Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Curso de Pós-Graduação em Dependência Química
Módulo 02 | Neurobiologia

2
Neurobiologia da Dependência química
Profa. Ana Regina Noto

3
Neurobiologia Cronograma do Módulo
3. Filme: “O poder do cérebro” Sexta Introdução 2. Neuroanatomia e neurofisiologia Sábado manhã 4. Psicofarmacologia I (sistemas de NT) 5. Reforço, Tolerância, S. Abstinência Sábado tarde Psicofarmacologia II (cinética e dinâmica das DR) 7. Filme: “Quem somos nós?” Domingo Bases genéticas da dependência 9. Debate final e Avaliação do módulo
 5. Reforço, Tolerância, S. Abstinência. Sábado tarde 6. Psicofarmacologia II (cinética e dinâmica das DR) 7. Filme: Quem somos nós Domingo 8. Bases genéticas da dependência. 9. Debate final e Avaliação do módulo.")
4
INTRODUÇÃO

5
Categoria de drogas psicoativas que podem provocar DEPENDÊNCIA
PSICOTRÓPICAS Atuam no Sistema Nervoso Central (SNC) e provocam alterações de comportamento Categoria de drogas psicoativas que podem provocar DEPENDÊNCIA
 e provocam alterações de comportamento. Categoria de drogas psicoativas que podem provocar DEPENDÊNCIA.")
6
Dependência Estado resultante da
interação entre um organismo vivo e uma substância, caracterizado por: Modificações de comportamento e outras reações que incluem: Impulso a utilizar a substância de modo contínuo ou periódico com a finalidade de experimentar seus efeitos psíquicos ou de evitar o desconforto da privação Organização Mundial de Saúde

7
Dependência: Evolução do conceito
psicologia sociologia antropologia MODELO MORAL “Falta de caráter” Escolha pessoal MODELO MÉDICO DOENÇA Lei do “tudo ou nada” Falta de controle Meta: abstinência SÍNDROME Contínuo-dinâmico Moderação Comportamento aprendido Sintoma Escolha Movimento de Temperança Sobell & Sobell 1980 Neuro-ciências Lei seca Alcoólicos Anônimos 1940 Jellinek 1960 G.Edwards 1976 1900 2000

8
Modelo Biopsicossocial
Dependência: Modelo Biopsicossocial MÉDICO DOENÇA - SÍNDROME SOCIAL SINTOMA MACROSSOCIAL PSICOLÓGICO SINTOMA ESCOLHA COMPORTAMENTO APRENDIDO RELACIONAL

9
Perspectiva biológica do avanço da dependência (sinais e sintomas)
Abstinência Uso exporádico Abuso Dependência Leve Dependência Moderada Dependência Grave Reforço Perspectiva biológica dos sinais e sintomas Síndrome de Abstinência Fissura Tolerância

10
Dependência: Principais características
1. Desejo ou compulsão 2. Dificuldade em controlar o consumo 3. Abandono de prazeres e interesses alternativos 4. Persistência no uso a despeito da evidência de conseqüências nocivas 5. Síndrome de Abstinência 6. Tolerância Organização Mundial de Saúde

11
NEUROANATOMIA E DEPENDÊNCIA

12
senso-percepção motivação coordenação motora julgamento entre outros
DEPENDÊNCIA Dependência envolve transtornos da função cerebral pelo uso de substâncias. Os processos mais alterados são: senso-percepção motivação coordenação motora julgamento entre outros

13
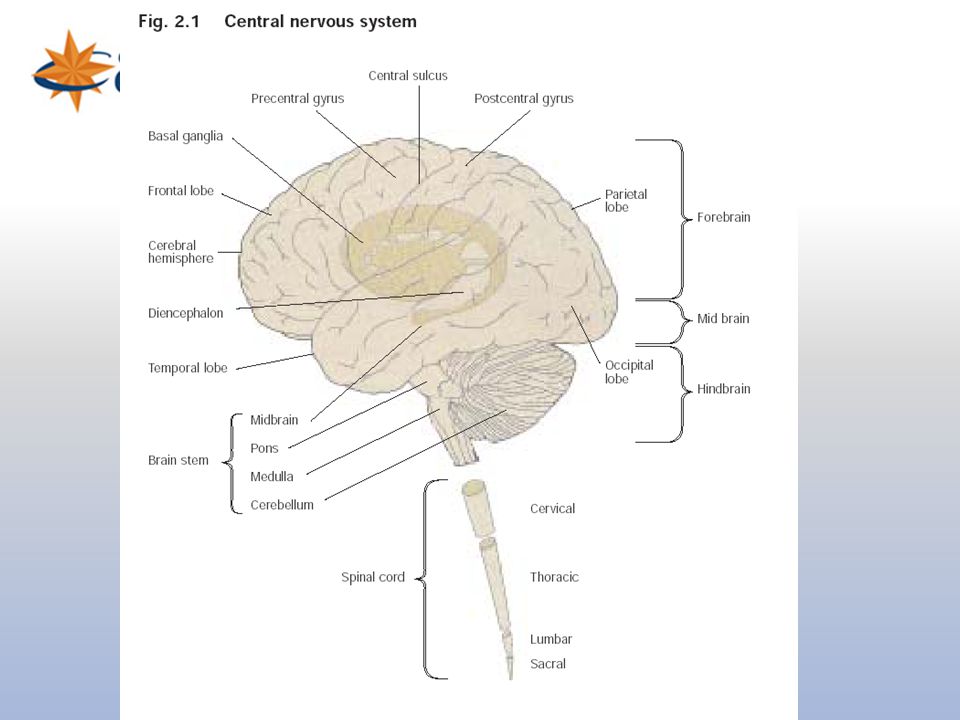
Slide 2: The brain and spinal cord
The central nervous system is composed of both the brain and the spinal cord. Describe the brain as a functional unit; it is made up of billions of nerve cells (neurons) that communicate with each other using electrical and chemical signals.
 that communicate with each other using electrical and chemical signals.")
15
Sistema Nervoso Central
CÓRTEX HIPOTÁLAMO HIPOCAMPO AMIGDALA GÂNGLIOS DA BASE NIDA, 2005 NIDA, 2005

