Carregar apresentação
A apresentação está carregando. Por favor, espere

1
"Proximidades entre Nefrologia e Cirurgia Vascular“ LAVUEL – 2010
Waldir E. Garcia Professor Associado da Disciplina de Nefrologia do Departamento de Clínica Médica/UEL

2
Nefrologia Cirurgia vascular
IRA/IRC Agudizada: - IAPC - aterosclerose/arterioesclerose - diabetes mellitus nefropatia isquêmica - nefropatia do contraste - rabdomiólise - ateroembolismo Hipertensão reno-vascular nefropatia isquêmica Via de acesso para hemodiálise: FAV (confecção e tratamento das complicações) - Transplante renal
 - Transplante renal.")
3
IRA, IRC Agudizada Quando devemos pensar neste diagnóstico ? ≠ retenção de produtos normalmente excretados pelos rins ( ↑ uréia e creatinina com ↓ na TFG – fórmulas!) - redução do volume urinário (RIFLE/AKIN)
 - redução do volume urinário (RIFLE/AKIN)")
4
Porque o risco de IRA ou de IRC Agudizada
está aumentado nos pacientes com IAPC?

6
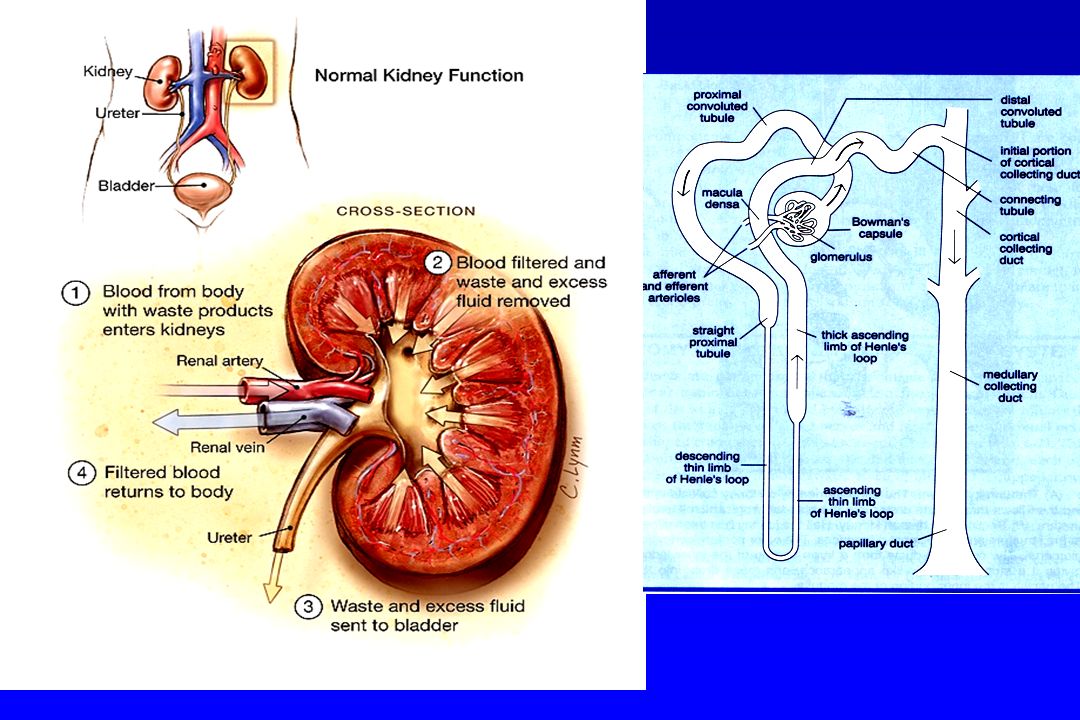
Hemodinâmica Renal: função glomerular...
Débito Cardíaco: ml/min Fluxo Sanguíneo Renal: 1200 ml/min Fluxo Plasmático Renal: 600 ml/min 4) Fração de Filtração (TFG/FPR) = 20% TFG 120 ml/min Formação do Ultrafiltrado – funções tubulares... 100 ml x 1440 min = ml/dia ou 28 x o Débito Cardíaco
 Fração de Filtração (TFG/FPR) = 20% TFG 120 ml/min. Formação do Ultrafiltrado – funções tubulares ml x 1440 min = ml/dia. ou 28 x o Débito Cardíaco.")
8
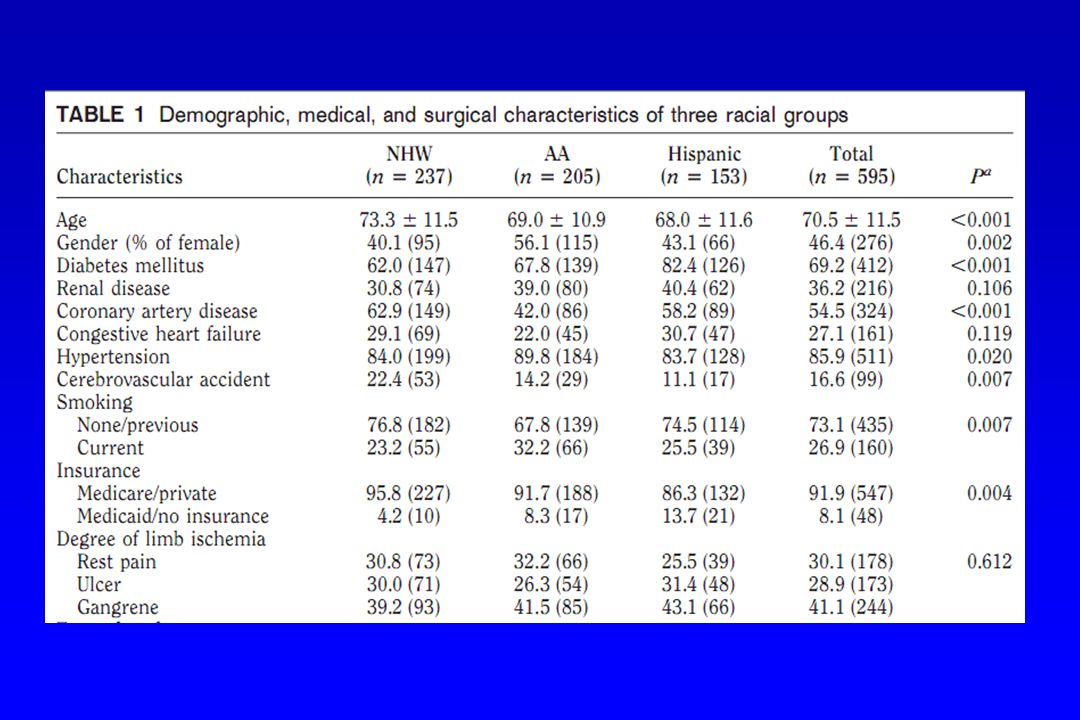
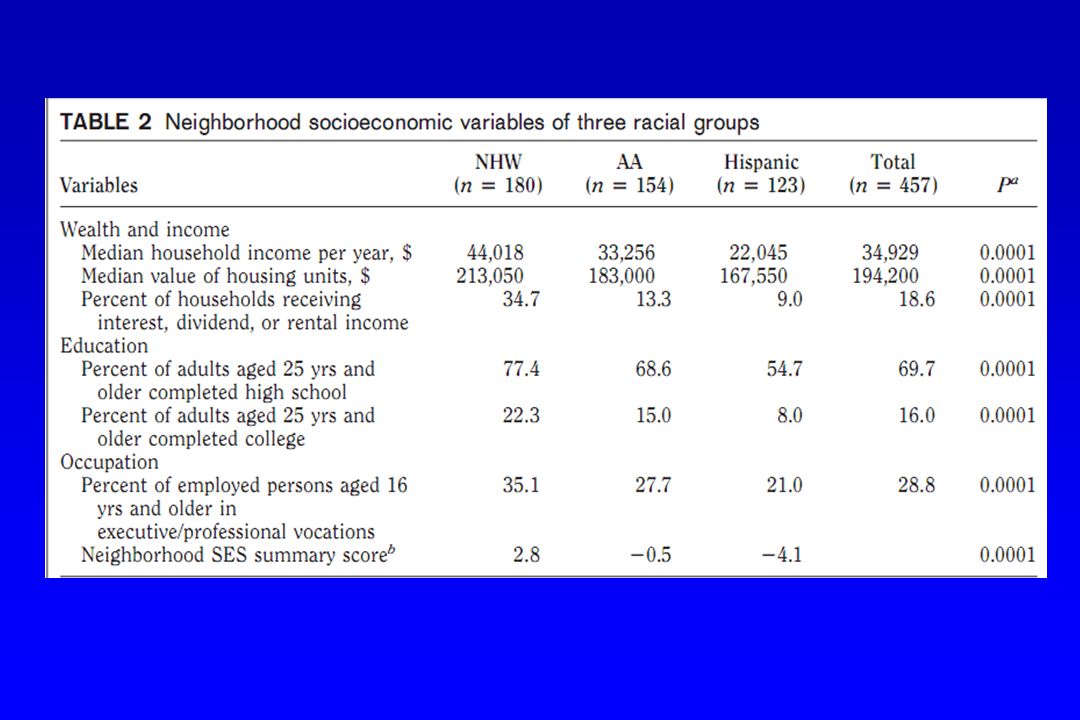
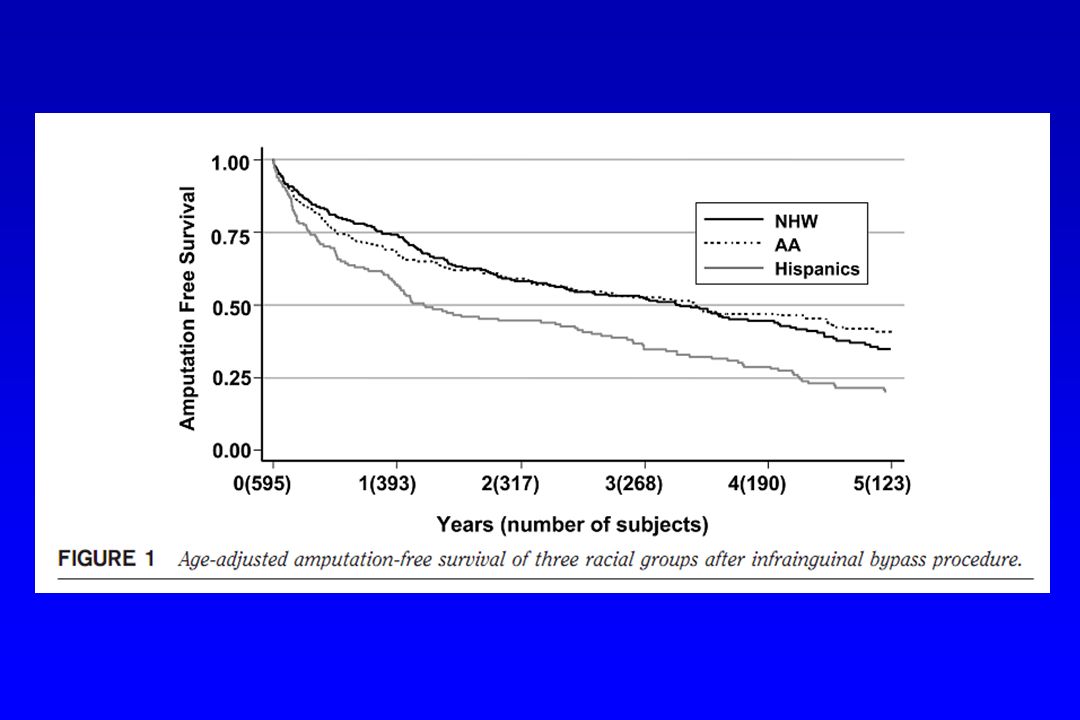
amputação sobrevida

