Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Fatores nutricionais e demográficos associados com icterícia colestática prolongada no recém-nascido prematuro Danilo de Melo Gomes Maria Thereza Alves Pontes Internato – ESCS/SES/DF – 2/9/2008 Coordenação: Paulo R. Margotto www.paulomargotto.com.br

2
OBJETIVOS Existe relação entre os níveis de aminoácidos e o desenvolvimento da colestase? Existe relação entre os níveis de aminoácidos e o desenvolvimento da colestase? Identificar fatores de risco associados com o desenvolvimento de icterícia colestática prolongada Identificar fatores de risco associados com o desenvolvimento de icterícia colestática prolongada

3
INTRODUÇÃO Definição de colestase (diminuição da formação e do fluxo da bile) Definição de colestase (diminuição da formação e do fluxo da bile) RN (principalmente RNPT): imaturidade do sistema biliar RN (principalmente RNPT): imaturidade do sistema biliar BD > 5 mg/100ml ou acima de 15% da BT BD > 5 mg/100ml ou acima de 15% da BT
 Definição de colestase (diminuição da formação e do fluxo da bile) RN (principalmente RNPT): imaturidade do sistema biliar RN (principalmente RNPT): imaturidade do sistema biliar BD > 5 mg/100ml ou acima de 15% da BT BD > 5 mg/100ml ou acima de 15% da BT")
4
INTRODUÇÃO Nutrição parenteral como fator de risco Nutrição parenteral como fator de risco Diagnóstico de exclusão Diagnóstico de exclusão Parece não haver diferença na incidência de colestase relacionada à dose de aa na NP Parece não haver diferença na incidência de colestase relacionada à dose de aa na NP

5
MÉTODOS Estudo multicêntrico (n=11 Centros) e randomizado Estudo multicêntrico (n=11 Centros) e randomizado Crianças elegíveis: Crianças elegíveis: 23 a 29 semanas de IG 23 a 29 semanas de IG Menos de 48h de vida à randomização Menos de 48h de vida à randomização Consentimento dos pais Consentimento dos pais RN da própria Unidade de Saúde RN da própria Unidade de Saúde
 e randomizado Estudo multicêntrico (n=11 Centros) e randomizado Crianças elegíveis: Crianças elegíveis: 23 a 29 semanas de IG 23 a 29 semanas de IG Menos de 48h de vida à randomização Menos de 48h de vida à randomização Consentimento dos pais Consentimento dos pais RN da própria Unidade de Saúde RN da própria Unidade de Saúde")
6
MÉTODOS Protocolo aprovado pelas comissões hospitalares Protocolo aprovado pelas comissões hospitalares Critérios de Exclusão Critérios de Exclusão Anomalia congênita ou cromossômica importante Anomalia congênita ou cromossômica importante

7
MÉTODOS Grupo 1 = 2,5 g/Kg/dia Grupo 1 = 2,5 g/Kg/dia 1g + 0,5 g/dia até 2,5g – D4 1g + 0,5 g/dia até 2,5g – D4 Diminuição para 1 g/Kg/dia se alimentação atingisse 80 a 100 ml/Kg/dia Diminuição para 1 g/Kg/dia se alimentação atingisse 80 a 100 ml/Kg/dia Grupo 2 = 3,5 g/Kg/dia Grupo 2 = 3,5 g/Kg/dia 1,5 g + 1 g/dia até 3,5g – D3 1,5 g + 1 g/dia até 3,5g – D3 Diminuição para 2 g/Kg/dia se alimentação atingisse 80 a 100 ml/Kg/dia Diminuição para 2 g/Kg/dia se alimentação atingisse 80 a 100 ml/Kg/dia Interrupção da suplementação de aa se alimentação alcançasse 100 a 130 ml/Kg/dia – Tratamento completado Interrupção da suplementação de aa se alimentação alcançasse 100 a 130 ml/Kg/dia – Tratamento completado Nutrição parenteral subsequente era fornecida a critério da equipe de saúde Nutrição parenteral subsequente era fornecida a critério da equipe de saúde

8
MÉTODOS Comparação das características demográficas e dos níveis de aa entre os RN com e sem colestase Comparação das características demográficas e dos níveis de aa entre os RN com e sem colestase Definição para colestase associada a NP: Definição para colestase associada a NP: BD > 5 mg/100ml a qualquer momento durante os primeiros 28 dias do nascimento BD > 5 mg/100ml a qualquer momento durante os primeiros 28 dias do nascimento Ausência de atresia biliar Ausência de atresia biliar Ausência de hepatite viral Ausência de hepatite viral

9
MÉTODOS Monitorização laboratorial: D0, D7 e D28 Monitorização laboratorial: D0, D7 e D28 Apresentação dos dados = mediana e quartiles (distribuição não normal) Apresentação dos dados = mediana e quartiles (distribuição não normal) Técnicas uni e multivariadas para comparar as diferenças entre os grupos Técnicas uni e multivariadas para comparar as diferenças entre os grupos
 Apresentação dos dados = mediana e quartiles (distribuição não normal) Técnicas uni e multivariadas para comparar as diferenças entre os grupos Técnicas uni e multivariadas para comparar as diferenças entre os grupos")
10
