n = 39) MK mg BID (n = 40) MK mg BID (n = 41) MK mg BID (n = 40) EFV 600 mg QD (n = 38) 100 80 60 Pacts com CV < 50 c/ml (%) * For more information on this study, go online to: 40 * 20 2 4 8 12 16 24 Semana *p < 0,001 para MK-0518 em cada dose vs EFV. Markowitz M, et al. IAC Abstract THLB0214.
 MK mg BID (n = 40) MK mg BID (n = 41) MK mg BID (n = 40) EFV 600 mg QD (n = 38) Pacts com CV < 50 c/ml (%) * For more information on this study, go online to: * Semana. *p < 0,001 para MK-0518 em cada dose vs EFV. Markowitz M, et al. IAC Abstract THLB0214.")
61
Inibidor de Integrase: GS-9137
Fase IIa, 10-dias em monoterapia vs placebo N = 40 pacientes Naïve de tratamento GS-9137 tateando dose Resposta Dose-dependente Reforço do RTV permitiu menor dose do GS-9137 e 1x/dia Nenhum evento adverso sério Placebo GS mg BID GS mg QD GS mg BID GS mg BID GS mg QD + RTV 100 mg QD 0.0 -0.5 Mudança Mediana da CV (log10 cópias/ml) -1.0 -1.5 Data were also presented at CROI from the phase IIa study of the integrase inhibitor GS The study consisted of 10 days of monotherapy with either placebo or 1 of 5 doses of GS‑9137, with or without ritonavir boosting. The study included 40 HIV-positive patients who were antiretroviral naive or off treatment, so the only active compound they received was expected to be GS Five doses of GS-9137 were tested: 800 mg once daily, 800 mg twice daily, 400 mg twice daily, 200 mg twice daily, and 50 mg once daily with 100 mg of ritonavir. GS-9137 is metabolized by the cytochrome P450 system and a small amount of ritonavir increases the concentration of the drug substantially. Overall, a dose-dependent treatment response was observed, and ritonavir boosting allowed a lower, once-daily GS-9137 dosing with similar activity to 800 mg twice daily dosing. The peak antiviral effect with 50 mg of GS-9137 plus 100 mg of ritonavir once daily was a decrease of approximately 2.0 log10 copies/mL; 800 mg twice daily and 400 mg twice daily had similar activity. There were no serious adverse events in any arm over the 10-day trial. The once-daily GS-9137 dose with ritonavir is being moved forward to a phase IIb trial. For more information, please go online to: -2.0 -2.5 BL 2 4 7 11 14 21 Dia Dose de 1x/dia com RTV será investigada em estudo fase II com pacientes experimentados DeJesus E, et al. CROI Abstract 160LB.
 Data were also presented at CROI from the phase IIa study of the integrase inhibitor GS The study consisted of 10 days of monotherapy with either placebo or 1 of 5 doses of GS‑9137, with or without ritonavir boosting. The study included 40 HIV-positive patients who were antiretroviral naive or off treatment, so the only active compound they received was expected to be GS Five doses of GS-9137 were tested: 800 mg once daily, 800 mg twice daily, 400 mg twice daily, 200 mg twice daily, and 50 mg once daily with 100 mg of ritonavir. GS-9137 is metabolized by the cytochrome P450 system and a small amount of ritonavir increases the concentration of the drug substantially. Overall, a dose-dependent treatment response was observed, and ritonavir boosting allowed a lower, once-daily GS-9137 dosing with similar activity to 800 mg twice daily dosing. The peak antiviral effect with 50 mg of GS-9137 plus 100 mg of ritonavir once daily was a decrease of approximately 2.0 log10 copies/mL; 800 mg twice daily and 400 mg twice daily had similar activity. There were no serious adverse events in any arm over the 10-day trial. The once-daily GS-9137 dose with ritonavir is being moved forward to a phase IIb trial. For more information, please go online to: BL Dia. Dose de 1x/dia com RTV será investigada em estudo fase II com pacientes experimentados. DeJesus E, et al. CROI Abstract 160LB.")