16
Slide 3: Brain regions and neuronal pathways
Certain parts of the brain govern specific functions. Point to areas such as the sensory (orange), motor (blue) and visual cortex (yellow) to highlight their specific functions. Point to the cerebellum (pink) for coordination and to the hippocampus (green) for memory. Indicate that nerve cells or neurons connect one area to another via pathways to send and integrate information. The distances that neurons extend can be short or long. For example; point to the reward pathway (orange). Explain that this pathway is activated when a person receives positive reinforcement for certain behaviors ("reward"). Indicate that you will explain how this happens when a person takes an addictive drug. As another example, point to the thalamus (magenta). This structure receives information about pain coming from the body (magenta line within the spinal cord), and passes the information up to the cortex. Tell the audience that you can look at this in more detail.
, motor (blue) and visual cortex (yellow) to highlight their specific functions. Point to the cerebellum (pink) for coordination and to the hippocampus (green) for memory. Indicate that nerve cells or neurons connect one area to another via pathways to send and integrate information. The distances that neurons extend can be short or long. For example; point to the reward pathway (orange). Explain that this pathway is activated when a person receives positive reinforcement for certain behaviors ( reward ). Indicate that you will explain how this happens when a person takes an addictive drug. As another example, point to the thalamus (magenta). This structure receives information about pain coming from the body (magenta line within the spinal cord), and passes the information up to the cortex. Tell the audience that you can look at this in more detail.")
18
Slide 12: Activation of the reward pathway by an electrical stimulus
The discovery of the reward pathway was achieved with the help of animals such as rats. Rats were trained to press a lever for a tiny electrical jolt to certain parts of the brain. Show that when an electrode is placed in the nucleus accumbens, the rat keeps pressing the lever to receive the small electrical stimulus because it feels pleasurable. This rewarding feeling is also called positive reinforcement. Point to an area of the brain close to the nucleus accumbens. Tell the audience that when the electrode is placed there, the rat will not press the lever for the electrical stimulus because stimulating neurons in a nearby area that does not connect with the nucleus accumbens does not activate the reward pathway. The importance of the neurotransmitter dopamine has been determined in these experiments because scientists can measure an increased release of dopamine in the reward pathway after the rat receives the reward. And, if the dopamine release is prevented (either with a drug or by destroying the pathway), the rat won't press the bar for the electrical jolt. So with the help of the rats, scientists figured out the specific brain areas as well as the neurochemicals involved in the reward pathway.
, the rat won t press the bar for the electrical jolt. So with the help of the rats, scientists figured out the specific brain areas as well as the neurochemicals involved in the reward pathway.")
19
Slide 8: Reward: drug self-administration
Introduce the concept of positive reinforcement or reward. Explain that rats will press a bar to get an injection of cocaine or heroin (self-administration - shown on the left). The rat keeps pressing to get more cocaine or heroin because the drugs make the rat feel so good. This is called positive reinforcement, or reward. Natural rewards include food, water and sex - each is required to maintain survival of our species. Animals and people will continue to exhibit a behavior that is rewarding - and they will cease that behavior when the reward is no longer present. Explain that there is actually a part of the brain that is activated by natural rewards and by artificial rewards such as addictive drugs. This part of the brain is called the reward system. Neuroscientists have been able to pinpoint the exact parts of the brain involved, with the help of the rats. Point to the cartoon on the right and explain that rats will also self-administer addictive drugs directly into their brains -but only into a specific area of the reward system. If the injection needle is moved less than a millimeter away from this crucial area, the rat won't press the lever for more drug. So based on information from working with the rats, scientists have drawn a map of the brain, and located the structures and pathways that are activated when an addictive drug is taken voluntarily. Tell the students that you will show them this "map".
. The rat keeps pressing to get more cocaine or heroin because the drugs make the rat feel so good. This is called positive reinforcement, or reward. Natural rewards include food, water and sex - each is required to maintain survival of our species. Animals and people will continue to exhibit a behavior that is rewarding - and they will cease that behavior when the reward is no longer present. Explain that there is actually a part of the brain that is activated by natural rewards and by artificial rewards such as addictive drugs. This part of the brain is called the reward system. Neuroscientists have been able to pinpoint the exact parts of the brain involved, with the help of the rats. Point to the cartoon on the right and explain that rats will also self-administer addictive drugs directly into their brains -but only into a specific area of the reward system. If the injection needle is moved less than a millimeter away from this crucial area, the rat won t press the lever for more drug. So based on information from working with the rats, scientists have drawn a map of the brain, and located the structures and pathways that are activated when an addictive drug is taken voluntarily. Tell the students that you will show them this map .")
20
Recompensas Naturais Comida Água Sexo

21
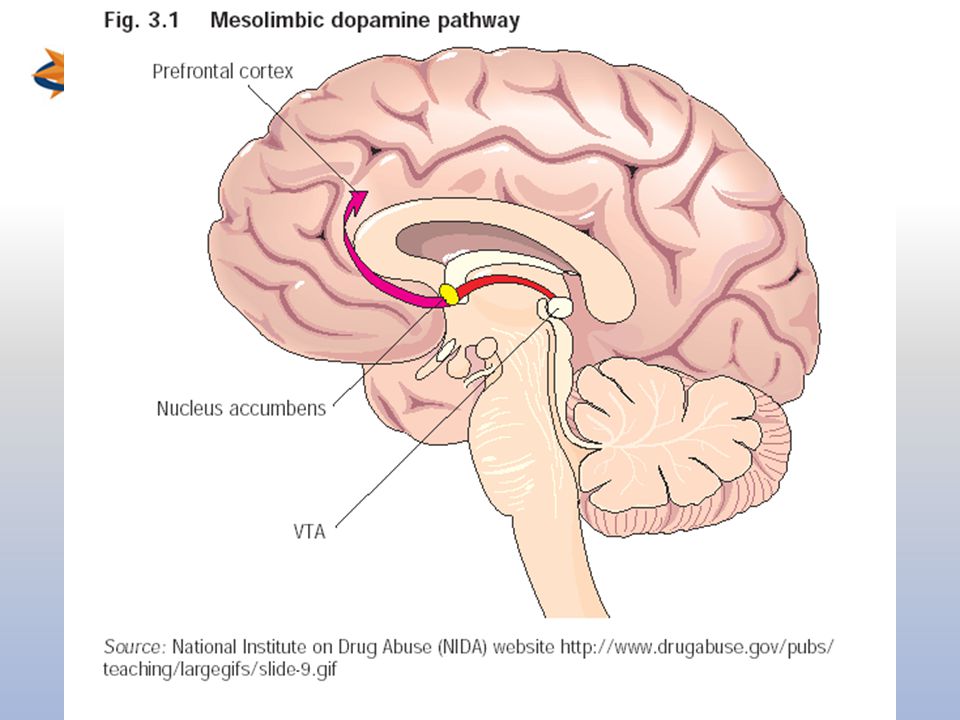
Slide 30: Summary; addictive drugs activate the reward system via increasing dopamine neurotransmission In this last slide, the reward pathway is shown along with several drugs that have addictive potential. Just as heroin (morphine) and cocaine activate the reward pathway in the VTA and nucleus accumbens, other drugs such as nicotine and alcohol activate this pathway as well, although sometimes indirectly (point to the globus pallidus, an area activated by alcohol that connects to the reward pathway). While each drug has a different mechanism of action, each drug increases the activity of the reward pathway by increasing dopamine transmission. Because of the way our brains are designed, and because these drugs activate this particular brain pathway for reward, they have the ability to be abused. Thus, addiction is truely a disease of the brain. As scientists learn more about this disease, they may help to find an effective treatment strategy for the recovering addict.
 and cocaine activate the reward pathway in the VTA and nucleus accumbens, other drugs such as nicotine and alcohol activate this pathway as well, although sometimes indirectly (point to the globus pallidus, an area activated by alcohol that connects to the reward pathway). While each drug has a different mechanism of action, each drug increases the activity of the reward pathway by increasing dopamine transmission. Because of the way our brains are designed, and because these drugs activate this particular brain pathway for reward, they have the ability to be abused. Thus, addiction is truely a disease of the brain. As scientists learn more about this disease, they may help to find an effective treatment strategy for the recovering addict.")
22
NEUROFISIOLOGIA