MÉTODOS Variáveis contínuas (IG, peso ao nascer e dose total de proteína) = Student’s t-tests Variáveis contínuas (IG, peso ao nascer e dose total de proteína) = Student’s t-tests Dados contínuos não-paramétricos = Kruskal-Wallis (variância) Dados contínuos não-paramétricos = Kruskal-Wallis (variância) Variáveis categóricas (raça, gênero) = X² e Fisher Variáveis categóricas (raça, gênero) = X² e Fisher P<0,1 na análise univariada para ser incluída na regressão logística P<0,1 na análise univariada para ser incluída na regressão logística Análise estatísica = JPM Release 5.0.1a (SAS Institute Inc, Cary, NC, USA) Análise estatísica = JPM Release 5.0.1a (SAS Institute Inc, Cary, NC, USA)
 = Student’s t-tests Variáveis contínuas (IG, peso ao nascer e dose total de proteína) = Student’s t-tests Dados contínuos não-paramétricos = Kruskal-Wallis (variância) Dados contínuos não-paramétricos = Kruskal-Wallis (variância) Variáveis categóricas (raça, gênero) = X² e Fisher Variáveis categóricas (raça, gênero) = X² e Fisher P<0,1 na análise univariada para ser incluída na regressão logística P<0,1 na análise univariada para ser incluída na regressão logística Análise estatísica = JPM Release 5.0.1a (SAS Institute Inc, Cary, NC, USA) Análise estatísica = JPM Release 5.0.1a (SAS Institute Inc, Cary, NC, USA)")
11
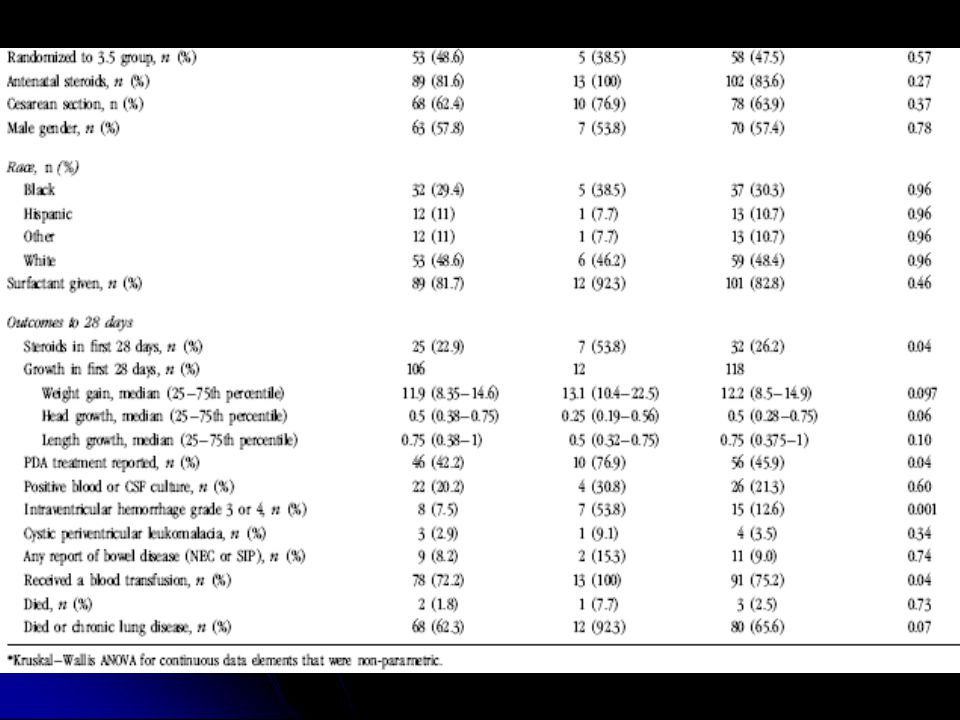
RESULTADOS 122 neonatos – 13 (10,7%) desenvolveram colestase: 122 neonatos – 13 (10,7%) desenvolveram colestase: Mais imaturos Mais imaturos Menor peso ao nascimento Menor peso ao nascimento NP de maior duração NP de maior duração Maior dose cumulativa de aa parenteral Maior dose cumulativa de aa parenteral Menor freqüência de nutrição enteral no 7° dia de vida Menor freqüência de nutrição enteral no 7° dia de vida Maior freqüência de: Maior freqüência de: Ducto arterioso patente Ducto arterioso patente Hemorragia intraventricular severa Hemorragia intraventricular severa Tratamento com esteróides Tratamento com esteróides Transfusão sanguínea Transfusão sanguínea
 desenvolveram colestase: 122 neonatos – 13 (10,7%) desenvolveram colestase: Mais imaturos Mais imaturos Menor peso ao nascimento Menor peso ao nascimento NP de maior duração NP de maior duração Maior dose cumulativa de aa parenteral Maior dose cumulativa de aa parenteral Menor freqüência de nutrição enteral no 7° dia de vida Menor freqüência de nutrição enteral no 7° dia de vida Maior freqüência de: Maior freqüência de: Ducto arterioso patente Ducto arterioso patente Hemorragia intraventricular severa Hemorragia intraventricular severa Tratamento com esteróides Tratamento com esteróides Transfusão sanguínea Transfusão sanguínea")
12
RESULTADOS Controle laboratorial Controle laboratorial Não houve diferença no D0 Não houve diferença no D0 D7 (fase enteral): aumento da uréia, citrulina, histidina, metionina e succinilcarnitina nos RN com colestase D7 (fase enteral): aumento da uréia, citrulina, histidina, metionina e succinilcarnitina nos RN com colestase D7: glutamato, serina e tiroxina diminuídos nos RN com e sem colestase D7: glutamato, serina e tiroxina diminuídos nos RN com e sem colestase A ÚNICA VARIÁVEL INDEPENDENTE ASSOCIADA COM AUMENTO DO RISCO DE COLESTASE FOI A DOSE TOTAL DE PROTEÍNA A ÚNICA VARIÁVEL INDEPENDENTE ASSOCIADA COM AUMENTO DO RISCO DE COLESTASE FOI A DOSE TOTAL DE PROTEÍNA
: aumento da uréia, citrulina, histidina, metionina e succinilcarnitina nos RN com colestase D7 (fase enteral): aumento da uréia, citrulina, histidina, metionina e succinilcarnitina nos RN com colestase D7: glutamato, serina e tiroxina diminuídos nos RN com e sem colestase D7: glutamato, serina e tiroxina diminuídos nos RN com e sem colestase A ÚNICA VARIÁVEL INDEPENDENTE ASSOCIADA COM AUMENTO DO RISCO DE COLESTASE FOI A DOSE TOTAL DE PROTEÍNA A ÚNICA VARIÁVEL INDEPENDENTE ASSOCIADA COM AUMENTO DO RISCO DE COLESTASE FOI A DOSE TOTAL DE PROTEÍNA")
17
DISCUSSÃO Estudos prévios relacionam os seguintes fatores com a colestase: Estudos prévios relacionam os seguintes fatores com a colestase: Imaturidade (26 x 27 sem – p=0,02) Imaturidade (26 x 27 sem – p=0,02) Extremo baixo peso ao nascer (800g x 990g – p=0,04) Extremo baixo peso ao nascer (800g x 990g – p=0,04) Quantidade (dose total e não diária) e formulação de aa via parenteral (91,5 x 38,5 g/Kg – p=0,001) Quantidade (dose total e não diária) e formulação de aa via parenteral (91,5 x 38,5 g/Kg – p=0,001) Ingesta calórica excessiva (gordura, carboidratos) Ingesta calórica excessiva (gordura, carboidratos) Toxicidade de sais minerais Toxicidade de sais minerais Sexo masculino Sexo masculino Asfixia perinatal Asfixia perinatal Fototoxicidade de suplementos multivitamínicos Fototoxicidade de suplementos multivitamínicos Toxicidade de fitosteróis de plantas Toxicidade de fitosteróis de plantas Predisposição genética Predisposição genética Duração na NP (27d x 16d – p=0,01) Duração na NP (27d x 16d – p=0,01)