13
Normal and Impaired Autoregulation of the Glomerular Filtration Rate during Reduction of Mean Arterial Pressure Figure 1. Normal and Impaired Autoregulation of the Glomerular Filtration Rate during Reduction of Mean Arterial Pressure. In normal autoregulation, the glomerular filtration rate (GFR) is maintained until the mean arterial pressure falls below 80 mm Hg. However, in patients with impaired autoregulation, the GFR falls below normal values while the mean arterial pressure remains within the normal range, resulting in normotensive ischemic acute renal failure. Abuelo J. N Engl J Med 2007;357:
 is maintained until the mean arterial pressure falls below 80 mm Hg. However, in patients with impaired autoregulation, the GFR falls below normal values while the mean arterial pressure remains within the normal range, resulting in normotensive ischemic acute renal failure. Abuelo J. N Engl J Med 2007;357:")
14
Intrarenal Mechanisms for Autoregulation of the Glomerular Filtration Rate under Decreased Perfusion Pressure and Reduction of the Glomerular Filtration Rate by Drugs Figure 2. Intrarenal Mechanisms for Autoregulation of the Glomerular Filtration Rate under Decreased Perfusion Pressure and Reduction of the Glomerular Filtration Rate by Drugs. Panel A shows normal conditions and a normal glomerular filtration rate (GFR). Panel B shows reduced perfusion pressure within the autoregulatory range. Normal glomerular capillary pressure is maintained by afferent vasodilatation and efferent vasoconstriction. Panel C shows reduced perfusion pressure with a nonsteroidal antiinflammatory drug (NSAID). Loss of vasodilatory prostaglandins increases afferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Panel D shows reduced perfusion pressure with an angiotensin-converting-enzyme inhibitor (ACEI) or an angiotensin-receptor blocker (ARB). Loss of angiotensin II action reduces efferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Abuelo J. N Engl J Med 2007;357:
. Panel B shows reduced perfusion pressure within the autoregulatory range. Normal glomerular capillary pressure is maintained by afferent vasodilatation and efferent vasoconstriction. Panel C shows reduced perfusion pressure with a nonsteroidal antiinflammatory drug (NSAID). Loss of vasodilatory prostaglandins increases afferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Panel D shows reduced perfusion pressure with an angiotensin-converting-enzyme inhibitor (ACEI) or an angiotensin-receptor blocker (ARB). Loss of angiotensin II action reduces efferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Abuelo J. N Engl J Med 2007;357:")
15
Figure 2. Intrarenal Mechanisms for Autoregulation of the Glomerular Filtration Rate under Decreased Perfusion Pressure and Reduction of the Glomerular Filtration Rate by Drugs. Panel A shows normal conditions and a normal glomerular filtration rate (GFR). Panel B shows reduced perfusion pressure within the autoregulatory range. Normal glomerular capillary pressure is maintained by afferent vasodilatation and efferent vasoconstriction. Panel C shows reduced perfusion pressure with a nonsteroidal antiinflammatory drug (NSAID). Loss of vasodilatory prostaglandins increases afferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Panel D shows reduced perfusion pressure with an angiotensin-converting-enzyme inhibitor (ACEI) or an angiotensin-receptor blocker (ARB). Loss of angiotensin II action reduces efferent resistance; this causes the glomerular capillary pressure to drop below normal values and the GFR to decrease. Abuelo J. N Engl J Med 2007;357:

16
Como avaliar a “função renal”
(taxa de filtração glomerular) ?
")
17
Estimativa da TFG através da Creatinina sérica Equação de Gault - Cocrkoft
TFG = (140 - idade) x Peso (Kg) x 1,73 ml/min/1,73 m2 72 x creatinina no sangue SC * x 0,85 para mulheres ** corrigir para a SC, especialmente na IRC e idosos (COCRKCROFT, D.W.; GAULT, M.H. – Nephron 16: 31-41, 1976)
 x Peso (Kg) x 1,73 ml/min/1,73 m2. 72 x creatinina no sangue SC. * x 0,85 para mulheres. ** corrigir para a SC, especialmente na IRC e idosos. (COCRKCROFT, D.W.; GAULT, M.H. – Nephron 16: 31-41, 1976)")
18
Diagnóstico da IRA / IRC Agudizada !

19
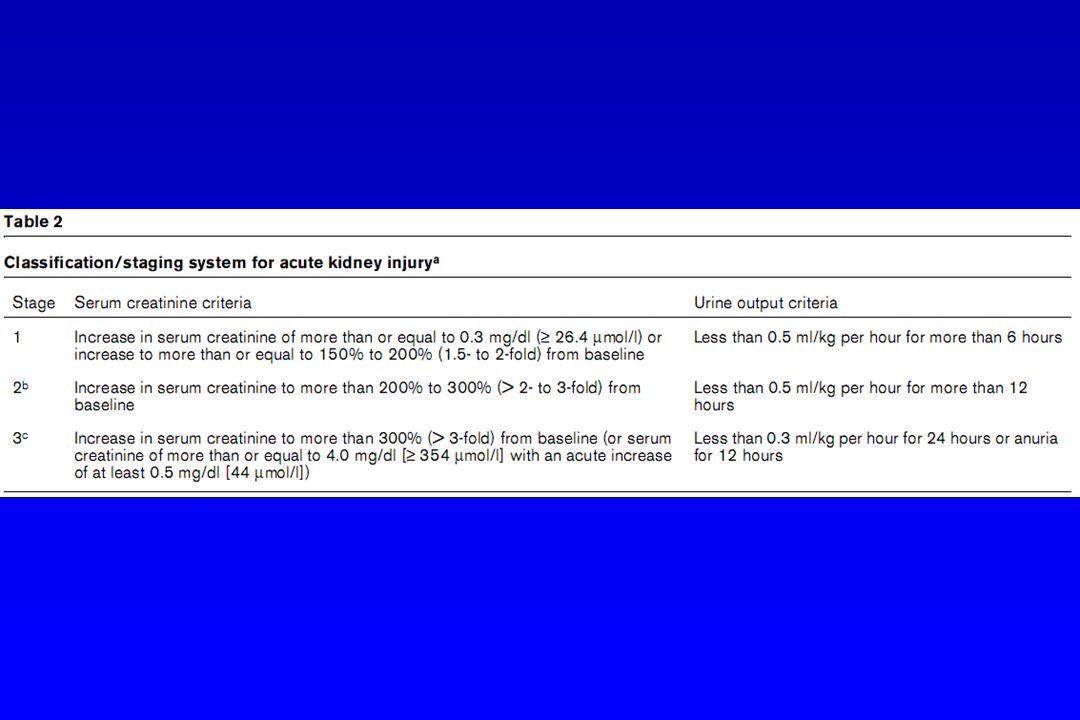
(ADQI – Belomo, R et al. Critical Care 8: R204 – R212, 2004)
")
20
(ADQI – Belomo, R et al. Critical Care 8: R204 – R212, 2004)
")
23
Stages of Chronic Kidney Disease (CKD), Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management Table 1. Stages of Chronic Kidney Disease (CKD), Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management. Stevens L et al. N Engl J Med 2006;354:
, Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management. Stevens L et al. N Engl J Med 2006;354:")
24
MANEJO DA IRA: TRATAMENTO CONSERVADOR :
1) CORREÇÃO DA DEPLEÇÃO DO VEC 2) PRESCRIÇÃO ADEQUADA – SUPORTE NUTRICIONAL 3) SUBSTITUIÇÃO OU CORREÇÃO DE DOSES DOS MEDICAMENTOS NEFROTÓXICOS 4) DIURÉTICOS 5) DOPAMINA 6) TERAPIA ANTIOXIDANTE / N-ACETIL CISTEÍNA 7) FATOR ATRIAL NATRIURÉTICO
 CORREÇÃO DA DEPLEÇÃO DO VEC. 2) PRESCRIÇÃO ADEQUADA – SUPORTE NUTRICIONAL. 3) SUBSTITUIÇÃO OU CORREÇÃO DE DOSES DOS. MEDICAMENTOS NEFROTÓXICOS. 4) DIURÉTICOS. 5) DOPAMINA. 6) TERAPIA ANTIOXIDANTE / N-ACETIL CISTEÍNA. 7) FATOR ATRIAL NATRIURÉTICO.")
25
Ajustar as drogas para o nível de Função Renal

26
* ou ANÚRIA !

