Carregar apresentação
A apresentação está carregando. Por favor, espere

1
EPILEPSIA Consulta de Epilepsia / UMES Serviço de Neurologia dos HUC
Conceição Bento

2
1 2 O QUE É EPILEPSIA? COMO SE MANIFESTA? COMO SE DIAGNOSTICA?
COMO SE TRATA? 2

3
O QUE É EPILEPSIA?

4
EPILEPSIA = alteração CEREBRAL
em que existe actividade eléctrica anormal, síncrona e excessiva de uma população de neurónios corticais; que se manifesta em episódios clínicos transitórios; recorrentes, não provocados por uma alteração aguda, sistémica ou neurológica; a alteração neurológica que originou as crises mantém-se mesmo quando estas não estão presentes.

5
CRISE: a manifestação clínica da actividade eléctrica transitória, síncrona, anormal e excessiva de uma população de neurónios corticais EPILEPSIA: uma tendência para surgirem crises recorrentes não provocadas por uma alteração sistémica ou neurológica aguda; é uma situação crónica; a alteração neurológica que originou as crises mantém-se mesmo quando estas não estão presentes. A seizure (from the Latin sacire—to take possession of) is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned with care. B. Overview In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other neurological disorders. Finally, we will address some of the main features of the abnormal physiological activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie certain seizure types.
 is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the. central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic. insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable. network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic. treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure. is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned. with care. B. Overview. In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider. some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that. determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic. basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other. neurological disorders. Finally, we will address some of the main features of the abnormal physiological. activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie. certain seizure types.")
6
Hiperexcitabilidade e Hipersincronia
CRISE: a manifestação clínica da actividade eléctrica síncrona, anormal e excessiva de uma população de neurónios corticais Hiperexcitabilidade e Hipersincronia Alteração da estabilidade de redes neuronais A seizure (from the Latin sacire—to take possession of) is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned with care. B. Overview In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other neurological disorders. Finally, we will address some of the main features of the abnormal physiological activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie certain seizure types.
 is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the. central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic. insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable. network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic. treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure. is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned. with care. B. Overview. In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider. some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that. determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic. basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other. neurological disorders. Finally, we will address some of the main features of the abnormal physiological. activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie. certain seizure types.")
7
Hiperexcitabilidade e Hipersincronia
SINCRONIZAÇÃO RÁPIDA DE UM GRUPO NEURÓNIOS Fish RD, Walker MC. Epilepsy. Comprehensive Review and Case Discussions. Hans O Luders . Martin Dunitz, 2001.

8
Hiperexcitabilidade e Hipersincronia
EXCITAÇÃO INIBIÇÃO NORMAL INIBIÇÃO EXCITAÇÃO HIPEREXCITABILIDADE Basic Mechanisms Underlying Seizures and Epilepsy American Epilepsy Society Modificado de White, 2001

9
HIPEREXCITABILIDADE (genética ou adquirida)
NEURÓNIO MEMBRANA CELULAR Tipo, número e distribuição dos canais iónicos Alteração nos canais iónicos dependentes de voltagem Alteração dos receptores de membrana PROCESSOS INTRACELULARES (síntese proteínas, RNAm, ...) ASPECTOS ESTRUTURAIS CONEXÕES INTER-NEURÓNIOS SINAPSES QUÍMICAS Neurotransmissores / Receptores neurotransmissores EPSPs e IPSPs “Arquitectura” da sinapse REDES E CIRCUITOS NEURONAIS “sprouting” de axónios excitatórios Perda de neurónios inibitórios MEIO EXTRACELULAR Alteração nas concentrações iónicas Alteração no espaço extracelular Células da glia ALTERAÇÕES SISTÉMICAS NTS: NTS/NMDS: Glutamato Dopamina Aspartato Noradrenal Ach Serotonina GABA Adenosina Glicina Pept e Prot Taurina H esteróides
 ASPECTOS ESTRUTURAIS. CONEXÕES INTER-NEURÓNIOS. SINAPSES QUÍMICAS. Neurotransmissores / Receptores neurotransmissores. EPSPs e IPSPs. Arquitectura da sinapse. REDES E CIRCUITOS NEURONAIS. sprouting de axónios excitatórios. Perda de neurónios inibitórios. MEIO EXTRACELULAR. Alteração nas concentrações iónicas. Alteração no espaço extracelular. Células da glia. ALTERAÇÕES SISTÉMICAS. NTS: NTS/NMDS: Glutamato Dopamina. Aspartato Noradrenal. Ach Serotonina. GABA Adenosina. Glicina Pept e Prot. Taurina H esteróides.")
10
Devinsky O, Craig JA. Clinical Symposia. Vol 46; N1.
CIBA-GEIGY, 1994.