62
ACTG 5211: Estudo Fase II de Vicriviroc em Pacientes Experimentados
Entrada no Estudo Dia 14 Semana 24 Semana 48 Placebo (n = 28) Adultos experimentados; CV ≥ cópias/ml Em esquema contendo RTV; Somente com fenótipo R5; Estratificado por uso de ENF e pelo CD4+ < ou ≥ 50 cél/mm³ no basal (N = 118) Vicriviroc 5 mg QD (n = 23) Vicriviroc 10 mg QD (n = 30) For more information on this study, go online to: Vicriviroc 15 mg QD (n = 30) Esquema em Falha EO (incluindo de mg RTV) Gulick R, et al. IAC Abstract THLB0217.
 Adultos experimentados; CV ≥ cópias/ml. Em esquema contendo RTV; Somente com fenótipo R5; Estratificado por uso de ENF e pelo CD4+ < ou ≥ 50 cél/mm³ no basal. (N = 118) Vicriviroc 5 mg QD. (n = 23) Vicriviroc 10 mg QD. (n = 30) For more information on this study, go online to: Vicriviroc 15 mg QD. (n = 30) Esquema em Falha. EO. (incluindo de mg RTV) Gulick R, et al. IAC Abstract THLB0217.")
63
Mudança Média de CV na semana 24 (ITT) (log10 cópias/ml)
ACTG 5211: Estudo Fase II do Vicriviroc em Pacientes Experimentados (cont) Adição de Vicriviroc ao esquema em falha por 14 dias, associado com ~ 1 log10 de redução na CV Supressão da CV foi sustentada até a semana 24 após a otimização do esquema no dia 14 Mudanças no tropismo do co-receptor ocorreram após o screening e durante o estudo Pessoas com vírus do tropismo duplo/misto (R5/X4) detectados na entrada tiveram uma supressão viral inferior vs vírus monotrópico R5 Dose de Vicriviroc Placebo 5 mg 10 mg 15 mg n = 28 23 30 30 -0.5 -0,29 -1.0 Mudança Média de CV na semana 24 (ITT) (log10 cópias/ml) -1.5 For more information on this study, go online to: -1,51* -1,68† -2.0 -1,86† -2.5 *p = 0,002 vs placebo. †p < 0,001 vs placebo. Gulick R, et al. IAC Abstract THLB0217.
 Adição de Vicriviroc ao esquema em falha por 14 dias, associado com ~ 1 log10 de redução na CV. Supressão da CV foi sustentada até a semana 24 após a otimização do esquema no dia 14. Mudanças no tropismo do co-receptor ocorreram após o screening e durante o estudo. Pessoas com vírus do tropismo duplo/misto (R5/X4) detectados na entrada tiveram uma supressão viral inferior vs vírus monotrópico R5. Dose de Vicriviroc. Placebo. 5 mg. 10 mg. 15 mg. n = , Mudança Média de CV na semana 24 (ITT) (log10 cópias/ml) For more information on this study, go online to: -1,51* -1,68† ,86† *p = 0,002 vs placebo. †p < 0,001 vs placebo. Gulick R, et al. IAC Abstract THLB0217.")
64
A4001029: Estudo Fase II de Maraviroc em Pacientes Experimentados com HIV X4
Estudo Fase IIb de maraviroc 150 mg QD ou BID vs placebo, ambos com EO em 190 pacits experimentados com vírus R5/X4 Sem diferença na ↓ CV entre MVC + EO vs EO na semana 24 Sem eventos adversos sérios; sem hepatotoxicidade, limfoma ou adenocarcinoma Maior contagem de CD4+ na semana 24 com MVC vs placebo Detecção de vírus X4-monotrópico mais comum na falha de tratamento com MVC Similar ↑ CD4+ em pacts com X4-mono vs toda a população tratada com MVC, sugerindo não haver impacto na recuperação imunológica A is an ongoing, 48-week, randomized, double-blind, multicenter, placebo-controlled Phase 2b study of MVC in treatment-experienced (triple-class experience and/or dual-class-resistant HIV-1) patients with HIV-1 RNA ≥5000 copies/mL & non-R5-tropic HIV-1 infection. Eligible patients were randomized 1:1:1 to one of three arms: OBT (comprising 3–6 open-label ARVs of which at least one is active and no more than one is an NNRTI) and placebo OBT plus MVC 150 mg QD OBT plus MVC 150 mg BID. Patients whose OBT did not contain a PI or the NNRTI delavirdine, received doses of MVC 300 mg QD or BID according to their original randomization. Co-receptor tropism testing was performed in all patients with treatment failure and/or HIV-1 RNA ≥500 copies/mL at screening, weeks 4, 8 and every 8 weeks thereafter. The primary endpoint of this analysis was the change from baseline to 24 weeks in viral load for patients with D/M-tropic HIV-1 at screening. Treatment failure was defined as any one of: an increase to ≥3x baseline plasma HIV-1 RNA level at week 2 or thereafter HIV-1 RNA <0.5 log10 decrease from baseline starting at Week 8 HIV-1 RNA <1.0 log10 decrease from baseline starting at Week 8, in a patient who had previously achieved a ≥2.0 log10 decrease from baseline an increase in HIV-1 RNA to ≥5,000 copies/mL in a patient previously confirmed to have undetectable levels of <400 copies/mL. These viral load criteria were confirmed by two consecutive measurements. For more information on this study, go online to: Mayer H, et al. IAC Abstract THLB0215.