23
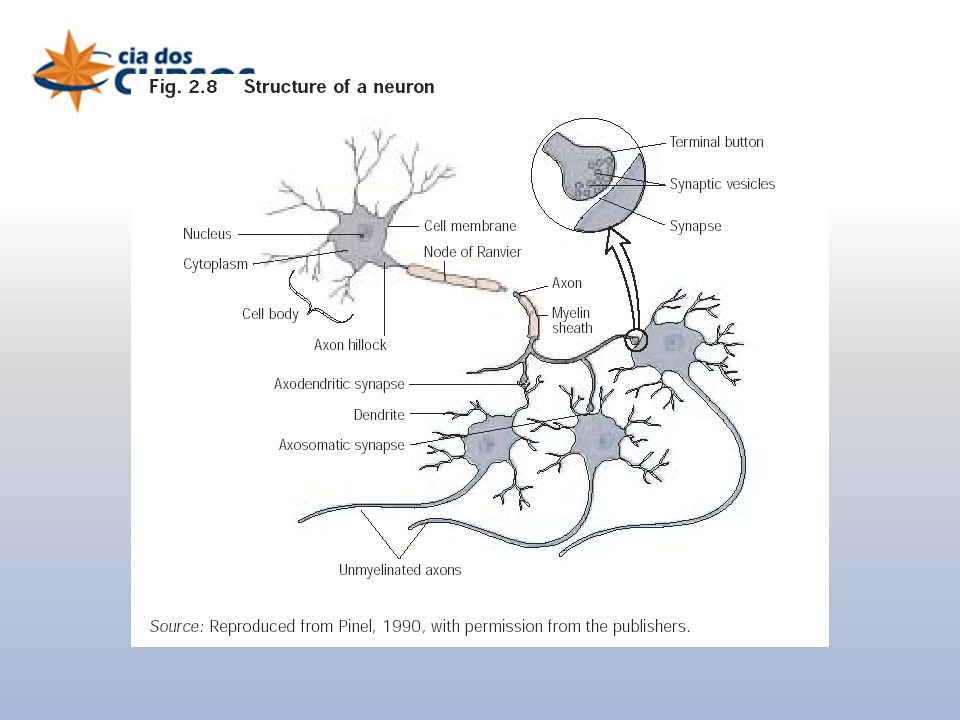
NEURÔNIO axônio Corpo celular dendritos
1-1 Stahl S M, Essential Psychopharmacology (2000)
")
25
Slide 6: Impulse flow Explain the normal direction of the flow of information (electrical and chemical). An electrical impulse (the action potential) travels down the axon toward the terminal. Point to the terminal. The terminal makes a connection with the dendrite of neighboring neuron, where it passes on chemical information. The area of connection is called the synapse. While the synapse between a terminal and a dendrite (shown here) is quite typical, other types of synapses exist as well--for example a synapse can occur between a terminal and a soma or axon.
. An electrical impulse (the action potential) travels down the axon toward the terminal. Point to the terminal. The terminal makes a connection with the dendrite of neighboring neuron, where it passes on chemical information. The area of connection is called the synapse. While the synapse between a terminal and a dendrite (shown here) is quite typical, other types of synapses exist as well--for example a synapse can occur between a terminal and a soma or axon.")
26
Potencial de ação

28
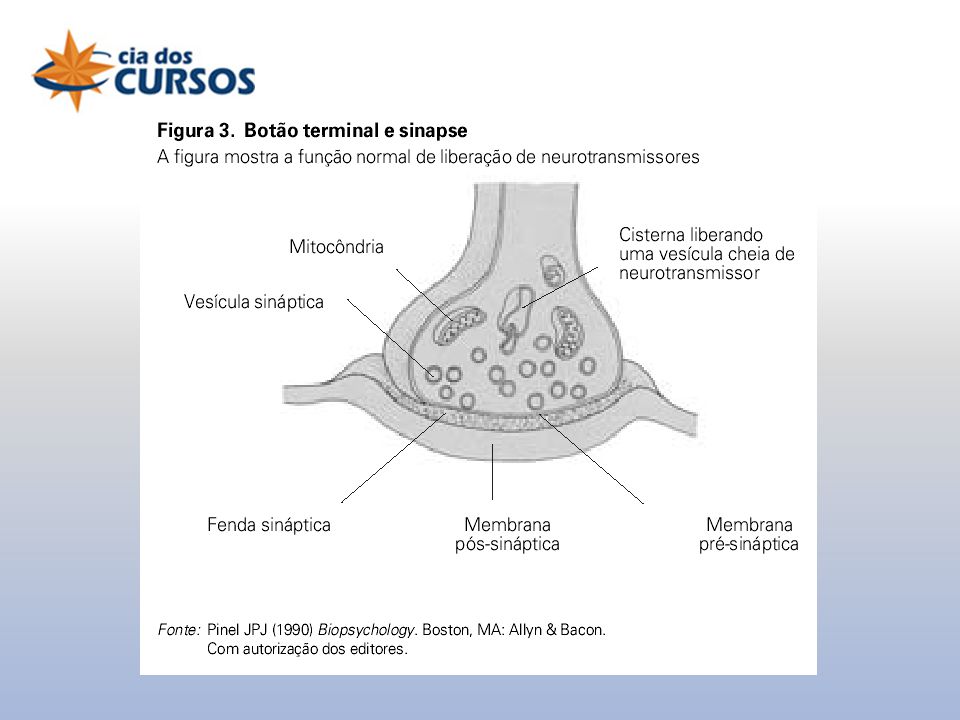
Comunicação química entre neurônios
SINAPSE NEURÔNIO PRÉ-SINAPTICO Vesículas sinapticas Neurotransmissores (NT) Receptores NEURÔNIO PÓS-SINAPTICO STAHL, 2000
 Receptores. NEURÔNIO PÓS-SINAPTICO. STAHL,")
29
“Caminhos” dos neurotransmissores
SINAPSE NEURÔNIO PRÉ-SINAPTICO Recaptação (NT volta para o neurônio pré-sinaptico) Liberação Metabolismo (inativação do NT com auxílio de uma enzima) NEURÔNIO PÓS-SINAPTICO STAHL, 2000
 Liberação. Metabolismo (inativação do NT com auxílio de uma enzima) NEURÔNIO PÓS-SINAPTICO. STAHL,")
30
SISTEMAS DE NEUROTRANSMISSÃO
PSICOFARMACOLOGIA 1 SISTEMAS DE NEUROTRANSMISSÃO Dopaminérgico Noradrenérgico Serotonérgico Colinérgico Gabaérgico