 Imaturidade (26 x 27 sem – p=0,02) Extremo baixo peso ao nascer (800g x 990g – p=0,04) Extremo baixo peso ao nascer (800g x 990g – p=0,04) Quantidade (dose total e não diária) e formulação de aa via parenteral (91,5 x 38,5 g/Kg – p=0,001) Quantidade (dose total e não diária) e formulação de aa via parenteral (91,5 x 38,5 g/Kg – p=0,001) Ingesta calórica excessiva (gordura, carboidratos) Ingesta calórica excessiva (gordura, carboidratos) Toxicidade de sais minerais Toxicidade de sais minerais Sexo masculino Sexo masculino Asfixia perinatal Asfixia perinatal Fototoxicidade de suplementos multivitamínicos Fototoxicidade de suplementos multivitamínicos Toxicidade de fitosteróis de plantas Toxicidade de fitosteróis de plantas Predisposição genética Predisposição genética Duração na NP (27d x 16d – p=0,01) Duração na NP (27d x 16d – p=0,01)")
18
DISCUSSÃO Difícil avaliação da toxicidade das altas doses de aa administradas via parenteral Difícil avaliação da toxicidade das altas doses de aa administradas via parenteral Aa hepatotóxicos: metionina, fenilalanina, tirosina e triptofano Aa hepatotóxicos: metionina, fenilalanina, tirosina e triptofano Podem reduzir a injúria hepática: glutamina e taurina Podem reduzir a injúria hepática: glutamina e taurina

19
DISCUSSÃO Difícil avaliação da toxicidade das altas doses de aa administradas via parenteral Difícil avaliação da toxicidade das altas doses de aa administradas via parenteral Aa hepatotóxicos: metionina, fenilalanina, tirosina e triptofano Aa hepatotóxicos: metionina, fenilalanina, tirosina e triptofano Podem reduzir a injúria hepática: glutamina e taurina Podem reduzir a injúria hepática: glutamina e taurina

20
DISCUSSÃO Alterações laboatoriais: causa ou conseqüência? Alterações laboatoriais: causa ou conseqüência? Monitorização dos níveis de aa: identifica RN com risco de desenvolver colestase e evitam doses hepatotóxicas Monitorização dos níveis de aa: identifica RN com risco de desenvolver colestase e evitam doses hepatotóxicas Alimentação enteral – estímulo da função entero- hepática Alimentação enteral – estímulo da função entero- hepática NP: gastrina e colecistoquinina reduzidas, com redução do transporte biliar NP: gastrina e colecistoquinina reduzidas, com redução do transporte biliar

21
DISCUSSÃO Tratamento com esteróides nos primeiros 28 dias de vida (marcador de doença) Tratamento com esteróides nos primeiros 28 dias de vida (marcador de doença) Níveis baixos de tiroxina e risco de colestase: risco indefinido Níveis baixos de tiroxina e risco de colestase: risco indefinido Grau de imaturidade ou severidade da doença (transfusão, hemorragia, esteróides, ducto arterioso, tiroxina) Grau de imaturidade ou severidade da doença (transfusão, hemorragia, esteróides, ducto arterioso, tiroxina)
 Tratamento com esteróides nos primeiros 28 dias de vida (marcador de doença) Níveis baixos de tiroxina e risco de colestase: risco indefinido Níveis baixos de tiroxina e risco de colestase: risco indefinido Grau de imaturidade ou severidade da doença (transfusão, hemorragia, esteróides, ducto arterioso, tiroxina) Grau de imaturidade ou severidade da doença (transfusão, hemorragia, esteróides, ducto arterioso, tiroxina)")
22
CONCLUSÃO Colestase: complicação comum e importante da NP em neonatos prematuros Colestase: complicação comum e importante da NP em neonatos prematuros Marcadores metabólicos de risco Marcadores metabólicos de risco Necessidade de estudos mais detalhados para otimizar a NP para os neonatos prematuros criticamente doentes Necessidade de estudos mais detalhados para otimizar a NP para os neonatos prematuros criticamente doentes

23
Abstract Abstract Objective: Objective: The primary aim of this study was to determine if an association exists between amino- acid levels and development of cholestasis. The secondary aim of our amino-acid dose comparison trial was to identify factors associated with the development of prolonged cholestatic jaundice. The primary aim of this study was to determine if an association exists between amino- acid levels and development of cholestasis. The secondary aim of our amino-acid dose comparison trial was to identify factors associated with the development of prolonged cholestatic jaundice. Study Design: Study Design: We compared demographic characteristics and amino-acid levels in neonates who developed cholestasis with those who did not. Parenteral-associated cholestatic liver disease was defined as a direct serum bilirubin above 5 mg per 100 ml any time during the first 28 days after birth in neonates with no history of biliary atresia or viral hepatitis. We obtained filter paper blood spots for