 patients with HIV-1 RNA ≥5000 copies/mL & non-R5-tropic HIV-1 infection. Eligible patients were randomized 1:1:1 to one of three arms: OBT (comprising 3–6 open-label ARVs of which at least one is active and no more than one is an NNRTI) and placebo. OBT plus MVC 150 mg QD. OBT plus MVC 150 mg BID. Patients whose OBT did not contain a PI or the NNRTI delavirdine, received doses of MVC 300 mg QD or BID according to their original randomization. Co-receptor tropism testing was performed in all patients with treatment failure and/or HIV-1 RNA ≥500 copies/mL at screening, weeks 4, 8 and every 8 weeks thereafter. The primary endpoint of this analysis was the change from baseline to 24 weeks in viral load for patients with D/M-tropic HIV-1 at screening. Treatment failure was defined as any one of: an increase to ≥3x baseline plasma HIV-1 RNA level at week 2 or thereafter. HIV-1 RNA <0.5 log10 decrease from baseline starting at Week 8. HIV-1 RNA <1.0 log10 decrease from baseline starting at Week 8, in a patient who had previously achieved a ≥2.0 log10 decrease from baseline. an increase in HIV-1 RNA to ≥5,000 copies/mL in a patient previously confirmed to have undetectable levels of <400 copies/mL. These viral load criteria were confirmed by two consecutive measurements. For more information on this study, go online to: Mayer H, et al. IAC Abstract THLB0215.")
65
Na falha virológica de qualquer braço
Estudo Fase II de TNX-355 Novo Inibidor de Entrada Semana 24 Semana 48 TNX mg/kg cada 2 semanas + EO guiado por FT/GT (n = 28) Pacientes experiementados (multiclasses); CV ≥ cópias/ml; CD4+ ≥ 50 céls/ml (N = 82) TNX mg/kg cada 2 semanas + EO guiado por FT/GT (n = 27) PSGT, combined phenotype/genotype resistance assay For more information on this study, go online to: Placebo + EO guiado por FT/GT (n = 27) Aberto TNX mg/kg cada 2 semanas + novo EO Na falha virológica de qualquer braço Norris D, et al. IAC Abstract THLB0218.
 Pacientes experiementados (multiclasses); CV ≥ cópias/ml; CD4+ ≥ 50 céls/ml. (N = 82) TNX mg/kg cada 2 semanas. + EO guiado por FT/GT. (n = 27) PSGT, combined phenotype/genotype resistance assay. For more information on this study, go online to: Placebo. + EO guiado por FT/GT. (n = 27) Aberto. TNX mg/kg cada 2 semanas. + novo EO. Na falha virológica de qualquer braço. Norris D, et al. IAC Abstract THLB0218.")
66
TNX-355: Análise de Eficácia na semana 24 e 48
Endpoint Primário: Média de redução de CV na semana 24 15 mg/kg 10 mg/kg Placebo Sem24 Sem48 Sem24 Sem48 Sem24 Sem48 Significante ↑ CD4+ na Sem 48 (~ +50 cél/mm3) TNX-355 foi bem tolerado; eventos adversos comparáveis ao grupo com placebo -0,20 -0,14 -0,5 Redução Média de CV na semana 24 (log10 cópias/ml) For more information on this study, go online to: -0,71† -1,0 -0,95* -0,96‡ -1,16‡ -1,5 *p = 0,003 vs placebo. †p < 0,01 vs placebo. ‡p < 0,001 vs placebo. Norris D, et al. IAC Abstract THLB0218.