27
Quando chamar a Nefro com urgência...
INDICATIONS FOR AND OPTIMAL TIMING OF DIALYSIS INITIATION : Refractory fluid overload Hyperkalemia (plasma potassium concentration >6.5 meq/L) or rapidly rising potassium levels Signs of uremia, such as pericarditis, neuropathy, or an otherwise unexplained decline in mental status Metabolic acidosis (pH less than 7.1) Uptodate * níveis ↑ de uréia e creatinina (→TFG < 10 ml/min)
 or rapidly rising potassium levels. Signs of uremia, such as pericarditis, neuropathy, or an otherwise unexplained decline in mental status. Metabolic acidosis (pH less than 7.1) Uptodate. * níveis ↑ de uréia e creatinina (→TFG < 10 ml/min)")
28
Kidney Atlas: Kierdorf, H
Kidney Atlas: Kierdorf, H.; Sieberth, HG – Nephrol Dial Transplant 1995; 10:2001-8

29
MANEJO DA IRA/IRC Agudizada: MEDIDAS PREVENTIVAS
RECONHECIMENTO DOS : 1) PACIENTES DE RISCO - DOENÇA RENAL PRÉVIA, IDADE AVANÇADA, DM, HA, IAPC MIELOMA MÚLTIPLO 2) FATORES E PROCEDIMENTOS DE RISCO – ** MEDICAMENTOS: IECA, AINH (hemodinâmica renal + nefrotoxicidade) ** EXAMES RADIOLÓGICOS CONTRASTADOS GRANDES CIRURGIAS (abdominais e cardiovasculares) ICTERÍCIA
 PACIENTES DE RISCO - DOENÇA RENAL PRÉVIA, IDADE AVANÇADA, DM, HA, IAPC. MIELOMA MÚLTIPLO. 2) FATORES E PROCEDIMENTOS DE RISCO – ** MEDICAMENTOS: IECA, AINH (hemodinâmica renal + nefrotoxicidade) ** EXAMES RADIOLÓGICOS CONTRASTADOS. GRANDES CIRURGIAS (abdominais e cardiovasculares) ICTERÍCIA.")
30
(SOLOMON, R.; et al - NEJM 331: 1416-1420, 1994)
")
31
83 pacientes com IRC (creatinina 2,4 1,3 mg/dl) foram para
TC contrastada, com contraste não-iônico de osmolaridade. - Receberam : N-ACETIL CISTEÍNA 600 mg, 2 x dia, VO ou placebo e SF 0,45% , 12 h. antes e após o contraste radiológico. -Resultados : 10 em 83 pacientes (12%) desenvolveram IRA ( creatinina de pelo menos 0,5 mg/dl em 48 hs.), sendo : 1 em 41 pacientes no grupo N-Acetil Cisteína (2%) X 9 em 42 pacientes no grupo controle (21% - p 0,01) (TEPEL, M.; et al. - NEJM 343(3): , 2000)
 desenvolveram IRA. ( creatinina de pelo menos 0,5 mg/dl em 48 hs.), sendo : 1 em 41 pacientes no grupo N-Acetil Cisteína (2%) X. 9 em 42 pacientes no grupo controle (21% - p 0,01) (TEPEL, M.; et al. - NEJM 343(3): , 2000)")
32
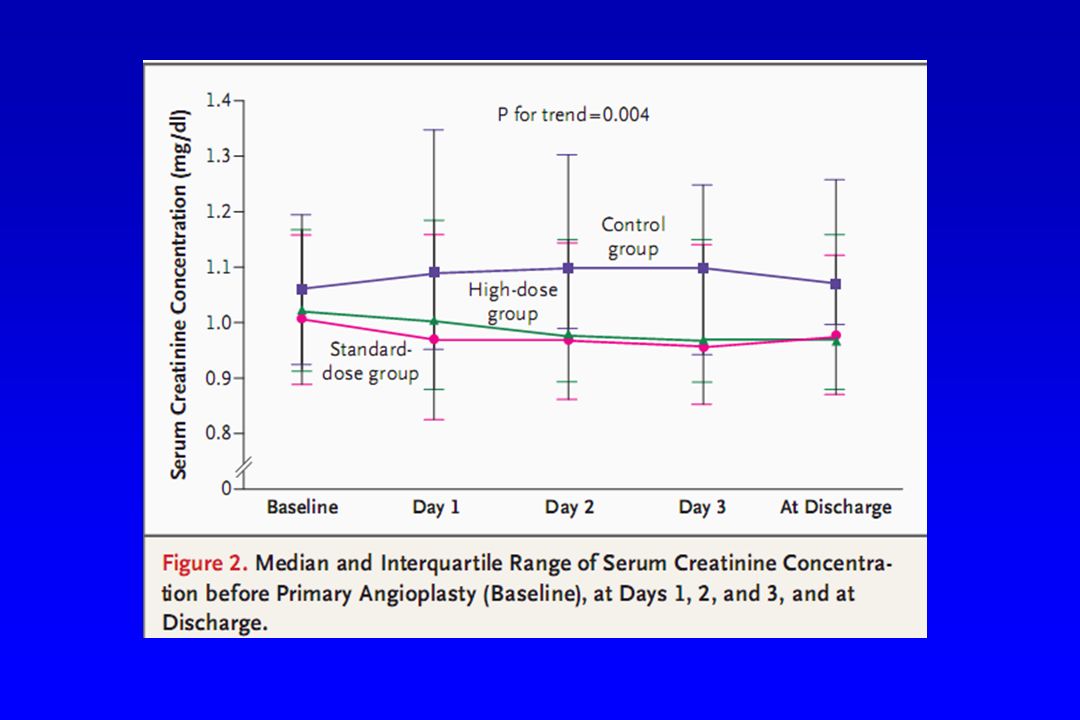
Serum Creatinine Concentrations Before and After Contrast
Merten, G. J. et al. JAMA 2004;291: Copyright restrictions may apply.