amino acid and acylcarnitine measurements on the day of randomization and days 7 and 28 of age to identify a profile of values that could be used to identify neonates with evidence of abnormal liver function. We compared demographic characteristics and amino-acid levels in neonates who developed cholestasis with those who did not. Parenteral-associated cholestatic liver disease was defined as a direct serum bilirubin above 5 mg per 100 ml any time during the first 28 days after birth in neonates with no history of biliary atresia or viral hepatitis. We obtained filter paper blood spots for amino acid and acylcarnitine measurements on the day of randomization and days 7 and 28 of age to identify a profile of values that could be used to identify neonates with evidence of abnormal liver function. Result: Result: We enrolled 122 neonates in our study; 13 (10.7%) developed cholestasis. Neonates who developed cholestasis were more immature, had lower birth weight, were exposed to parenteral nutrition for a longer period, had a higher cumulative dose of amino acids, were less often on enteral nutrition by day 7 of age, more often had a patent ductus arteriosus and severe intraventricular hemorrhage and were more commonly treated with steroids by 28 days of age. Amino acid and acylcarnitine values were not different for the two groups on the day of randomization. On day 7 (parenteral phase of nutrition), blood urea nitrogen, citrulline, histidine, methionine and succinyl carnitine were higher, and serine, glutamate and thyroxine levels were lower in the neonates who developed cholestasis than in who did not. We enrolled 122 neonates in our study; 13 (10.7%) developed cholestasis. Neonates who developed cholestasis were more immature, had lower birth weight, were exposed to parenteral nutrition for a longer period, had a higher cumulative dose of amino acids, were less often on enteral nutrition by day 7 of age, more often had a patent ductus arteriosus and severe intraventricular hemorrhage and were more commonly treated with steroids by 28 days of age. Amino acid and acylcarnitine values were not different for the two groups on the day of randomization. On day 7 (parenteral phase of nutrition), blood urea nitrogen, citrulline, histidine, methionine and succinyl carnitine were higher, and serine, glutamate and thyroxine levels were lower in the neonates who developed cholestasis than in who did not. Conclusion: Conclusion: Cholestasis remains an important complication of parenteral nutrition, and several clinical and biochemical factors may be helpful in identifying high-risk patients. Cholestasis remains an important complication of parenteral nutrition, and several clinical and biochemical factors may be helpful in identifying high-risk patients.
 developed cholestasis. Neonates who developed cholestasis were more immature, had lower birth weight, were exposed to parenteral nutrition for a longer period, had a higher cumulative dose of amino acids, were less often on enteral nutrition by day 7 of age, more often had a patent ductus arteriosus and severe intraventricular hemorrhage and were more commonly treated with steroids by 28 days of age. Amino acid and acylcarnitine values were not different for the two groups on the day of randomization. On day 7 (parenteral phase of nutrition), blood urea nitrogen, citrulline, histidine, methionine and succinyl carnitine were higher, and serine, glutamate and thyroxine levels were lower in the neonates who developed cholestasis than in who did not. We enrolled 122 neonates in our study; 13 (10.7%) developed cholestasis. Neonates who developed cholestasis were more immature, had lower birth weight, were exposed to parenteral nutrition for a longer period, had a higher cumulative dose of amino acids, were less often on enteral nutrition by day 7 of age, more often had a patent ductus arteriosus and severe intraventricular hemorrhage and were more commonly treated with steroids by 28 days of age. Amino acid and acylcarnitine values were not different for the two groups on the day of randomization. On day 7 (parenteral phase of nutrition), blood urea nitrogen, citrulline, histidine, methionine and succinyl carnitine were higher, and serine, glutamate and thyroxine levels were lower in the neonates who developed cholestasis than in who did not. Conclusion: Conclusion: Cholestasis remains an important complication of parenteral nutrition, and several clinical and biochemical factors may be helpful in identifying high-risk patients. Cholestasis remains an important complication of parenteral nutrition, and several clinical and biochemical factors may be helpful in identifying high-risk patients..")