 TNX-355 foi bem tolerado; eventos adversos comparáveis ao grupo com placebo. -0,20. -0,14. -0,5. Redução Média de CV na semana 24 (log10 cópias/ml) For more information on this study, go online to: -0,71† -1,0. -0,95* -0,96‡ -1,16‡ -1,5. *p = 0,003 vs placebo. †p < 0,01 vs placebo. ‡p < 0,001 vs placebo. Norris D, et al. IAC Abstract THLB0218.")
67
PA-457: Resposta Virológica para Novos Inibidores de Maturação
Fase IIa, 10-dias monoterapia com PA-457 vs placebo em 32 pacientes[1] Dosando o PA-457 – oral (70h de meia-vida), tateando dose Mediana de redução de 1 log10 na CV com PA mg/dia Bem tolerado Nenhuma resistência percebida em estudos clínicos[2] -0.8 -0.4 -1.2 Mudança Mediana CV no dia 10 (log10 cópias/ml) PL (n = 8) 25 (n = 6) 50 (n = 6) 100 (n = 6) 200 (n = 6) PA-457 (mg/dia) +0,03 +0,05 -0,17 (p = 0,02) -0,48 (p = 0,004) -1,03 (p < 0,0001) Data were presented at the 2005 Interscience Conference on Antimicrobial Agents and Chemotherapy from a phase IIa study of 10 days of monotherapy with PA-457. This phase IIa trial consisted of HIV-infected patients who were not on any other therapy and who were randomized to receive placebo or 1 of 4 doses of PA-457 (25, 50, 100, 200 mg/day). The investigators observed a clear dose response, with substantial activity in the 200-mg once-daily arm (median HIV-1 RNA decrease at Day 10: ~ 1.0 log10 copies/mL). PA-457 was generally very well tolerated. There was no resistance to PA-457 observed in patients that received the drug over the 10-day period. Notably, this drug has a very long half-life of longer than 70 hours, so the fact that resistance was not rapidly selected for was a very positive outcome of this study. Further modeling data suggested that the dose with maximum antiviral effectiveness has not yet been reached and perhaps doses > 200 mg would have a more profound effect. For more information, please go online to: 1. Beatty G, et al. ICAAC Abstract H-416d. 2. Adamson C, et al. CROI Abstract 156.
, tateando dose. Mediana de redução de 1 log10 na CV com PA mg/dia. Bem tolerado. Nenhuma resistência percebida em estudos clínicos[2] Mudança Mediana CV no dia 10 (log10 cópias/ml) PL (n = 8) 25 (n = 6) 50 (n = 6) 100 (n = 6) 200 (n = 6) PA-457 (mg/dia) +0,03. +0,05. -0,17 (p = 0,02) -0,48 (p = 0,004) -1,03 (p < 0,0001) Data were presented at the 2005 Interscience Conference on Antimicrobial Agents and Chemotherapy from a phase IIa study of 10 days of monotherapy with PA-457. This phase IIa trial consisted of HIV-infected patients who were not on any other therapy and who were randomized to receive placebo or 1 of 4 doses of PA-457 (25, 50, 100, 200 mg/day). The investigators observed a clear dose response, with substantial activity in the 200-mg once-daily arm (median HIV-1 RNA decrease at Day 10: ~ 1.0 log10 copies/mL). PA-457 was generally very well tolerated. There was no resistance to PA-457 observed in patients that received the drug over the 10-day period. Notably, this drug has a very long half-life of longer than 70 hours, so the fact that resistance was not rapidly selected for was a very positive outcome of this study. Further modeling data suggested that the dose with maximum antiviral effectiveness has not yet been reached and perhaps doses > 200 mg would have a more profound effect. For more information, please go online to: 1. Beatty G, et al. ICAAC Abstract H-416d. 2. Adamson C, et al. CROI Abstract 156.")
68
Próxima Geração de Inibidores de Fusão
Dados de Animais Melhora da propriedade farmacocinética Potencial para 1x/semana Dados In-vitro Alta barreira genética Ativo contra vírus ENF-resistentes 100 Macaco Cynomolgus IV, 1 mg/Kg 1000 Clearance (ml/kg/hr) ENF TRI TRI ENF 10 100 Concentração Plasmática (mm3/ml) For more information, see the Capsule Summary at Diminuição de Atividade TRI-999 TRI-999 1 10 TRI-1144 TRI-1144 ENF 10 20 30 40 1 2 3 > 4 Tempo (H) (n) (6) (7) (8) (9) Números de Mutações Delmedico M, et al. CROI Abstract 48.