31
Neurotransmissores Substâncias químicas (moléculas) que transmitem “mensagens” entre neurônios Ex: DOPAMINA OH- CH2 – CH2 OH- NH2

32
NEUROTRANSMISSORES DOPAMINA (DA) - Sistema Dopaminérgico
NORADRENALINA(NA) – Sistema Noradrenérgico SEROTONINA (5HT) – Sistema Serotonérgico ACETILCOLINA (Ach)– Sistema Colinérgico GABA – Sistema Gabaérgico GLUTAMATO – Sistema Glutamatérgico
 – Sistema Noradrenérgico. SEROTONINA (5HT) – Sistema Serotonérgico. ACETILCOLINA (Ach)– Sistema Colinérgico. GABA – Sistema Gabaérgico. GLUTAMATO – Sistema Glutamatérgico.")
33
Receptores Complexos moleculares, localizados na membrana do neurônio, responsáveis por receber “mensagens” Ex:

34
IONOTRÓPICOS (rápidos) METABOTRÓPICOS (lentos)
TIPOS DE RECEPTORES IONOTRÓPICOS (rápidos) METABOTRÓPICOS (lentos) Controlam canais IÔNICOS (entrada e saída de íons) Controlam “segundo mensageiro” ex: Proteína G (transmitem a mensagem química, para desencadear outros eventos - metabolismo)
 METABOTRÓPICOS (lentos) Controlam canais IÔNICOS. (entrada e saída de íons) Controlam segundo mensageiro ex: Proteína G. (transmitem a mensagem química, para desencadear outros eventos - metabolismo)")
35
RECEPTORES E SISTEMAS DE NEUROTRANSMISSÃO
Cada neurotransmissor tem seus receptores específicos DOPAMINA (DA) – D1, D2 NORADRENALINA – alfa, beta SEROTONINA (5HT) – 5HT1 (a, b, c e d), 5HT2 ACETILCOLINA – Nicotínico e Muscarínico GABA – GABAa e GABAb GLUTAMATO – NMDA, AMPA e cainato
 – D1, D2. NORADRENALINA – alfa, beta. SEROTONINA (5HT) – 5HT1 (a, b, c e d), 5HT2. ACETILCOLINA – Nicotínico e Muscarínico. GABA – GABAa e GABAb. GLUTAMATO – NMDA, AMPA e cainato.")
36
Metabolismo Ex: inativação da dopamina Dopamina HVA ENZIMAS
MAO COMT Dopamina HVA (ácido homovanílico) ENZIMAS ENZIMAS: substâncias que catalizam (aceleram) reações Sem elas, as reações são mais lentas ou nem mesmo acontecem MAO – Monoamonoxidade (uma das principais enzimas, responsével pela inativação da dopamina, noradrenalina e serotonina)
 ENZIMAS. ENZIMAS: substâncias que catalizam (aceleram) reações. Sem elas, as reações são mais lentas ou nem mesmo acontecem. MAO – Monoamonoxidade (uma das principais enzimas, responsével pela inativação da dopamina, noradrenalina e serotonina)")
37
Comunicação Dopaminérgica HVA (ácido homovanílico)
Dopamina MAO HVA (ácido homovanílico) (ou COMT) D1 STAHL, 2000
 (ou COMT) D1. STAHL,")
38
- Nigro- estriatal (relacionada ao sistema motor - Parkinson)
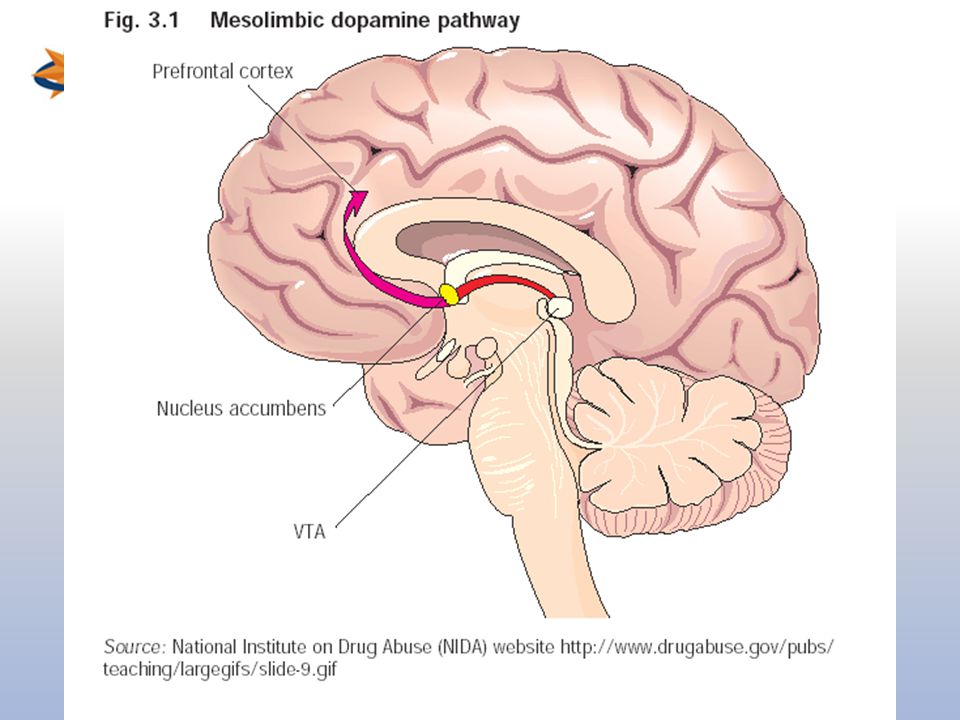
VIAS DOPAMINÉRGICAS Mesolímbica (relacionada agressividade, reforço) - Nigro- estriatal (relacionada ao sistema motor - Parkinson) - Meso-cortical (relacionada doenças afetivas - Esquizofrenia) - Túbero infundibular (relacionada a hormônios - GH) - Retinal
 - Nigro- estriatal (relacionada ao sistema motor - Parkinson) - Meso-cortical (relacionada doenças afetivas - Esquizofrenia) - Túbero infundibular (relacionada a hormônios - GH) - Retinal.")
39
FUNÇÕES RELACIONADAS AO SISTEMA DOPAMINÉRGICO
Reforço Agressividade Sistema motor Afetividade