11
Epileptic neurones exhibits abnormal activity characterized by burst firing with intervening prolonged periods of excitability (spontaneously or in response to afferent stimulation). The paroxysmal depolarization shift (PDS) is an abnormally large prolonged depolarizing post-synaptic potential, which can cause the burst firing of neurones and capable of subsequently exciting other neurones to adopt a similarly abnormal synchronized pattern of firing. Devinsky O, Craig JA. Clinical Symposia. Vol 46; N1. CIBA-GEIGY, 1994.
 is an abnormally large prolonged depolarizing post-synaptic potential, which can cause the burst firing of neurones and capable of subsequently exciting other neurones to adopt a similarly abnormal synchronized pattern of firing. Devinsky O, Craig JA. Clinical Symposia. Vol 46; N1. CIBA-GEIGY,")
12
Fish RD, Walker MC. Epilepsy. Comprehensive Review and Case Discussions.
Hans O Luders . Martin Dunitz, 2001.

13
EPILEPSIA: uma tendência para surgirem crises recorrentes não provocadas por uma alteração sistémica ou neurológica aguda; é uma situação crónica; a alteração neurológica que originou as crises mantém-se mesmo quando estas não estão presentes. A seizure (from the Latin sacire—to take possession of) is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned with care. B. Overview In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other neurological disorders. Finally, we will address some of the main features of the abnormal physiological activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie certain seizure types. EPILEPTOGÉNESE: a sequência de eventos que converte uma rede neuronal normal numa rede hiperexcitável .
 is the clinical manifestation of an abnormal, excessive, hypersynchronous discharge of a population of cortical neurons. Epilepsy is a disorder of the. central nervous system characterized by recurrent seizures unprovoked by an acute systemic or neurologic. insult. Epileptogenesis is the sequence of events that turns a normal neuronal network into a hyperexcitable. network. (Slide 2) Recognizing the distinction between seizures and epilepsy is essential. Epilepsy may require chronic. treatment (with antiepileptic medication and, in some cases, surgery) whereas therapy for an isolated seizure. is directed toward the underlying cause and may not require antiepileptic drugs (AEDs). Furthermore, epilepsy often has profound psychosocial ramifications for the patient, and is thus a diagnosis to be assigned. with care. B. Overview. In order to understand the concepts of seizures, epilepsy and epileptogenesis, we will first consider. some of the basic anatomic and electrophysiologic properties of the cerebral cortex, and the factors that. determine the level of neural activity at the cellular and cell network level. We will then discuss the physiologic. basis of the electroencephalogram (EEG), routinely used in assessing patients with seizures and other. neurological disorders. Finally, we will address some of the main features of the abnormal physiological. activity that occurs within a seizure focus, and present a few of the proposed mechanisms that may underlie. certain seizure types. EPILEPTOGÉNESE: a sequência de eventos que converte uma rede neuronal normal numa rede hiperexcitável .")
14
EPILEPTOGÉNESE: a sequência de eventos que converte uma rede neuronal normal numa rede hiperexcitável . Basic Mechanisms Underlying Seizures and Epilepsy American Epilepsy Society

15
EPILEPTOGÉNESE: a sequência de eventos que converte uma rede neuronal normal numa rede hiperexcitável . Basic Mechanisms Underlying Seizures and Epilepsy American Epilepsy Society

16
E. IDIOPÁTICA: sem qualquer lesão cerebral associada, nem outro sinal ou sintoma neurológico; geneticamente determinada (geralmente existe uma predisposição genética complexa ou raramente a herança de um só gene); geralmente idade dependente. E. SINTOMÁTICA: causada por uma ou mais lesões cerebrais identificáveis (inclui causas genéticas) E. CRIPTOGÉNICA: epilepsia sintomática em que não é possível identificar a etiologia.
 E. CRIPTOGÉNICA: epilepsia sintomática em que não é possível identificar a etiologia.")
17
Devinsky O, Craig JA. Clinical Symposia.
Vol 46; N1. CIBA-GEIGY, 1994.