 ENF 40 TRI TRI ENF Concentração Plasmática (mm3/ml) For more information, see the Capsule Summary at Diminuição de Atividade. TRI-999. TRI TRI TRI ENF > 4. Tempo (H) (n) (6) (7) (8) (9) Números de Mutações. Delmedico M, et al. CROI Abstract 48.")
69
Tempo Estimado para Disponibilidade de Novos Anti-retrovirais
Inibidor de CXCR4 Inibidores de Entrada (anti-gp120, CCR5, CXCR4) GS-9137 Inibidores de Maturação MK-0518 TNX-355 Inibidores de Integrase Inibidor de CCR5 PA-457 2006 2007 2008 2009 2010 This slide is an estimated timeline of when the drugs discussed here may become available. It compares the novel agents on the top of the slide with new agents in existing classes on the bottom of the slide. This timeline is based on best estimates, but it seems likely that etravirine (TMC125) will be the next newly available agent. CCR5 inhibitors may be available next year, and integrase inhibitors might be available in late 2007 or early 2008 if all goes well. TMC278 IP Etravirina Brecanavir ITRNN Apricitabina ITRN
 GS Inibidores de Maturação. MK TNX-355. Inibidores de Integrase. Inibidor de CCR5. PA This slide is an estimated timeline of when the drugs discussed here may become available. It compares the novel agents on the top of the slide with new agents in existing classes on the bottom of the slide. This timeline is based on best estimates, but it seems likely that etravirine (TMC125) will be the next newly available agent. CCR5 inhibitors may be available next year, and integrase inhibitors might be available in late 2007 or early 2008 if all goes well. TMC278. IP. Etravirina. Brecanavir. ITRNN. Apricitabina. ITRN.")
70
Estudos Clínicos em Andamento com Novas Drogas no Brasil
TPV – Resist (resgate) Darunavir (TMC-114) – Power 1 (resgate), DRV X LPV-r (falha inicial) Etravirina (TMC-125) Etravirina + Darunavir – 206 (resgate) Etravirina X LPV-r – 227 (resgate - interrompido) TMC-278 (naïve) MK-0518 Fase II – resgate Fase III – resgate Fase III – naïve (não iniciado ainda) Vicriviroc – (resgate – em andamento) Smart
 Darunavir (TMC-114) – Power 1 (resgate), DRV X LPV-r (falha inicial) Etravirina (TMC-125) Etravirina + Darunavir – 206 (resgate) Etravirina X LPV-r – 227 (resgate - interrompido) TMC-278 (naïve) MK Fase II – resgate. Fase III – resgate. Fase III – naïve (não iniciado ainda) Vicriviroc – (resgate – em andamento) Smart.")
71
A resistência aos anti-retrovirais será o grande limitador da sobrevida dos pacientes que têm acesso ao tratamento em médio e longo prazo.

72
Conclusões: Passos Importantes para Reconquistar a Supressão Virológica
Focar para máxima supressão Se não for possível, manter a função imune e prevenir deterioração clínica Usar teste de resistência e o histórico de tratamento para estimar a suscetibilidade às drogas Considerar os testes de resistência anteriores Selecionar um novo esquema com pelo menos 2 drogas plenamente ativas Combinação de IP recentemente aprovadas (TPV/RTV, DRV/RTV) com agentes ativos ou nova classe (ex. ENF) Novas drogas em desenvolvimento aumentam a oportunidade para criar esquemas com ≥ 2 medicamentos ativos para pacientes fortemente experimentados
 com agentes ativos ou nova classe (ex. ENF) Novas drogas em desenvolvimento aumentam a oportunidade para criar esquemas com ≥ 2 medicamentos ativos para pacientes fortemente experimentados.")
