Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Rafaella Elíria Abbott
IMAGING IN EPILEPSY: a paediatric perspective Review article The British Journal of radiology, July 2001 Rafaella Elíria Abbott

2
Objetivos do artigo: Os avanços radiológicos são importantes, porém a avaliação mais importante na epilepsia é a história clínica! Lembrar que imagem não é necessária em todas as crianças com epilepsia, mas desempenha um papel fundamental em alguns casos ; Discutir e definir os casos necessários; Discutir um pouco dos exames de imagem na epilepsia da infância.

3
Diagnóstico de epilepsia
4 pontos Reconhecer a crise convulsiva Classificar a crise convulsiva Identificar uma síndrome epiléptica Identificar etiologia secundária

4
Table 1. Classification of seizures
Partial seizures (seizures beginning locally) Simple (consciousness not impaired) + motor symptoms + somatosensory or special sensory symptoms + autonomic symptoms + psychic symptoms Complex (consciousness lost) Beginning as simple partial seizure, progressing to complex seizure Consciousness lost at onset loss of consciousness only with automatism Partial seizures becoming secondarily generalized Generalized seizures Absence seizures Typical (petit mal) Atypical Myoclonic Clonic Tonic Tonic–clonic Atonic
 Simple (consciousness not impaired) + motor symptoms. + somatosensory or special sensory symptoms. + autonomic symptoms. + psychic symptoms. Complex (consciousness lost) Beginning as simple partial seizure, progressing to complex seizure. Consciousness lost at onset. loss of consciousness only. with automatism. Partial seizures becoming secondarily generalized. Generalized seizures. Absence seizures. Typical (petit mal) Atypical. Myoclonic. Clonic. Tonic. Tonic–clonic. Atonic.")
5
Epilepsia x Crise x Síndromes epilépticas
Epilepsia: distúrbio do SNC, caracterizado por crises sucessivas,sem outras causas sistêmicas ou neurológicas. Crise: Manifestação clínica de uma descarga anormal excessiva e hipersincrônica de neurônios corticais. Síndrome: forma particular de epilepsia, que apresenta causa,clínica e prognóstico específicos. As síndromes podem apresentar mais de um tipo de crise.

6
Table 2. A glossary of eponymous paediatric epilepsy syndromes
West’s syndrome Uncommon. Infantile spasms, hypsarrythmia on electroencephalogram (EEG) and arrested psychomotor development. Age of onset 3–12 months. 70–80% are associated with conditions such as tuberous sclerosis, hypoxic–ischaemic change, infection and metabolic abnormalities. Prognosis generally poor. Landau–Kleffner syndrome Rare. Acquired epileptic aphasia. Generalized and focal seizures usually preceded by receptive and expressive language disorder. Developmental regression. Age of onset 2–10 years. Prognosis is good for seizure control but poor for language recovery. Lennox–Gastaut syndrome Uncommon. Most common intractable childhood epilepsy. Tonic and atypical absences with ‘‘drop’’ attacks. Age of onset peaks at 3–5 years. One in five have preceding West’s syndrome. Prognosis poor with persistent developmental abnormalities. Ohtahara’s syndrome Rare. Early infantile epileptic encephalopathy. Brief tonic seizures, EEG showing burst suppression. Age of onset first few months of life. Brain malformations are common. Prognosis poor. Kojewnikov’s syndrome Rare. Chronic progressive epilepsia partialis continua of childhood. Frequent continuous, partial motor seizures. Age of onset up to 10 years. Associated with subacute encephalitis (Rasmussen’s) and mitochondrial encephalomyopathies. Prognosis poor, with hemiplegia and dysphasia.
 and arrested psychomotor development. Age of onset 3–12 months. 70–80% are associated with conditions such as tuberous sclerosis, hypoxic–ischaemic change, infection and metabolic abnormalities. Prognosis generally poor. Landau–Kleffner syndrome. Rare. Acquired epileptic aphasia. Generalized and focal seizures usually preceded by receptive and expressive language disorder. Developmental regression. Age of onset 2–10 years. Prognosis is good for seizure control but poor for language recovery. Lennox–Gastaut syndrome. Uncommon. Most common intractable childhood epilepsy. Tonic and atypical absences with ‘‘drop’’ attacks. Age of onset peaks at 3–5 years. One in five have preceding West’s syndrome. Prognosis poor with persistent developmental abnormalities. Ohtahara’s syndrome. Rare. Early infantile epileptic encephalopathy. Brief tonic seizures, EEG showing burst suppression. Age of onset first few months of life. Brain malformations are common. Prognosis poor. Kojewnikov’s syndrome. Rare. Chronic progressive epilepsia partialis continua of childhood. Frequent continuous, partial motor seizures. Age of onset up to 10 years. Associated with subacute encephalitis (Rasmussen’s) and mitochondrial encephalomyopathies. Prognosis poor, with hemiplegia and dysphasia.")
7
Guidelines para indicações de imagem em epilepsia