40
Drogas de abuso – sistema dopaminérgico
Diminui a recaptação (ex: COCAÍNA) Aumenta a liberação (ex: ANFETAMINAS) Dopamina STAHL, 2000
 Aumenta a liberação (ex: ANFETAMINAS) Dopamina. STAHL,")
41
Comunicação Noradrenérgica
MAO Noradrenalina HVMA (ác. homovanílmandélico) (ou COMT) Receptores: alfa ou beta STAHL, 2000
 (ou COMT) Receptores: alfa ou beta. STAHL,")
42
VIAS NORADRENÉRGICAS Feixe noradrenérgico ventral
Feixe noradrenérgico dorsal

43
FUNÇÕES RELACIONADAS AO SISTEMA NORADRENÉRGICO
Vigília (acordar) Humor Recompensa Controle da PA (Pressão Arterial)
 Humor. Recompensa. Controle da PA (Pressão Arterial)")
44
DROGAS QUE ATUAM NO SISTEMA NORADRENÉRGICO
Diminui a recaptação (ex: COCAÍNA) Aumenta a liberação (ex: ANFETAMINAS) Noradrenalina STAHL, 2000
 Aumenta a liberação (ex: ANFETAMINAS) Noradrenalina. STAHL,")
45
Comunicação Serotonérgica 5HIAA (ác. 5 hidroxi indol acético)
MAO Serotonina (5HT) 5HIAA (ác. 5 hidroxi indol acético) Receptores: 5HT1, 5HT2 STAHL, 2000
 5HIAA (ác. 5 hidroxi indol acético) Receptores: 5HT1, 5HT2. STAHL,")
46
FUNÇÕES RELACIONADAS AO SISTEMA SEROTONÉRGICO
Alterações sensoriais (pode propicia alucinações) Humor (melhora) Temperatura (desregula) Apetite (diminui) Dor (diminui)
 Humor (melhora) Temperatura (desregula) Apetite (diminui) Dor (diminui)")
47
DROGAS QUE ATUAM NO SISTEMA SEROTONÉRGICO
Diminui a recaptação (ex: fluoxetina, êxtase) Aumenta a liberação (ex: êxtase) Serotonina Agonista (ex: LSD, êxtase, DMT, mescalina) STAHL, 2000
 Aumenta a liberação (ex: êxtase) Serotonina. Agonista (ex: LSD, êxtase, DMT, mescalina) STAHL,")
48
TIPOS DE RELAÇÃO ENTRE DROGA-RECEPTOR
AGONISTAS: drogas que se acoplam ao receptor produzindo efeitos, como “falso-neurotransmissores” (ex: LSD é agonista dos receptores 5HT2a) ANTAGONISTAS: drogas que se acoplam ao receptor e NÃO produzem efeitos, inclusive, impedem a ação dos neurotransmissores (por “ocupar o espaço”)
 ANTAGONISTAS: drogas que se acoplam ao receptor e NÃO produzem efeitos, inclusive, impedem a ação dos neurotransmissores (por ocupar o espaço )")
49
Comunicação Colinérgico
AchE Acetilcolina (Ach) Acetato + colina Receptores: M1, M2 STAHL, 2000
 Acetato + colina. Receptores: M1, M2. STAHL,")
50
FUNÇÕES RELACIONADAS AO SISTEMA COLINÉRGICO
Aprendizado e Memória (Dç Alzheimer) Motricidade (Dç Parkinson) Vigília
 Motricidade (Dç Parkinson) Vigília.")
51
DROGAS QUE ATUAM NO SISTEMA COLINÉRGICO
- Anticolinérgicos (Ex: Lírio Bc, Artane, etc)
")
52
Comunicação Gabaérgica
GABA t GABA Succinil semi aldeído Receptores: GABA a STAHL, 2000

53
Cl- O CLORO HIPERPOLARIZA A MEMBRANA, DIFICULTANDO A OCORRÊNCIA DE POTENCIAL DE AÇÃO

54
DROGAS QUE ATUAM NO SISTEMA GABAÉRGICO
Benzodiazepínicos: facilitam a ação do GABA por modificar a configuração do receptor GABAa (agonista alostérico)
")
55
Cogumelos (Psiloscibe sp)
DROGAS PSICOTRÓPICAS Chaloult, 1971 ESTIMULANTES Cocaína Anfetamina DEPRESSORAS Álcool Heroína Solventes Benzodiazepínicos Ecstasy Maconha LSD Cogumelos (Psiloscibe sp) DMT PERTURBADORAS - ALUCINÓGENAS (psicodislépticas) Chaloult, 1971; Abraham et al., 1996; Kovar, 1998
 DMT. PERTURBADORAS - ALUCINÓGENAS. (psicodislépticas) Chaloult, 1971; Abraham et al., 1996; Kovar,")
56
Fatores que influenciam os efeitos das drogas
Droga e sua ação no SNC Dose administrada e farmacocinética Tempo de uso Contexto de uso Estado psicológico

57
COCAÍNA, ANFETAMINAS, CAFEÍNA, NICOTINA
ESTIMULANTES COCAÍNA, ANFETAMINAS, CAFEÍNA, NICOTINA

58
Estimulantes = Psicoanalépticos
Aumento da atividade do SNC - Alteração “quantitativa” Aumento da energia, vigor físico, disposição, vigília e diminuição do cansaço e da fome Além do uso “recreativo”, são empregadas nos remédios moderadores de apetite