Apresentações semelhantes

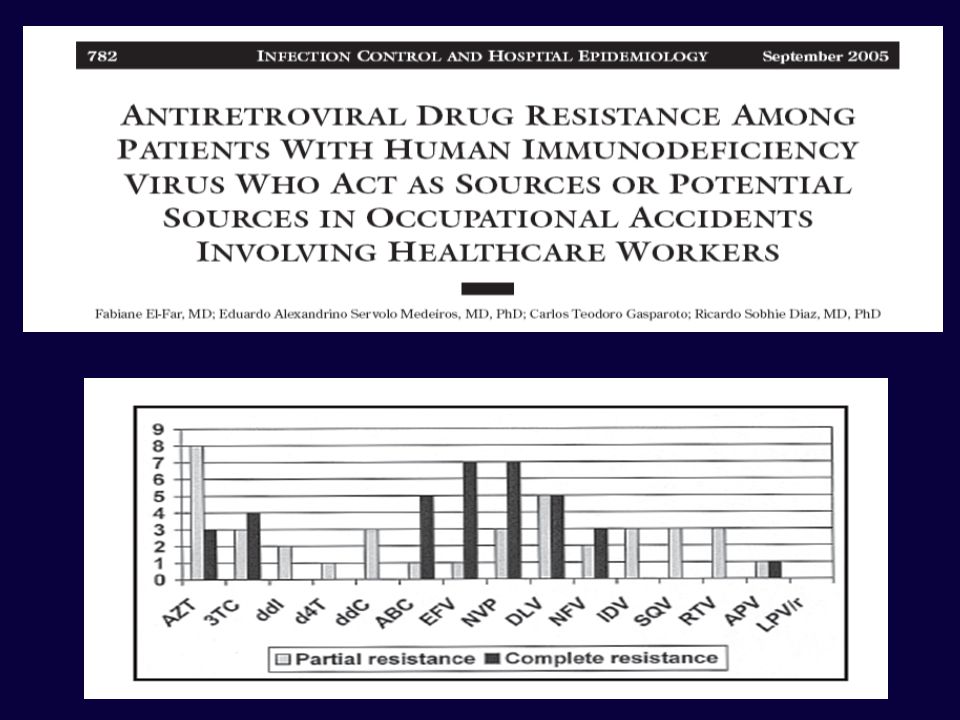

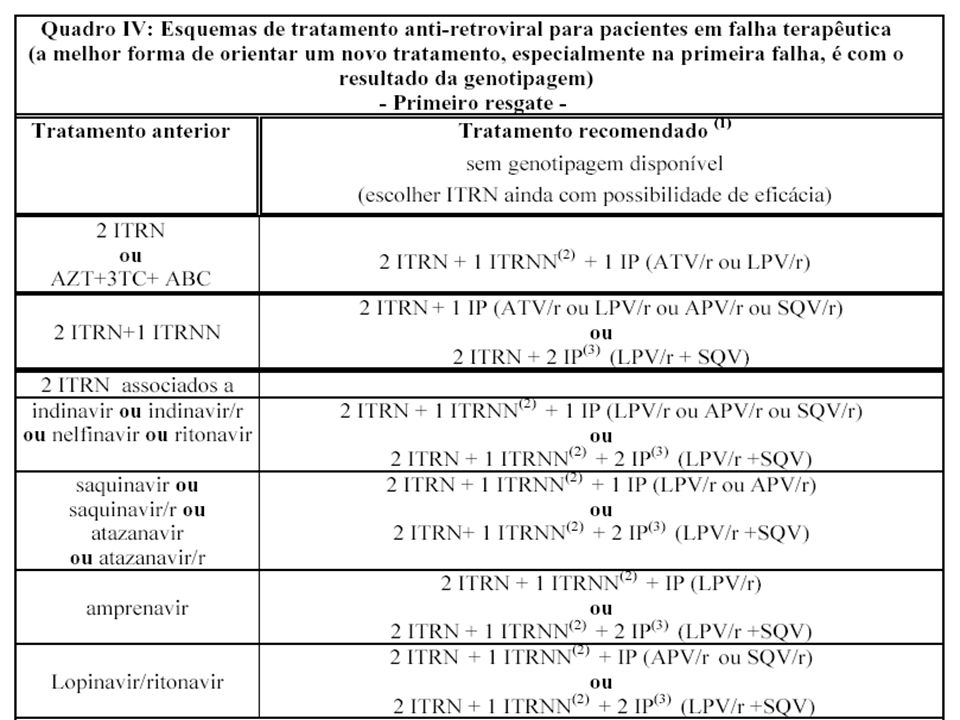














 em Pacientes com Falha ao Tratamento Anti-retroviral (TAR) e Resistência.>")