24
Referências do artigo: Venigalla S, Gourley GR. Neonatal cholestasis. Semin Perinatol 2004; 28: 348–355. | Article | PubMed | Venigalla S, Gourley GR. Neonatal cholestasis. Semin Perinatol 2004; 28: 348–355. | Article | PubMed |ArticlePubMedArticlePubMed Emerick KM, Whitington PF. Molecular basis of neonatal cholestasis. Pediatr Clin North Am 2002; 49: 221–235. | Article | PubMed | Emerick KM, Whitington PF. Molecular basis of neonatal cholestasis. Pediatr Clin North Am 2002; 49: 221–235. | Article | PubMed |ArticlePubMedArticlePubMed Karpen SJ. Update on the etiologies and management of neonatal cholestasis. Clin Perinatol 2002; 29: 159–180. | Article | PubMed | Karpen SJ. Update on the etiologies and management of neonatal cholestasis. Clin Perinatol 2002; 29: 159–180. | Article | PubMed |ArticlePubMedArticlePubMed Peden VH, Witzleben CL, Skelton MA. Total parenteral nutrition. J Pediatr 1971; 78: 180–181. | PubMed | ChemPort | Peden VH, Witzleben CL, Skelton MA. Total parenteral nutrition. J Pediatr 1971; 78: 180–181. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Teitelbaum DH, Tracy T. Parenteral nutrition-associated cholestasis. Semin Pediatr Surg 2001; 10: 72–80. | Article | PubMed | ChemPort | Teitelbaum DH, Tracy T. Parenteral nutrition-associated cholestasis. Semin Pediatr Surg 2001; 10: 72–80. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Clark RH, Chace DH, Spitzer AR. The effects of two different doses of amino acid administration on growth and blood amino acids in premature neonates admitted to the NICU: a randomized controlled trial. Pediatrics 2007 (in press). Clark RH, Chace DH, Spitzer AR. The effects of two different doses of amino acid administration on growth and blood amino acids in premature neonates admitted to the NICU: a randomized controlled trial. Pediatrics 2007 (in press). Spencer AU, Yu S, Tracy TF, Aouthmany MM, Llanos A, Brown MB et al. Parenteral nutrition-associated cholestasis in neonates: multivariate analysis of the potential protective effect of taurine. JPEN J Parenter Enteral Nutr 2005; 29: 337–343. | PubMed | ChemPort | Spencer AU, Yu S, Tracy TF, Aouthmany MM, Llanos A, Brown MB et al. Parenteral nutrition-associated cholestasis in neonates: multivariate analysis of the potential protective effect of taurine. JPEN J Parenter Enteral Nutr 2005; 29: 337–343. | PubMed | ChemPort |PubMedChemPortPubMedChemPort
. Clark RH, Chace DH, Spitzer AR. The effects of two different doses of amino acid administration on growth and blood amino acids in premature neonates admitted to the NICU: a randomized controlled trial. Pediatrics 2007 (in press). Spencer AU, Yu S, Tracy TF, Aouthmany MM, Llanos A, Brown MB et al. Parenteral nutrition-associated cholestasis in neonates: multivariate analysis of the potential protective effect of taurine. JPEN J Parenter Enteral Nutr 2005; 29: 337–343. | PubMed | ChemPort | Spencer AU, Yu S, Tracy TF, Aouthmany MM, Llanos A, Brown MB et al. Parenteral nutrition-associated cholestasis in neonates: multivariate analysis of the potential protective effect of taurine. JPEN J Parenter Enteral Nutr 2005; 29: 337–343. | PubMed | ChemPort |PubMedChemPortPubMedChemPort.")