38
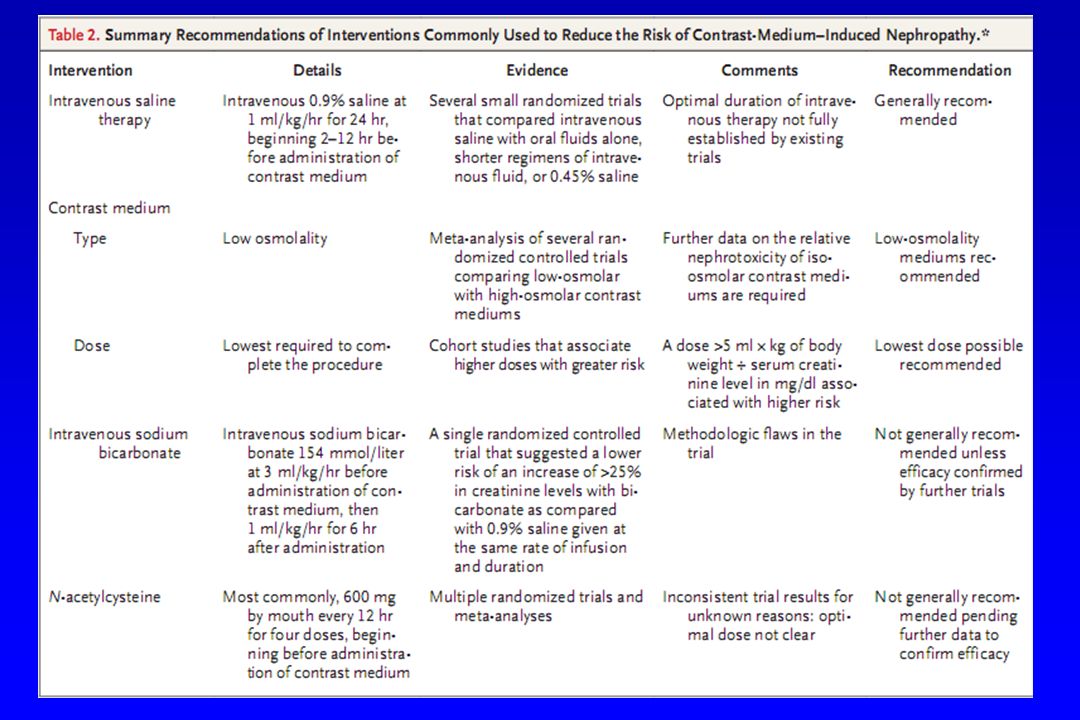
Conduta prática para manter VEC expandido antes de
procedimentos endovasculares com uso de contraste: SG 5% ml Bicarbonato de sódio a 8,4 % ml correr em BIC 3 ml/kg peso em 1 hora antes do exame e 1 ml/Kg peso/hora por mais 6 horas 3) Acetilcisteína 600 a 1200 mg 12/12 h. na véspera e no dia do exame (VO ou EV)
 Acetilcisteína 600 a 1200 mg 12/12 h. na véspera e no. dia do exame (VO ou EV)")
39
Table 1. Stages of Chronic Kidney Disease (CKD), Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management.
, Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management..")
40
Table 1. Stages of Chronic Kidney Disease (CKD), Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management.
, Prevalence in the United States in 2000, and Stage-Specific Recommendations for Detection, Evaluation, and Management..")
42
Tabela 3 adaptada: 1 – Verificar VEC, PVC e volume urinário
2 – Medir CPK 3 – Avaliar ureia e creatinina séricas e eletrólitos urinário, verificar tb.: calcio, fósforo, sódio, potássio, magnésio, gasometria, albumina e ácido úrico hemograma e coagulograma 4 – Urina tipo I (bioquímica e sedimento) 5 - Reposição de SF 0,9% 400 ml/hora ( ou mais, S/N) 6 – Volume urinário desejado: 3 ml/kg/hora, cerca de 200 ml/hora 7 – Acompanhar K sérico com frequência 8 – Corrigir Ca↓ apenas se sintomática ou se K↑↑ 9 – Investigar causas de rabdomiólise 10 – Verificar pH Urinário. Repor NaHCO3 se pH<6,5 (solução com 150 mEq/L) 11 – Considerar uso de Manitol (até 200 g/dia, dose total 800 g); checar osmolaridade e gap osmolar, suspender se diurese < 20 ml/hora 12 – Manter oferta alta de volume até urina clarear e “dipstick” normal para “Hb” 13 – Indicações de diálise: hipercalemia refratária ou de ascenção rápida, oligúria (< 0,5 ml/Kg/hora) ou anúria, sobrecarga de volume ou acidose grave (pH< 7,1)
 5 - Reposição de SF 0,9% 400 ml/hora ( ou mais, S/N) 6 – Volume urinário desejado: 3 ml/kg/hora, cerca de 200 ml/hora. 7 – Acompanhar K sérico com frequência. 8 – Corrigir Ca↓ apenas se sintomática ou se K↑↑ 9 – Investigar causas de rabdomiólise. 10 – Verificar pH Urinário. Repor NaHCO3 se pH<6,5 (solução com 150 mEq/L) 11 – Considerar uso de Manitol (até 200 g/dia, dose total 800 g); checar osmolaridade e gap osmolar, suspender se diurese < 20 ml/hora. 12 – Manter