59
COCAÍNA Capa cocaína

60
Slide 25: Snorting vs smoking cocaine: different addictive liabilities
Historically cocaine abuse involved snorting the powdered form (the hydrochloride salt). When cocaine is processed to form the free base, it can be smoked. Heating the hydrochloride salt form of cocaine will destroy it; the free base can be volatilized at high temperature without any destruction of the compound. Smoking gets the drug to the brain more quickly than does snorting. Show the audience why this happens. Snorting requires that the cocaine travels from the blood vessels in the nose to the heart (blue arrow), where it gets pumped to the lungs (blue arrow) to be oxygenated. The oxygenated blood (red arrows) carrying the cocaine then travels back to the heart where it is pumped out to the organs of the body, including the brain. However, smoking bypasses much of this--the cocaine goes from the lungs directly to the heart and up to the brain. The faster a drug with addictive liability reaches the brain, the more likely it will be abused. Thus, the time between taking the drug and the positive reinforcing or rewarding effects that are produced can determine the likelihood of abuse.
. When cocaine is processed to form the free base, it can be smoked. Heating the hydrochloride salt form of cocaine will destroy it; the free base can be volatilized at high temperature without any destruction of the compound. Smoking gets the drug to the brain more quickly than does snorting. Show the audience why this happens. Snorting requires that the cocaine travels from the blood vessels in the nose to the heart (blue arrow), where it gets pumped to the lungs (blue arrow) to be oxygenated. The oxygenated blood (red arrows) carrying the cocaine then travels back to the heart where it is pumped out to the organs of the body, including the brain. However, smoking bypasses much of this--the cocaine goes from the lungs directly to the heart and up to the brain. The faster a drug with addictive liability reaches the brain, the more likely it will be abused. Thus, the time between taking the drug and the positive reinforcing or rewarding effects that are produced can determine the likelihood of abuse.")
61
Slide 26: Localization of cocaine "binding sites"
When a person smokes or snorts cocaine, it reaches all areas of the brain, but it binds to sites in some very specific areas. These are highlighted with the yellow dots; the VTA, the nucleus accumbens and the caudate nucleus (the largest structure). Point out that cocaine binds especially in the reward areas that you have just discussed. The binding of cocaine in other areas such as the caudate nucleus can explain other effects such as increased stereotypic (or repetitive) behaviors (pacing, nail-biting, scratching, etc..)
. Point out that cocaine binds especially in the reward areas that you have just discussed. The binding of cocaine in other areas such as the caudate nucleus can explain other effects such as increased stereotypic (or repetitive) behaviors (pacing, nail-biting, scratching, etc..)")
62
x Mecanismo de ação principal:
Cocaína diminui a recaptação de dopamina e noradrenalina x COCAÍNA Diminui a recaptação, aumentando a concentração de dopamina na fenda sinaptica Slide 27: Dopamine binding to receptors and uptake pumps in the nucleus accumbens; the action of cocaine Explain that cocaine binds to sites in areas of the brain that are rich in dopamine synapses such as the VTA and the nucleus accumbens. Review dopamine transmission in the close-up of a synapse in the nucleus accumbens. Point to dopamine (inside the terminal) that is released into the synaptic space. The dopamine binds to dopamine receptors and then is taken up by uptake pumps back into the terminal. Now show what happens when cocaine is present (yellow). Cocaine binds to the uptake pumps and prevents them from transporting dopamine back into the neuron terminal. So more dopamine builds up in the synaptic space and it is free to activate more dopamine receptors. This is the same effect that you showed in an earlier slide with morphine, where morphine increased dopamine release from the terminal to produce more dopamine in the synaptic space. Dopamina
 that is released into the synaptic space. The dopamine binds to dopamine receptors and then is taken up by uptake pumps back into the terminal. Now show what happens when cocaine is present (yellow). Cocaine binds to the uptake pumps and prevents them from transporting dopamine back into the neuron terminal. So more dopamine builds up in the synaptic space and it is free to activate more dopamine receptors. This is the same effect that you showed in an earlier slide with morphine, where morphine increased dopamine release from the terminal to produce more dopamine in the synaptic space. Dopamina.")
63
Slide 26: Localization of cocaine "binding sites"
When a person smokes or snorts cocaine, it reaches all areas of the brain, but it binds to sites in some very specific areas. These are highlighted with the yellow dots; the VTA, the nucleus accumbens and the caudate nucleus (the largest structure). Point out that cocaine binds especially in the reward areas that you have just discussed. The binding of cocaine in other areas such as the caudate nucleus can explain other effects such as increased stereotypic (or repetitive) behaviors (pacing, nail-biting, scratching, etc..)
. Point out that cocaine binds especially in the reward areas that you have just discussed. The binding of cocaine in other areas such as the caudate nucleus can explain other effects such as increased stereotypic (or repetitive) behaviors (pacing, nail-biting, scratching, etc..)")
64
Principais efeitos da cocaína
Aumento da energia Aumento da disposição Vigor físico Sensação de poder Diminuição do cansaço Redução do apetite/fome

65
Slide 28: Cocaine dependence and activation of the reward pathway
Review where cocaine binds within the reward pathway (the VTA and the nucleus accumbens). As a result of cocaine's actions in the nucleus accumbens (point to the dots of cocaine in the VTA and nucleus accumbens), there are increased impulses leaving the nucleus accumbens to activate the reward system. This pathway can be activated even in the absence of cocaine, i.e. during craving. Indicate that with repeated use of cocaine, the body relies on this drug to maintain rewarding feelings. The person is no longer able to feel the positive reinforcement or pleasurable feelings of natural rewards (i.e. food, water, sex)--the person is only able to feel pleasure from the cocaine. Thus the user becomes dependent and when the cocaine is no longer present, anhedonia (inability to feel pleasure) and depression emerge as part of a withdrawal syndrome. To avoid this, the user goes back to the cocaine. Unlike the example for morphine, the cocaine addiction (i.e. craving) and the dependence (i.e. anhedonia) both involve structures in the reward pathway.
. As a result of cocaine s actions in the nucleus accumbens (point to the dots of cocaine in the VTA and nucleus accumbens), there are increased impulses leaving the nucleus accumbens to activate the reward system. This pathway can be activated even in the absence of cocaine, i.e. during craving. Indicate that with repeated use of cocaine, the body relies on this drug to maintain rewarding feelings. The person is no longer able to feel the positive reinforcement or pleasurable feelings of natural rewards (i.e. food, water, sex)--the person is only able to feel pleasure from the cocaine. Thus the user becomes dependent and when the cocaine is no longer present, anhedonia (inability to feel pleasure) and depression emerge as part of a withdrawal syndrome. To avoid this, the user goes back to the cocaine. Unlike the example for morphine, the cocaine addiction (i.e. craving) and the dependence (i.e. anhedonia) both involve structures in the reward pathway.")
66
Álcool, solventes, benzodiazepínicos, barbitúricos
DEPRESSORES Álcool, solventes, benzodiazepínicos, barbitúricos

67
BENZODIAZEPÍNICOS

68
Depressoras = Psicolépticos
Diminuição da atividade do SNC - Alteração “quantitativa” Lentidão, sonolência, apatia, redução da coordenação motora, dificuldade de concentração e redução da memória. Além do uso “recreativo”, são empregadas nos remédios ansiolíticos e hipnóticos

69
Mecanismo de ação principal: Facilitam a ação do Gaba
GABA a STAHL, 2000

70
Cl- O CLORO HIPERPOLARIZA A MEMBRANA, DIFICULTANDO A OCORRÊNCIA DE POTENCIAL DE AÇÃO e portanto ocorre “depressão” de várias áreas do SNC

71
ÁLCOOL Capa álcool

73
ÁLCOOL Variações individuais (ex: gênero), alimentação, padrão de uso.
Efeito bifásico: 1º estimulante (ação em DA e NA) 2º depressor (ação em GABA e Glutamato). Gravidez (Síndrome fetal) e amamentação
 2º depressor (ação em GABA e Glutamato). Gravidez (Síndrome fetal) e amamentação.")
74
ALUCINÓGENOS