25
Zambrano E, El Hennawy M, Ehrenkranz RA, Zelterman D, Reyes-Mugica M. Total parenteral nutrition induced liver pathology: an autopsy series of 24 newborn cases. Pediatr Dev Pathol 2004; 7: 425–432. | Article | PubMed | Zambrano E, El Hennawy M, Ehrenkranz RA, Zelterman D, Reyes-Mugica M. Total parenteral nutrition induced liver pathology: an autopsy series of 24 newborn cases. Pediatr Dev Pathol 2004; 7: 425–432. | Article | PubMed |ArticlePubMedArticlePubMed Suchy FJ, Balistreri WF, Heubi JE, Searcy JE, Levin RS. Physiologic cholestasis: elevation of the primary serum bile acid concentrations in normal infants. Gastroenterology 1981; 80: 1037– 1041. | PubMed | ChemPort | Suchy FJ, Balistreri WF, Heubi JE, Searcy JE, Levin RS. Physiologic cholestasis: elevation of the primary serum bile acid concentrations in normal infants. Gastroenterology 1981; 80: 1037– 1041. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Colomb V, Jobert-Giraud A, Lacaille F, Goulet O, Fournet JC, Ricour C. Role of lipid emulsions in cholestasis associated with long-term parenteral nutrition in children. JPEN J Parenter Enteral Nutr 2000; 24: 345–350. | PubMed | ChemPort | Colomb V, Jobert-Giraud A, Lacaille F, Goulet O, Fournet JC, Ricour C. Role of lipid emulsions in cholestasis associated with long-term parenteral nutrition in children. JPEN J Parenter Enteral Nutr 2000; 24: 345–350. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Krawinkel MB. Parenteral nutrition-associated cholestasis—what do we know, what can we do? Eur J Pediatr Surg 2004; 14: 230–234. | Article | PubMed | ChemPort | Krawinkel MB. Parenteral nutrition-associated cholestasis—what do we know, what can we do? Eur J Pediatr Surg 2004; 14: 230–234. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Bougle D, Bureau F, Deschrevel G, Hecquard C, Neuville D, Drosdowsky M et al. Chromium and parenteral nutrition in children. J Pediatr Gastroenterol Nutr 1993; 17: 72– 74. | PubMed | ChemPort | Bougle D, Bureau F, Deschrevel G, Hecquard C, Neuville D, Drosdowsky M et al. Chromium and parenteral nutrition in children. J Pediatr Gastroenterol Nutr 1993; 17: 72– 74. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Bove KE, Kosmetatos N, Wedig KE, Frank DJ, Whitlatch S, Saldivar V et al. Vasculopathic hepatotoxicity associated with E-Ferol syndrome in low-birth-weight infants. JAMA 1985; 254: 2422–2430. | Article | PubMed | ChemPort | Bove KE, Kosmetatos N, Wedig KE, Frank DJ, Whitlatch S, Saldivar V et al. Vasculopathic hepatotoxicity associated with E-Ferol syndrome in low-birth-weight infants. JAMA 1985; 254: 2422–2430. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Erikson KM, Thompson K, Aschner J, Aschner M. Manganese neurotoxicity: a focus on the neonate. Pharmacol Ther 2007; 113: 369–377. | Article | PubMed | ChemPort | Erikson KM, Thompson K, Aschner J, Aschner M. Manganese neurotoxicity: a focus on the neonate. Pharmacol Ther 2007; 113: 369–377. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Forbes A, Jawhari A. Manganese toxicity and parenteral nutrition. Lancet 1996; 347: 1774. | Article | PubMed | ChemPort | Forbes A, Jawhari A. Manganese toxicity and parenteral nutrition. Lancet 1996; 347: 1774. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Klein GL. Aluminum: new recognition of an old problem. Curr Opin Pharmacol 2005; 5: 637– 640. | Article | PubMed | ChemPort | Klein GL. Aluminum: new recognition of an old problem. Curr Opin Pharmacol 2005; 5: 637– 640. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort

26
Albers MJ, Gast-Bakker DA, van Dam NA, Madern GC, Tibboel D. Male sex predisposes the newborn surgical patient to parenteral nutrition-associated cholestasis and to sepsis. Arch Surg 2002; 137: 789–793. | Article | PubMed | Albers MJ, Gast-Bakker DA, van Dam NA, Madern GC, Tibboel D. Male sex predisposes the newborn surgical patient to parenteral nutrition-associated cholestasis and to sepsis. Arch Surg 2002; 137: 789–793. | Article | PubMed |ArticlePubMedArticlePubMed Herzog D, Chessex P, Martin S, Alvarez F. Transient cholestasis in newborn infants with perinatal asphyxia. Can J Gastroenterol 2003; 17: 179– 182. | PubMed | ChemPort | Herzog D, Chessex P, Martin S, Alvarez F. Transient cholestasis in newborn infants with perinatal asphyxia. Can J Gastroenterol 2003; 17: 179– 182. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Chessex P, Lavoie JC, Rouleau T, Brochu P, St Louis P, Levy E et al. Photooxidation of parenteral multivitamins induces hepatic steatosis in a neonatal guinea pig model of intravenous nutrition. Pediatr Res 2002; 52: 958–963. | PubMed | ChemPort | Chessex P, Lavoie JC, Rouleau T, Brochu P, St Louis P, Levy E et al. Photooxidation of parenteral multivitamins induces hepatic steatosis in a neonatal guinea pig model of intravenous nutrition. Pediatr Res 2002; 52: 958–963. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Chessex P, Friel J, Harrison A, Rouleau T, Lavoie JC. The mode of delivery of parenteral multivitamins influences nutrient handling in an animal model of total parenteral nutrition. Clin Nutr 2005; 24: 281–287. | Article | PubMed | ChemPort | Chessex P, Friel J, Harrison A, Rouleau T, Lavoie JC. The mode of delivery of parenteral multivitamins influences nutrient handling in an animal model of total parenteral nutrition. Clin Nutr 2005; 24: 281–287. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Silvers KM, Darlow BA, Winterbourn CC. Lipid peroxide and hydrogen peroxide formation in parenteral nutrition solutions containing multivitamins. JPEN J Parenter Enteral Nutr 2001; 25: 14–17. | PubMed | ChemPort | Silvers KM, Darlow BA, Winterbourn CC. Lipid peroxide and hydrogen peroxide formation in parenteral nutrition solutions containing multivitamins. JPEN J Parenter Enteral Nutr 2001; 25: 14–17. | PubMed | ChemPort |PubMedChemPortPubMedChemPort Clayton PT, Whitfield P, Iyer K. The role of phytosterols in the pathogenesis of liver complications of pediatric parenteral nutrition. Nutrition 1998; 14: 158– 164. | Article | PubMed | ChemPort | Clayton PT, Whitfield P, Iyer K. The role of phytosterols in the pathogenesis of liver complications of pediatric parenteral nutrition. Nutrition 1998; 14: 158– 164. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Bindl L, Lutjohann D, Buderus S, Lentze MJ, Bergmann K. High plasma levels of phytosterols in patients on parenteral nutrition: a marker of liver dysfunction. J Pediatr Gastroenterol Nutr 2000; 31: 313–316. | Article | PubMed | ChemPort | Bindl L, Lutjohann D, Buderus S, Lentze MJ, Bergmann K. High plasma levels of phytosterols in patients on parenteral nutrition: a marker of liver dysfunction. J Pediatr Gastroenterol Nutr 2000; 31: 313–316. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort

27
Thureen PJ, Hay Jr WW. Early aggressive nutrition in preterm infants. Semin Neonatol 2001; 6: 403– 415. | Article | PubMed | ChemPort | Thureen PJ, Hay Jr WW. Early aggressive nutrition in preterm infants. Semin Neonatol 2001; 6: 403– 415. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Thureen PJ, Melara D, Fennessey PV, Hay Jr WW. Effect of low versus high intravenous amino acid intake on very low birth weight infants in the early neonatal period. Pediatr Res 2003; 53: 24– 32. | Article | PubMed | ISI | ChemPort | Thureen PJ, Melara D, Fennessey PV, Hay Jr WW. Effect of low versus high intravenous amino acid intake on very low birth weight infants in the early neonatal period. Pediatr Res 2003; 53: 24– 32. | Article | PubMed | ISI | ChemPort |ArticlePubMedISIChemPortArticlePubMedISIChemPort Kotsopoulos K, Benadiba-Torch A, Cuddy A, Shah PS. Safety and efficacy of early amino acids in preterm <28 weeks gestation: prospective observational comparison. J Perinatol 2006; 26: 749– 754. | Article | PubMed | ChemPort | Kotsopoulos K, Benadiba-Torch A, Cuddy A, Shah PS. Safety and efficacy of early amino acids in preterm <28 weeks gestation: prospective observational comparison. J Perinatol 2006; 26: 749– 754. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Poindexter BB, Langer JC, Dusick AM, Ehrenkranz RA. Early provision of parenteral amino acids in extremely low birth weight infants: relation to growth and neurodevelopmental outcome. J Pediatr 2006; 148: 300– 305. | Article | PubMed | ChemPort | Poindexter BB, Langer JC, Dusick AM, Ehrenkranz RA. Early provision of parenteral amino acids in extremely low birth weight infants: relation to growth and neurodevelopmental outcome. J Pediatr 2006; 148: 300– 305. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Clark RH, Wagner CL, Merritt RJ, Bloom BT, Neu J, Young TE et al. Nutrition in the neonatal intensive care unit: how do we reduce the incidence of extrauterine growth restriction? J Perinatol 2003; 23: 337– 344. | Article | PubMed | Clark RH, Wagner CL, Merritt RJ, Bloom BT, Neu J, Young TE et al. Nutrition in the neonatal intensive care unit: how do we reduce the incidence of extrauterine growth restriction? J Perinatol 2003; 23: 337– 344. | Article | PubMed |ArticlePubMedArticlePubMed Suita S, Yamanouchi T, Masumoto K, Ogita K, Nakamura M, Taguchi S. Changing profile of parenteral nutrition in pediatric surgery: a 30-year experience at one institute. Surgery 2002; 131: S275–S282. | Article | PubMed | Suita S, Yamanouchi T, Masumoto K, Ogita K, Nakamura M, Taguchi S. Changing profile of parenteral nutrition in pediatric surgery: a 30-year experience at one institute. Surgery 2002; 131: S275–S282. | Article | PubMed |ArticlePubMedArticlePubMed Wright K, Ernst KD, Gaylord MS, Dawson JP, Burnette TM. Increased incidence of parenteral nutrition-associated cholestasis with aminosyn PF compared to trophamine. J Perinatol 2003; 23: 444– 450. | Article | PubMed | ChemPort | Wright K, Ernst KD, Gaylord MS, Dawson JP, Burnette TM. Increased incidence of parenteral nutrition-associated cholestasis with aminosyn PF compared to trophamine. J Perinatol 2003; 23: 444– 450. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Adamkin DH. Total parenteral nutrition-associated cholestasis: prematurity or amino acids? J Perinatol 2003; 23: 437–438. | Article | PubMed | ChemPort | Adamkin DH. Total parenteral nutrition-associated cholestasis: prematurity or amino acids? J Perinatol 2003; 23: 437–438. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Kadrofske MM, Parimi PS, Gruca LL, Kalhan SC. Effect of intravenous amino acids on glutamine and protein kinetics in low-birth-weight preterm infants during the immediate neonatal period. Am J Physiol Endocrinol Metab 2006; 290: E622–E630. | Article | PubMed | ChemPort | Kadrofske MM, Parimi PS, Gruca LL, Kalhan SC. Effect of intravenous amino acids on glutamine and protein kinetics in low-birth-weight preterm infants during the immediate neonatal period. Am J Physiol Endocrinol Metab 2006; 290: E622–E630. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort

28
de Urbina JJ, Jorquera F, Culebras JM, Villares C, Gonzalez-Gallego J, Tunon MJ. Effects of parenteral nutrition supplemented with alanyl-glutamine on nutrition status in rats. JPEN J Parenter Enteral Nutr 2005; 29: 262–265. | PubMed | de Urbina JJ, Jorquera F, Culebras JM, Villares C, Gonzalez-Gallego J, Tunon MJ. Effects of parenteral nutrition supplemented with alanyl-glutamine on nutrition status in rats. JPEN J Parenter Enteral Nutr 2005; 29: 262–265. | PubMed |PubMed Parimi PS, Kadrofske MM, Gruca LL, Hanson RW, Kalhan SC. Amino acids, glutamine, and protein metabolism in very low birth weight infants. Pediatr Res 2005; 58: 1259–1264. | Article | PubMed | ChemPort | Parimi PS, Kadrofske MM, Gruca LL, Hanson RW, Kalhan SC. Amino acids, glutamine, and protein metabolism in very low birth weight infants. Pediatr Res 2005; 58: 1259–1264. | Article | PubMed | ChemPort |ArticlePubMedChemPortArticlePubMedChemPort Poindexter BB, Ehrenkranz RA, Stoll BJ, Wright LL, Poole WK, Oh W et al. Parenteral glutamine supplementation does not reduce the risk of mortality or late- onset sepsis in extremely low birth weight infants. Pediatrics 2004; 113: 1209– 1215. | Article | PubMed | Poindexter BB, Ehrenkranz RA, Stoll BJ, Wright LL, Poole WK, Oh W et al. Parenteral glutamine supplementation does not reduce the risk of mortality or late- onset sepsis in extremely low birth weight infants. Pediatrics 2004; 113: 1209– 1215. | Article | PubMed |ArticlePubMedArticlePubMed Tyson JE, Kennedy KA. Trophic feedings for parenterally fed infants. Cochrane Database Syst Rev 2005; (3): CD000504. | PubMed | Tyson JE, Kennedy KA. Trophic feedings for parenterally fed infants. Cochrane Database Syst Rev 2005; (3): CD000504. | PubMed |PubMed Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev 2000; (2): CD001970. | PubMed | Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev 2000; (2): CD001970. | PubMed |PubMed Unachak K, Dejkhamron P. Primary congenital hypothyroidism: clinical characteristics and etiological study. J Med Assoc Thai 2004; 87: 612–617. | PubMed | Unachak K, Dejkhamron P. Primary congenital hypothyroidism: clinical characteristics and etiological study. J Med Assoc Thai 2004; 87: 612–617. | PubMed |PubMed
: CD | PubMed | Tyson JE, Kennedy KA. Trophic feedings for parenterally fed infants. Cochrane Database Syst Rev 2005; (3): CD | PubMed |PubMed Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev 2000; (2): CD | PubMed | Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev 2000; (2): CD | PubMed |PubMed Unachak K, Dejkhamron P. Primary congenital hypothyroidism: clinical characteristics and etiological study. J Med Assoc Thai 2004; 87: 612–617. | PubMed | Unachak K, Dejkhamron P. Primary congenital hypothyroidism: clinical characteristics and etiological study. J Med Assoc Thai 2004; 87: 612–617. | PubMed |PubMed.")
29
Consultem também: TERAPIA COM O ÁCIDO URSODEOXICÓLICO (UDCA) EM NEONATOS DE MUITO BAIXO PESO AO NASCER COM COLESTASE ASSOCIADA À NUTRIÇÃO PARENTERAL Autor(es): Dr. Paulo R. Margotto Colestase Autor(es): Maria Carolina Guimarães Santos, Elisa de Carvalho Colestase associada a nutrição parenteral (CANP) em recém- nascidos pequenos para a idade gestacional Autor(es): Daniel T. Robinson and Richard A. Ehrenkranz. Apresentação:Cynthia Bettini L. de C. Monteiro, Clarice de Menezes, Alberto Guerra Dias, Paulo R. Margotto COLESTASE ASSOCIADA A NUTRIÇÃO PARENTERAL TOTAL: PREMATURIDADE OU AMINOÁCIDOS ? Autor(es): Paulo R. Margotto
: Maria Carolina Guimarães Santos, Elisa de Carvalho Colestase associada a nutrição parenteral (CANP) em recém- nascidos pequenos para a idade gestacional Autor(es): Daniel T. Robinson and Richard A. Ehrenkranz. Apresentação:Cynthia Bettini L. de C. Monteiro, Clarice de Menezes, Alberto Guerra Dias, Paulo R. Margotto COLESTASE ASSOCIADA A NUTRIÇÃO PARENTERAL TOTAL: PREMATURIDADE OU AMINOÁCIDOS . Autor(es): Paulo R. Margotto.")
30
Ddo Danilo, Dr. Paulo R. Margotto e Dda Maria Thereza OBRIGADO!

Apresentações semelhantes