oferta alta de volume até urina clarear e dipstick normal para Hb 13 – Indicações de diálise: hipercalemia refratária ou de ascenção rápida, oligúria. (< 0,5 ml/Kg/hora) ou anúria, sobrecarga de volume ou acidose grave (pH< 7,1)")
43
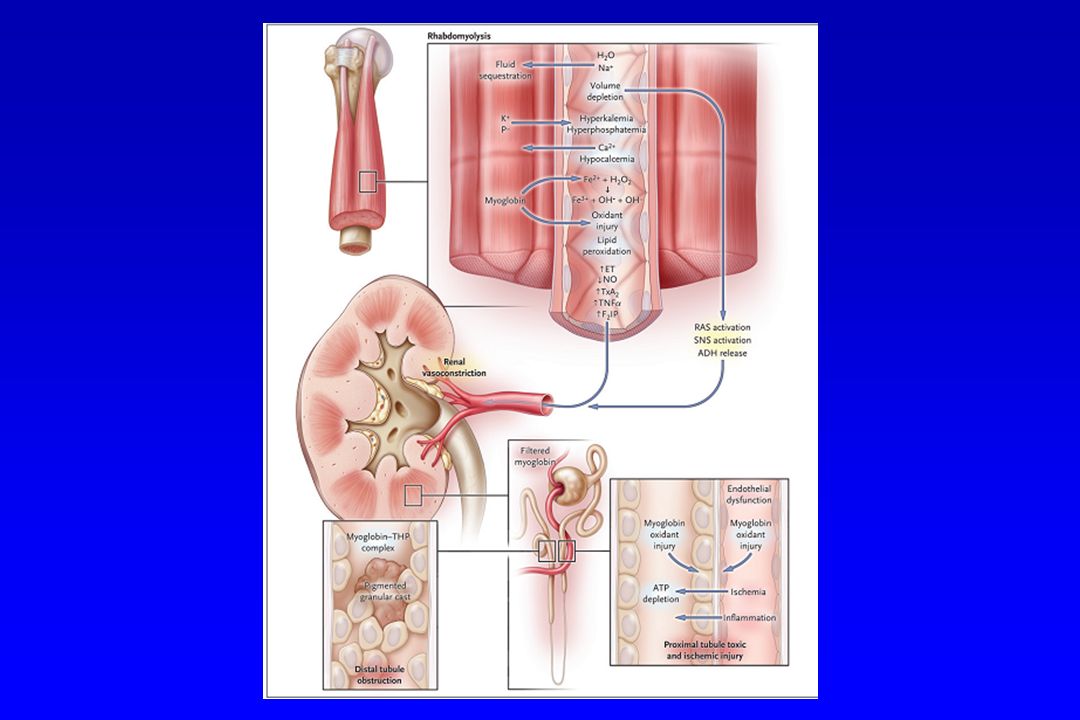
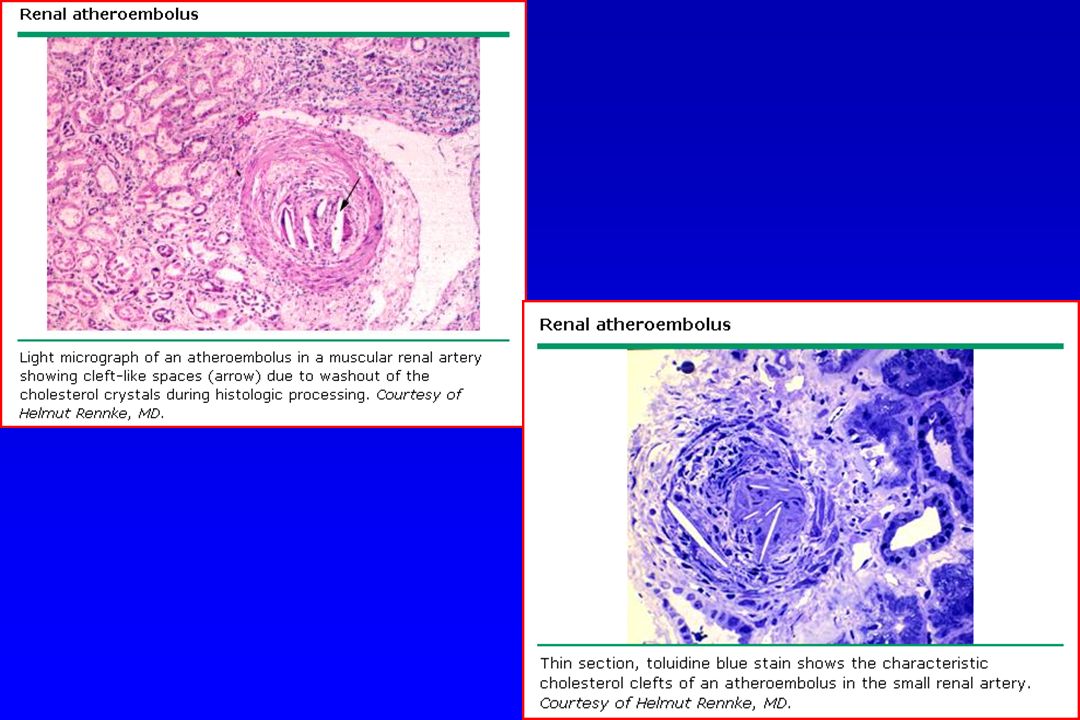
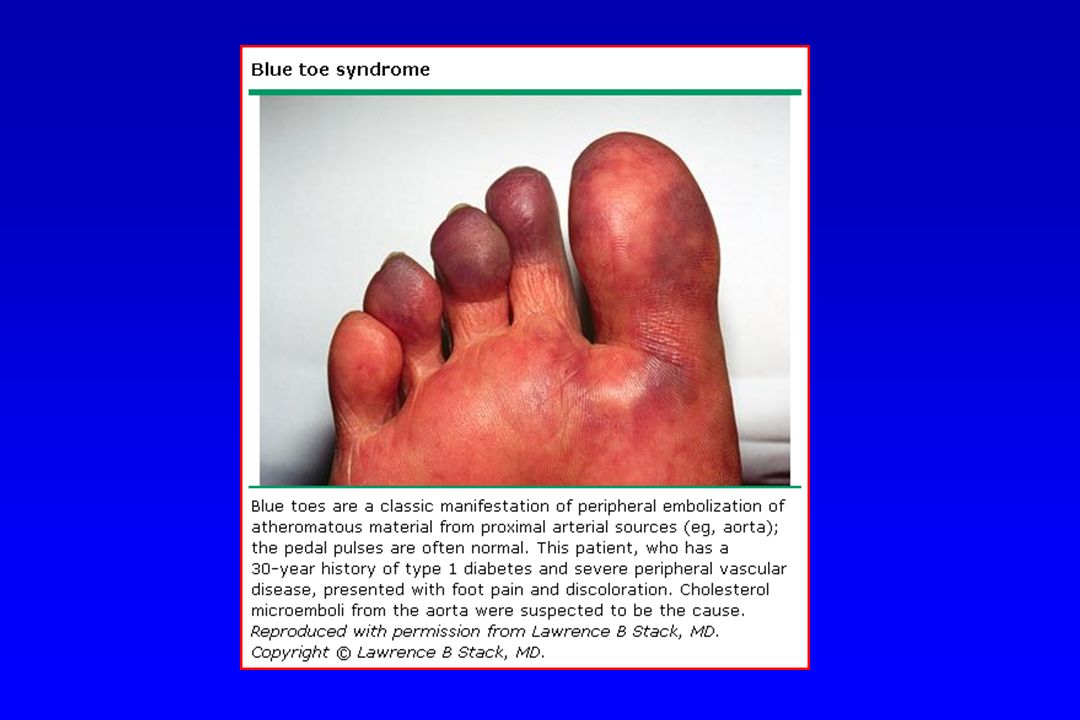
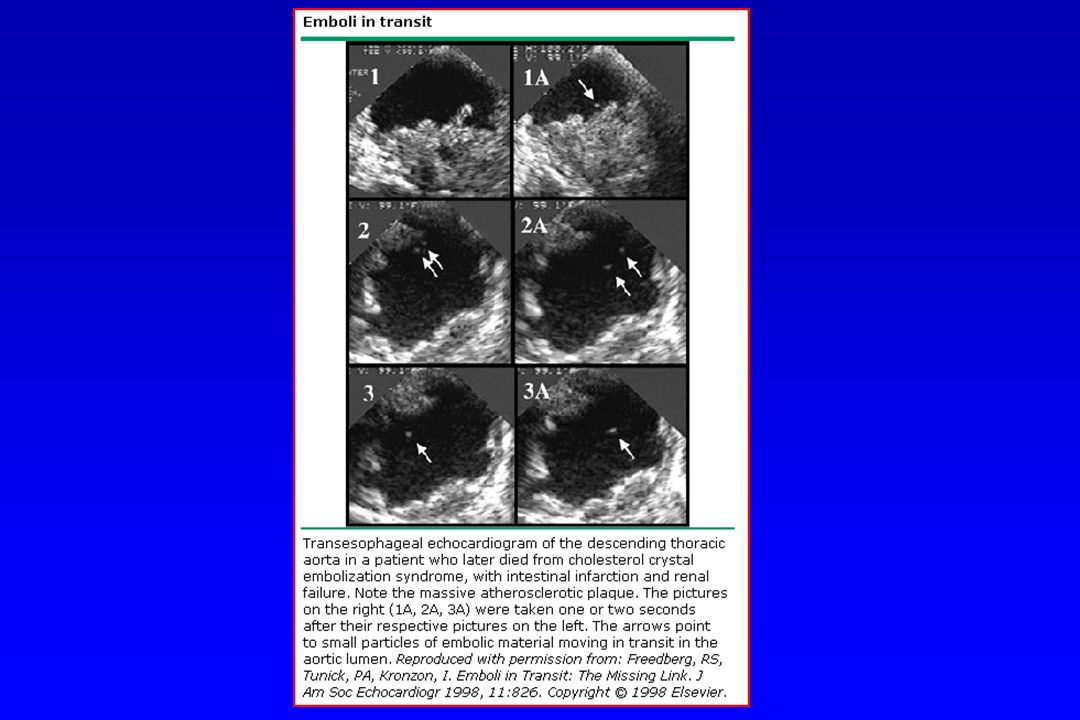
ATEROEMBOLISMO (embolismo por cristais de colesterol) piora da função renal após procedimento endovascular (aguda, sub-aguda ou crônica) urina normal ou com alterações inespecíficas (pode apresentar hematúria, proteinúria ou cilindros) eosinofilía / eosinofilúria hipocomplementemia presença de áreas de livedo reticularis comprometimento de outros territórios: S. dedo azul, trombose mesentérica, etc…
 urina normal ou com alterações inespecíficas. (pode apresentar hematúria, proteinúria ou cilindros) eosinofilía / eosinofilúria. hipocomplementemia. presença de áreas de livedo reticularis. comprometimento de outros territórios: S. dedo azul, trombose mesentérica, etc…")
48
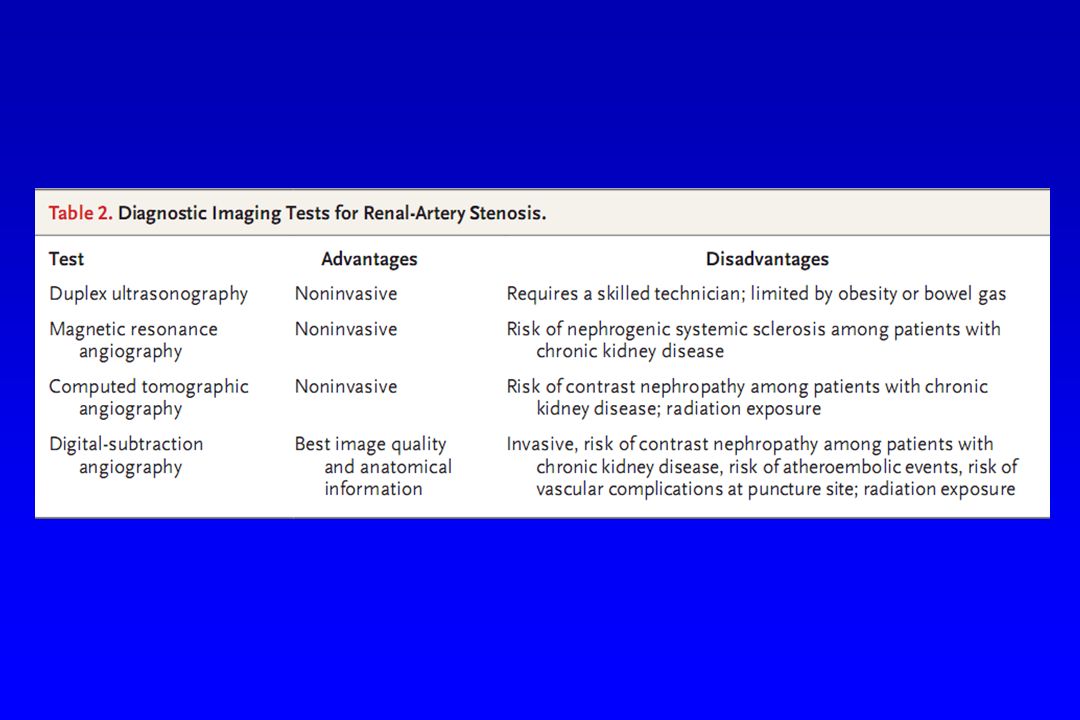
Safian R and Textor S. N Engl J Med 2001;344:431-442