75
Classificação dos alucinógenos
De acordo com a similaridade estrutural e funcional INDÓLICOS (indolalquilaminas) Ex: LSD, Pscilocibina, Ibogaína, DMT 2. FEAs (feniletilaminas) Ex: Mescalina, MDMA (ecstasy) 3. ANTICOLINÉRGICOS Ex: atropina, escopolamina, triexafenidil (Artane®) 4. PCP e ketamina (anestésicos dissociativos) 5. CANABINÓIDES Ex: maconha Abraham et al., 1996 Kovar, 1998
 Ex: LSD, Pscilocibina, Ibogaína, DMT. 2. FEAs (feniletilaminas) Ex: Mescalina, MDMA (ecstasy) 3. ANTICOLINÉRGICOS. Ex: atropina, escopolamina, triexafenidil (Artane®) 4. PCP e ketamina (anestésicos dissociativos) 5. CANABINÓIDES. Ex: maconha. Abraham et al., 1996 Kovar,")
76
Perturbadoras, alucinógenas = Psicodislépticos
Modificação da atividade do SNC - Alteração “qualitativa” Confusão mental (delírios e alucinações), despersonalização, distorção de tempo e espaço. Não tem indicação clínica (exceto alguns alucinógenos secundários, como anticolinérgicos e anestésicos dissociativos)
, despersonalização, distorção de tempo e espaço. Não tem indicação clínica (exceto alguns alucinógenos secundários, como anticolinérgicos e anestésicos dissociativos)")
77
INDÓLICOS Pscilocibina Ibogaína DMT LSD

78
serotonina MDMA LSD Psilocibina Mescalina 5HT2A 5HT2A
13-10 Stahl S M, Essential Psychopharmacology (2000)
")
79
Interação 5HT-DA Substância negra Núcleos da rafe
11-17 Stahl S M, Essential Psychopharmacology (2000)
")
80
Efeitos agudos - intensos
LSD - Efeitos Efeitos agudos - intensos Entre outros... Sinestesia Cinestesia

81
ÊXTASE

82
Farmacocinética da MDMA
(ecstasy) Início: min Aumento: min Platô horas EFEITOS 1 2 3 4 5 6 7 8 9 10 11 12 HORAS Curran & Travil, 1997
 Início: min. Aumento: 5-20 min. Platô 2-3 horas. EFEITOS HORAS. Curran & Travil,")
83
Mecanismo de ação da MDMA
SINAPSE SEROTONÉRGICO AGONISTA 5HT2 LIBERAÇÃO RECAPTAÇÃO DOPAMINÉRGICO LIBERAÇÃO RECAPTAÇÃO NORADRENÉRGICO STAHL, 2000 Downing, 1986; Vollenweider,et al, 1998

84
Efeitos Imediatos com Dose Usual
ÊXTASE Efeitos Imediatos com Dose Usual POSITIVOS Felicidade / Bom humor Proximidade c/ outros Empatia sentidos autoconfiança Euforia Loquacidade Agitação “Aumento de energia” NEGATIVOS OU NEUTROS Diminuição do apetite Bruxismo / Trismo Náuseas e vômitos Taquicardia Hipertensão Insônia Sudorese Tremores Hepatotoxicidade

85
MACONHA Capa maconha

86
desenho esquemático de binding de THC – CB1
Receptores CB Regiões do SNC desenho esquemático de binding de THC – CB1 Cortex - Cognição e sentidos Hipocampo – Memória Cerebelo – Equilíbrio, coordenação motora Via do reforço Acumbens (Gânglios da base)
")
87
Síndrome de Abstinência
Reforço – Compulsão Tolerância Síndrome de Abstinência

88
Dependência: Principais características
1. Desejo ou compulsão 2. Dificuldade em controlar o consumo 3. Abandono de prazeres e interesses alternativos 4. Persistência no uso a despeito da evidência de conseqüências nocivas 5. Síndrome de Abstinência 6. Tolerância Organização Mundial de Saúde

89
REFORÇO – COMPULSÃO

90
Compulsão - Comportamento é reforçado (recompensa ou prazer)
Estado em que um organismo apresenta um comportamento impulsivo e repetitivo: - Comportamento é reforçado (recompensa ou prazer) - Perda do controle em limitar o consumo
 - Perda do controle em limitar o consumo.")
92
Slide 12: Activation of the reward pathway by an electrical stimulus
The discovery of the reward pathway was achieved with the help of animals such as rats. Rats were trained to press a lever for a tiny electrical jolt to certain parts of the brain. Show that when an electrode is placed in the nucleus accumbens, the rat keeps pressing the lever to receive the small electrical stimulus because it feels pleasurable. This rewarding feeling is also called positive reinforcement. Point to an area of the brain close to the nucleus accumbens. Tell the audience that when the electrode is placed there, the rat will not press the lever for the electrical stimulus because stimulating neurons in a nearby area that does not connect with the nucleus accumbens does not activate the reward pathway. The importance of the neurotransmitter dopamine has been determined in these experiments because scientists can measure an increased release of dopamine in the reward pathway after the rat receives the reward. And, if the dopamine release is prevented (either with a drug or by destroying the pathway), the rat won't press the bar for the electrical jolt. So with the help of the rats, scientists figured out the specific brain areas as well as the neurochemicals involved in the reward pathway.
, the rat won t press the bar for the electrical jolt. So with the help of the rats, scientists figured out the specific brain areas as well as the neurochemicals involved in the reward pathway.")
93
Slide 8: Reward: drug self-administration
Introduce the concept of positive reinforcement or reward. Explain that rats will press a bar to get an injection of cocaine or heroin (self-administration - shown on the left). The rat keeps pressing to get more cocaine or heroin because the drugs make the rat feel so good. This is called positive reinforcement, or reward. Natural rewards include food, water and sex - each is required to maintain survival of our species. Animals and people will continue to exhibit a behavior that is rewarding - and they will cease that behavior when the reward is no longer present. Explain that there is actually a part of the brain that is activated by natural rewards and by artificial rewards such as addictive drugs. This part of the brain is called the reward system. Neuroscientists have been able to pinpoint the exact parts of the brain involved, with the help of the rats. Point to the cartoon on the right and explain that rats will also self-administer addictive drugs directly into their brains -but only into a specific area of the reward system. If the injection needle is moved less than a millimeter away from this crucial area, the rat won't press the lever for more drug. So based on information from working with the rats, scientists have drawn a map of the brain, and located the structures and pathways that are activated when an addictive drug is taken voluntarily. Tell the students that you will show them this "map".
. The rat keeps pressing to get more cocaine or heroin because the drugs make the rat feel so good. This is called positive reinforcement, or reward. Natural rewards include food, water and sex - each is required to maintain survival of our species. Animals and people will continue to exhibit a behavior that is rewarding - and they will cease that behavior when the reward is no longer present. Explain that there is actually a part of the brain that is activated by natural rewards and by artificial rewards such as addictive drugs. This part of the brain is called the reward system. Neuroscientists have been able to pinpoint the exact parts of the brain involved, with the help of the rats. Point to the cartoon on the right and explain that rats will also self-administer addictive drugs directly into their brains -but only into a specific area of the reward system. If the injection needle is moved less than a millimeter away from this crucial area, the rat won t press the lever for more drug. So based on information from working with the rats, scientists have drawn a map of the brain, and located the structures and pathways that are activated when an addictive drug is taken voluntarily. Tell the students that you will show them this map .")
94
Slide 30: Summary; addictive drugs activate the reward system via increasing dopamine neurotransmission In this last slide, the reward pathway is shown along with several drugs that have addictive potential. Just as heroin (morphine) and cocaine activate the reward pathway in the VTA and nucleus accumbens, other drugs such as nicotine and alcohol activate this pathway as well, although sometimes indirectly (point to the globus pallidus, an area activated by alcohol that connects to the reward pathway). While each drug has a different mechanism of action, each drug increases the activity of the reward pathway by increasing dopamine transmission. Because of the way our brains are designed, and because these drugs activate this particular brain pathway for reward, they have the ability to be abused. Thus, addiction is truely a disease of the brain. As scientists learn more about this disease, they may help to find an effective treatment strategy for the recovering addict.
 and cocaine activate the reward pathway in the VTA and nucleus accumbens, other drugs such as nicotine and alcohol activate this pathway as well, although sometimes indirectly (point to the globus pallidus, an area activated by alcohol that connects to the reward pathway). While each drug has a different mechanism of action, each drug increases the activity of the reward pathway by increasing dopamine transmission. Because of the way our brains are designed, and because these drugs activate this particular brain pathway for reward, they have the ability to be abused. Thus, addiction is truely a disease of the brain. As scientists learn more about this disease, they may help to find an effective treatment strategy for the recovering addict.")
95
TOLERÂNCIA Necessidade de quantidades crescentes da substância para obter o mesmo efeito (ou quantidade habitual produz cada vez menos efeito) OMS, 2004