8
Table 3. Guidelines for specific seizure types and epilepsy syndromes
A. Not every child with epilepsy needs brain imaging (CT or MRI) B. The following groups of patients do not require brain imaging: 1. children with primary (idiopathic) generalized epilepsy: typical absence epilepsy (‘‘petit mal’’) juvenile myoclonic epilepsy epilepsy with ‘‘grand mal’’ on awakening 2. children with benign partial epilepsy with either centrotemporal or occipital spikes 3. children with simple febrile convulsions 4. a persistent focal discharge (spike, sharp or slow wave) on a single electroencephalogram does not in itself justify a brain scan C. The following groups of children with epilepsy require brain imaging: 1. children with a focal neurological deficit or asymmetry 2. children with evidence of a neurocutaneous syndrome, such as tuberous sclerosis or neurofibromatosis 3. children with evidence of developmental regression 4. children with simple partial seizures 5. children with refractory complex partial seizures (refractory implies at least one seizure per month) not responding to anti-epileptic treatment 6. children with infantile spasms or myoclonic seizures presenting in the first year of life 7. children with persisting unclassifiable seizures
 B. The following groups of patients do not require brain imaging: 1. children with primary (idiopathic) generalized epilepsy: typical absence epilepsy (‘‘petit mal’’) juvenile myoclonic epilepsy. epilepsy with ‘‘grand mal’’ on awakening. 2. children with benign partial epilepsy with either centrotemporal or occipital spikes. 3. children with simple febrile convulsions. 4. a persistent focal discharge (spike, sharp or slow wave) on a single electroencephalogram does not in itself. justify a brain scan. C. The following groups of children with epilepsy require brain imaging: 1. children with a focal neurological deficit or asymmetry. 2. children with evidence of a neurocutaneous syndrome, such as tuberous sclerosis or neurofibromatosis. 3. children with evidence of developmental regression. 4. children with simple partial seizures. 5. children with refractory complex partial seizures (refractory implies at least one seizure per month) not. responding to anti-epileptic treatment. 6. children with infantile spasms or myoclonic seizures presenting in the first year of life. 7. children with persisting unclassifiable seizures.")
9
LOBO TEMPORAL Área de maior interesse para os radiologistas em crianças com epilepsia. ELT- Epilepsia di Lobo Temporal corresponde a 40% de todos os casos deepilepsia na população, e foi dividida em ELTM (epilepsia do lobo temporal mesial) e ELTN (epilepsia do lobo temporal neocortical ou lateral) ELTM = 60% dos casos de ELT ELTM apresentar também alto índice de casos de epilepsia refratárias aos medicamentos.
 e ELTN (epilepsia do lobo temporal neocortical ou lateral) ELTM = 60% dos casos de ELT. ELTM apresentar também alto índice de casos de epilepsia refratárias aos medicamentos.")
10
Características na RM incluem atrofia hipocampal em T2
Esclerose mesial temporal, também conhecida como esclerose hipocampal é a anomalia estrutural focal mais comumente diagnosticada em pacientes com epilepsia. A maioria dos casos estão presentes na infância, porém não é raro que este transtorno também apareça pela primeira vez em adultos jovens. O tipo de crise típica é sensitiva com automatismos; a generalização secundária é rara. Características na RM incluem atrofia hipocampal em T2 hiperintensidade de sinal FLAIR

11
MR image of the temporal lobe showing atrophy and increased T2 signal in the left hippocampus, consistent with mesial temporal sclerosis.