52
ENGELHORN, C.A.; ENGELHORN, A L. ; PULLIG, R.
Arq. Bras. Cardiol. [online]. 2004, vol. 82, no. 5, pp

53
ENGELHORN, C.A.; ENGELHORN, A L. ; PULLIG, R.
Arq. Bras. Cardiol. [online]. 2004, vol. 82, no. 5, pp

54
IECA

55
Perimedial Fibroplasia of the Renal Artery (Panel A) and a Near-Normal Renal Artery after Percutaneous Balloon Angioplasty (Panel B) Figure 2. Perimedial Fibroplasia of the Renal Artery (Panel A) and a Near-Normal Renal Artery after Percutaneous Balloon Angioplasty (Panel B). Careful observation shows that the beads (arrow) in perimedial fibroplasia are less numerous and smaller than those in medial fibroplasia. There is usually a robust collateral circulation in patients with perimedial fibroplasia. (Images courtesy of Anthony W. Stanson, M.D., Mayo Clinic, Rochester, Minnesota.) Slovut D and Olin J. N Engl J Med 2004;350:
 and a Near-Normal Renal Artery after Percutaneous Balloon Angioplasty (Panel B). Careful observation shows that the beads (arrow) in perimedial fibroplasia are less numerous and smaller than those in medial fibroplasia. There is usually a robust collateral circulation in patients with perimedial fibroplasia. (Images courtesy of Anthony W. Stanson, M.D., Mayo Clinic, Rochester, Minnesota.) Slovut D and Olin J. N Engl J Med 2004;350:")
56
Angiographic Appearance of the Two Most Common Forms of Renal-Artery Stenosis
Figure 2. Angiographic Appearance of the Two Most Common Forms of Renal-Artery Stenosis. Panel A shows the typical beaded, aneurysmal appearance of the distal right renal artery in a patient with refractory hypertension and fibromuscular dysplasia. After angioplasty, there was improvement in the angiographic appearance (Panel B) and resolution of hypertension. Panel C shows the typical appearance of atherosclerotic renal-artery stenosis, involving the ostium and proximal third of the left renal artery (arrows). After angioplasty, there was residual stenosis, dissection, and a pressure gradient (arrows in Panel D), which resolved after the placement of a Palmaz stent (arrows in Panel E). (Panels A and B were provided courtesy of Richard Stack, M.D.) Safian R and Textor S. N Engl J Med 2001;344:
 and resolution of hypertension. Panel C shows the typical appearance of atherosclerotic renal-artery stenosis, involving the ostium and proximal third of the left renal artery (arrows). After angioplasty, there was residual stenosis, dissection, and a pressure gradient (arrows in Panel D), which resolved after the placement of a Palmaz stent (arrows in Panel E). (Panels A and B were provided courtesy of Richard Stack, M.D.) Safian R and Textor S. N Engl J Med 2001;344:")
57
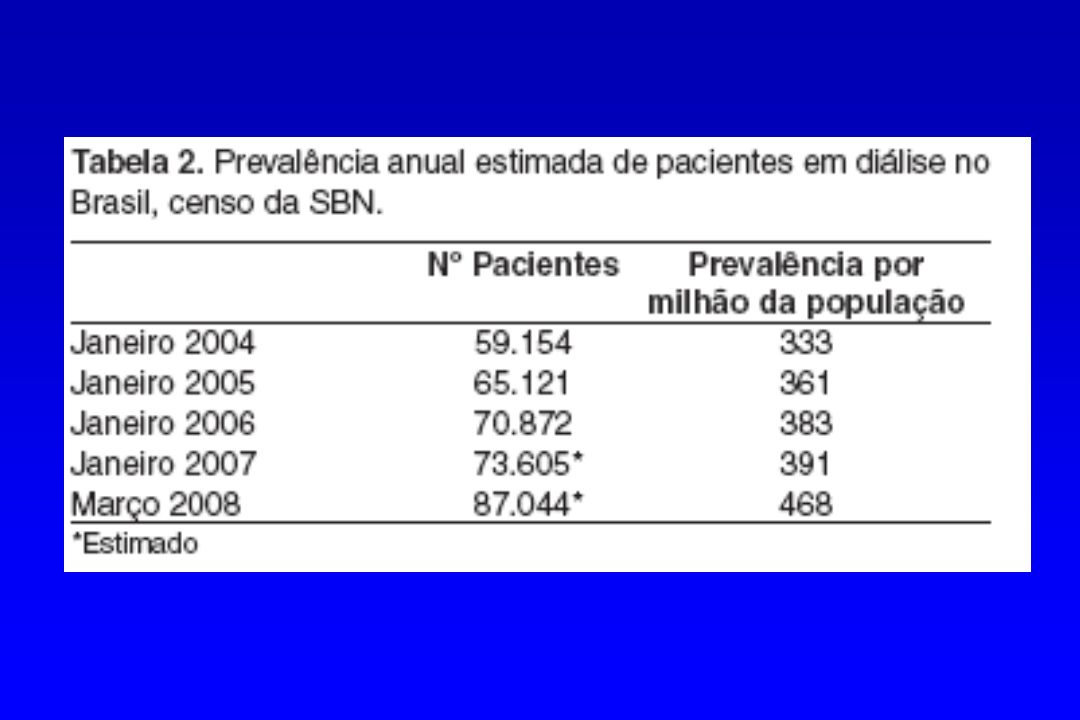
A “epidemia” da IRC

58
USRDS - http://www.usrds.org/

59
USRDS - http://www.usrds.org/

67
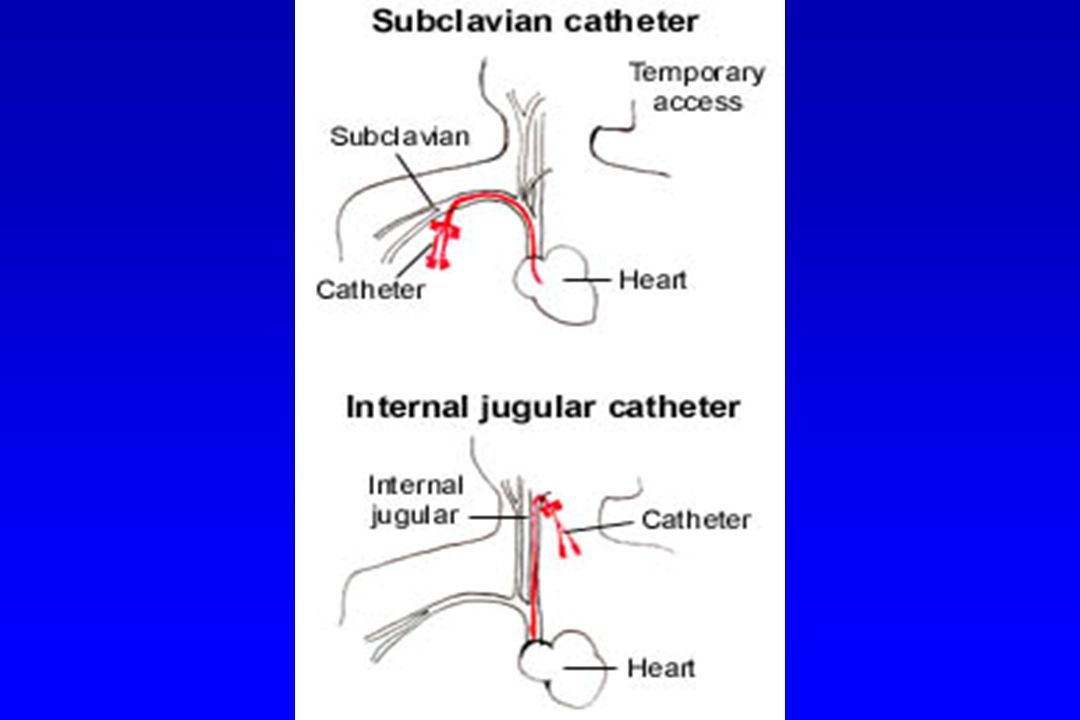
História da hemodiálise
1966: Brescia, Cimino, Appel e Hurwich - Nova York fístula arteriovenosa subcutânea para hemodiálise

72
Figure 1. Estimated Cumulative Mortality after Acute Myocardial Infarction among Patients on Dialysis. The bars indicate standard errors.

Apresentações semelhantes



















>")