96
TOLERÂNCIA O organismo vai ficando menos sensível aos efeitos da substância: DOWNREGULATION DOS RECEPTORES NIDA

97
Ex.: cocaína e anfetaminas
TOLERÂNCIA CRUZADA quando o cérebro do usuário, uma vez já tolerante à droga, invoca o mesmo mecanismo adaptativo quando exposto à outras drogas que produzem efeitos psicoativos similares. Ex.: cocaína e anfetaminas álcool e anestésico Morfina e Heróina DESAFIO: Pq não ocorre tolerância cruzada entre, por exemplo, cocaína e benzodiazepínicos ???????

98
SINDROME DE ABSTINÊNCIA
Conjunto de sinais e sintomas que ocorrem quando o consumo da substância é reduzido ou interrompido OMS, 2004

99
Comunicação química entre neurônios
SINAPSE Retirada da droga Neurotransmissores Quantidade de receptores insuficiente para manter o sistema funcionando normalmente Receptores Down regulation STAHL, 2000

100
SÍNDROME DE ABSTINÊNCIA (OMS)
")
101
Bases Genéticas na vulnerabilidade às dependências

102
e, em parte, explicar a variação do consumo e da dependência”
Bases Genéticas “As heranças genéticas podem ser responsáveis por diferenças de ação das drogas entre os indivíduos e, em parte, explicar a variação do consumo e da dependência”

103
é um “Transtorno Complexo”
Bases Genéticas Dependência é um “Transtorno Complexo” ou seja, provavelmente causado pela interação de vários genes com vários fatores ambientais.

104
Bases Genéticas substâncias psicoativas podem ter um efeito maior em pessoas com vulnerabilidade genética a dependência. CUIDADO! Para não confundir com determinismo biológico (ex:cor dos olhos)
")
105
Bases Genéticas Tipos de estudos:
- Estudos de padrões transgeracionais (famílias) em gêmeos monozigóticos x dizigóticos e indivíduos adotados. - Estudo de “traços” relacionados - Busca de genes possivelmente relacionados (como genes de receptores, genes de enzimas, etc)
 em gêmeos monozigóticos x dizigóticos e indivíduos adotados. - Estudo de traços relacionados. - Busca de genes possivelmente relacionados (como genes de receptores, genes de enzimas, etc)")
106
Genética e a dependência do álcool
- Diferenças nas características dos receptores gabaérgicos, serotonérgicos e dopaminérgicos - Diferenças no metabolismo: ex. deficiência da enzima aldeído desidrogenase (ADH)
")
107
Dependência do álcool deficiência enzimática ADH, especialmente em orientais
Álcool desidrogenase Aldeído desidrogenase X ACETALDEÍDO ACETATO ETANOL (Álcool Etílico) Reações: “vermelhão” no rosto, náuseas, mal estar, etc.
 Reações: vermelhão no rosto, náuseas, mal estar, etc.")
108
Dependência do Tabaco Vários genes implicados:
Ex: Metabolismo da nicotina (acúmulo de nicotina no cérebro), receptores, etc Diferenças de hereditariedade entre populações, gênero.
, receptores, etc. Diferenças de hereditariedade entre populações, gênero.")
109
Perspectivas da genética
Os resultados até então encontrados, embora incompletos, indicam perspectivas promissoras. Uma vez identificados os genes, o desafio será compreender a interação com o ambiente: para novos diagnósticos e tratamentos.

110
COMORBIDADE

111
Transtornos associados
COMORBIDADE Transtornos associados Ocorrência conjunta de dois ou mais transtornos mentais ou condições médicas gerais.

112
Tratamento Farmacológico ÁLCOOL Dissulfiram (Anti-álcool)
Álcool desidrogenase Aldeído desidrogenase X ACETALDEÍDO ACETATO ETANOL (Álcool Etílico) Reações: “vermelhão” no rosto, náuseas, mal estar, etc. REAÇÃO AVERSIVA
 Reações: vermelhão no rosto, náuseas, mal estar, etc. REAÇÃO AVERSIVA.")
113
Tratamento Farmacológico ÁLCOOL
Acamprosato Substância sintética semelhante a um aminoácido natural. Restabelece atividade de neurônios que ficaram super excitados devido à exposição crônica ao álcool

114
Tratamento Farmacológico ÁLCOOL Naltrexona
Substância que bloqueia os receptores opióides

115
Tratamento Farmacológico TABACO Adesivos transdérmicos
Substituição da nicotina com retirada gradativa

116
Tratamento Farmacológico TABACO Bupropiona
Inibidor fraco da recaptura de noradrenalina e dopamina

117
Tratamento Farmacológico HEROíNA Metadona
Substituição da heroína por metadona com posterior retirada gradativa

Apresentações semelhantes