12
Coronal T1 weighted gradient echo MR volume acquisition showing bilateral areas of cortical dysplasia (arrowheads).
.")
13
da substância cinzenta
Relaxometria em T2 Avaliação da substância cinzenta hipocampal. T2 maps of the temporal lobes showing the sampling area, and histograms of the T2 times with derived average values. The left temporal lobe shows an increased T2 time (123 ms), consistent with mesial sclerosis.
, consistent with mesial. sclerosis.")
14
Exames: TC crânio RM de crânio RM Funcional
PET (TC emissão de positron) SPECT (Emissão de Fóton Único) Angiografia cerebral
 SPECT (Emissão de Fóton Único) Angiografia cerebral.")
15
TC CRÂNIO Menos utilizado atualmente, mas ainda muito utilizado na suspeita de calcificação cerebral.

16
CT of a child with tuberous sclerosis showing periventricular calcification and low attenuation parenchymal tubers. CT remains the imaging modality of choice for identifying focal calcification.

17
Exame atualmente de escolha.
RM CRÂNIO Exame atualmente de escolha.

18
Patologias específicas- Estruturas de causas de epilepsia que possam ser identificadas pela RM:
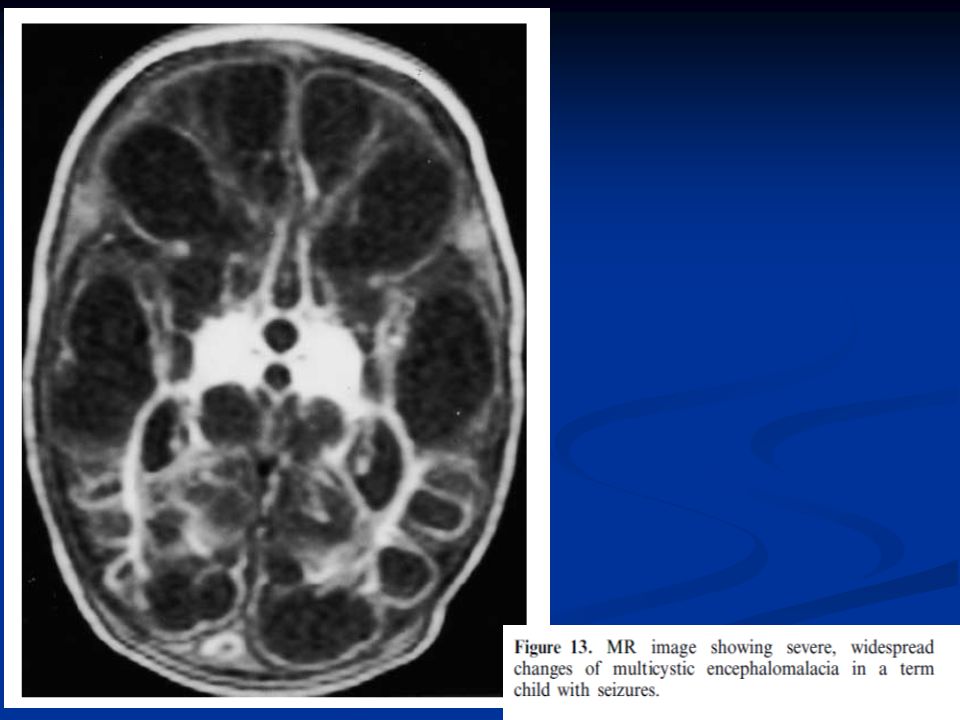
Esclerose mesial temporal (esclerose hipocampal); Malformações do desenvolvimento cortical (por exemplo, a displasia cortical); Tumores cerebrais; Malformações vasculares; Infarto cerebral, hemorragia cerebral; Lesão cerebral traumática ; Infecções, incluindo a encefalite, abscesso cerebral, granulomas e cistos (neurocisticercose);
; Malformações do desenvolvimento cortical (por exemplo, a displasia cortical); Tumores cerebrais; Malformações vasculares; Infarto cerebral, hemorragia cerebral; Lesão cerebral traumática ; Infecções, incluindo a encefalite, abscesso cerebral, granulomas e cistos (neurocisticercose);")
19
RESSONÂNCIA MAGNÉTICA FUNCIONAL
A RMf pode detectar alterações focais no fluxo do sangue e os níveis de oxigenação, que ocorrem quando uma área do cérebro é ativada. RMf não-invasiva, avaliação motora, sensorial e funções da linguagem, e é mais comumente usada como parte do planejamento cirúrgico ,para prever o limite de déficit neurológico pós-operatório, particularmente a função da linguagem .

20
SPECT Em uma tomografia por emissão de fóton único (SPECT) 99mTc
SPECT fornece um instantâneo estudo da circulação cerebral, no momento da injeção. O marcador é estável por várias horas, permitindo que a imagem latente fluxo seja observada. Em pacientes com epilepsia focal, o SPECT demonstra hiperperfusão no período ictal hipoperfusão pós-ictal hipoperfusão interictal SPECT podendo ser útil na identificação de um possível foco epiléptico, particularmente quando a RM é normal, SPECT apresenta lata sensibilidade para avaliação da epilepsia do lobo temporal (>90%), mas a sensibilidade para os focos de crise extratemporal é menor .
, mas a sensibilidade para os focos de crise extratemporal é menor .")
21
An ictal SPECT scan showing hyperperfusion at a likely seizure focus in the left temporal region

22
99Tcm-labelled hexamethyl propyleneamine oxime SPECT interictal brain images. The top two rows show a normal dataset, the bottom two rows show a number of focal defects, especially in the right frontal region.

23
PET Imagem do metabolismo cerebral.
No período Ictal os exames podem ser úteis, mas são difíceis de obter, exceto em casos raros, tais como epilepsia parcial contínua. Áreas com hipometabolismo refletem distúrbios focais funcionais da atividade cerebral associada com o tecido epileptogênico. Geralmente é realizado pré-operatório.

24
IMAGENS

25
MR inversion recovery sequence demonstrating
a subtle focal area of polymicrogyria/cortical dysplasia (arrowheads).
.")
26
(b) (a) Figure 7. (a,b) Three-dimensional cortical rendering from a volume acquisition clearly showing bilateral symmetrical pachygyria of the frontal lobes.
 Three-dimensional cortical rendering from a volume acquisition clearly showing bilateral symmetrical pachygyria of the frontal lobes.")
27
Coronal T1 weighted MR image through the pituitary region showing the hypothalamic hamartoma responsible for the child’s gelastic seizures (arrow).
.")
28
MR image showing the pial–ependymal seam of grey matter typical of schizencephaly in the right frontal lobe.

29
Cerebral spinal fluid suppression (fluid attenuated inversion recovery (FLAIR).
MR image of the brain of a child with tuberous sclerosis showing multiple cortical tubers and subependymal nodules and a calcified focus in the right occipital lobe. Note the generalized increase in signal intensity of the right cerebral hemisphere related to a recent period of status epilepticus.

30
(a) (b) Figure 11. (a) CT in the early stages of herpes encephalitis showing reduced attenuation in the right temporal lobe. (b) MR image showing bilateral changes involving the temporal lobes and right cingulate gyrus.
 CT in the early stages of herpes encephalitis showing reduced attenuation in the right temporal lobe. (b) MR image showing bilateral changes involving the temporal lobes and right cingulate gyrus.")
31
MR image showing unusual, predominantly
unilateral changes secondary to toxoplasmosis infection. Note the right orbital abnormality

35
Pontos-chave Imagem não deve ser solicitada para todas as crianças;
ELTM tem alto índice e muitos casos de intratabilidade medicamentosa; RM é o exame de escolha; SPECT e PET podem ser úteis nos casos em que aRM não apresenta anormalidade.

36
Referências: Imaging in epilepsy: a paediatric perspective – Review article – The British Journal of Radiology – Julho/2001 Neuroimaging in the evaluation of seizures and epilepsy – Up to date – Out/2009

Apresentações semelhantes