18
Etiologia – Epilepsias Sintomáticas:
Anomalias do desenvolvimento cortical Esclerose do hipocampo Doenças neurocutâneas Canalopatias Cromossomopatias Anóxia peri-natal Lesões infecciosas Lesões traumáticas Lesões vasculares Lesões tumorais Lesões inflamatórias . . . Alterações estruturais adquiridas Malformações cerebrais congénitas Alterações “metabólicas” INICIO pode ser ou não idade dependente CLÍNICA idade dependente PROGNÓSTICO não idade dependente

19
Esclerose mesial temporal
Glioma Displasia cortical

20
Angioma cavernoso Enfarte

21
COMO SE MANIFESTA?

22
ILAE 2001

23
Noachtar S. Epilepsy. Comprehensive Review and Case Discussions.
Hans O Luders . Martin Dunitz, 2001.

29
ILAE 2001

30
CRISES EPILÉPTICAS: Generalizadas Parciais Não classificadas
COM PERDA DE CONSCIÊNCIA SEM PERDA DE CONSCIÊNCIA GLOSSÁRIO da terminologia descritiva para a semiologia ictal (...) TERMOS GERAIS “6.0. GENERALIZADA (sin. bilateral) – Uma crise cuja semiologia inicial indica (ou é consistente com) o envolvimento global de ambos os hemisférios cerebrais” ILAE 2001
 TERMOS GERAIS GENERALIZADA (sin. bilateral) – Uma crise cuja semiologia inicial indica (ou é consistente com) o envolvimento global de ambos os hemisférios cerebrais ILAE")
31
Parciais Generalizadas
The Patient Guide to Epilepsy. CIBA-GEIGY, 1993.

32
ILAE 1981

33
ILAE 1981

34
AUSÊNCIAS CRISES DIALÉPTICAS TÍPICAS SIMPLES COMPLEXAS ATÍPICAS
CONSCIÊNCIA vigília responsividade memória TÍPICAS SIMPLES COMPLEXAS ATÍPICAS CRISES DIALÉPTICAS CRISES HIPOMOTORAS

35
The Patient Guide to Epilepsy.
CIBA-GEIGY, 1993.

36
MIOCLÓNICAS Duração < 100 mseg c. tónicas - segundos a minutos
“sudden, brief, shock-like contractions” Duração < 100 mseg c. tónicas - segundos a minutos espasmos - ± 1 segundo c. clónicas – repetição ± 2 a 3 c / seg Mioclonias negativas Interrupção do tónus < 500 mseg ILAE 2001

37
Devinsky O, Craig JA. Clinical Symposia.
Vol 46; N1. CIBA-GEIGY, 1994.

38
CRISES TCG Primariamente Generalizadas Secundariamente Generalizadas
Raras antes dos 3 anos Não existem antes dos 6 meses Sub-grupos CTCG MCG TCG MTCG ATCG Fase Pré-Tónico-Clónica: movimento versivo da cabeça e olhos e vocalizações

39
CRISE TÓNIC-CLÓNICO- -GENERALIZADA (TCG)
Devinsky O, Craig JA. Clinical Symposia. Vol 46; N1. CIBA-GEIGY, 1994.

40
SEQUÊNCIAS NAS CRISES GENERALIZADAS
Mioclonia crise TCG Ausência crise TCG Ausência mioclónica crise TCG Ausência mioclonia crise TCG

41
CRISES CLÓNICAS “Repeated, short contractions of various muscle groups usually characterized by jerking or twitching movements recurring at a regular interval between 0.2 and 5 times per second.” Como crises generalizadas isoladas nos adultos são raras. Frequentes como parte das crises TCG ou CTCG. Podem ocorrer nas Epilepsias Mioclónicas Progressivas

42
CRISES TÓNICAS ILAE 2001: Tónico - Aumento sustentado da contracção muscular com duração de poucos segundos ou minutos Parciais/ generalizadas Axial/ membros Na evolução das crises TCG Tónicas Generalizadas: envolvem os músculos axiais e dos membros de forma simétrica e síncrona

43
CRISES ATÓNICAS ILAE 2001: “Perda ou diminuição súbita do tónus muscular sem aparente evento mioclónico ou tónico precedente, durante 1 ou 2 segundos ou mais, envolvendo a musculatura da cabeça, do tronco, da mandíbula ou dos membros” A zona sintomatogénica cortical não está claramente definida; é possível que este fenómeno seja mediado pela formação reticular bulbar (gigantocellular nucleus) que se projecta inferior e bilateralmente no feixe lateral reticuloespinhal inibindo o tónus proximal antigravitacional
 que se projecta inferior e bilateralmente no feixe lateral reticuloespinhal inibindo o tónus proximal antigravitacional.")
44
Parciais - crises parciais simples - crises parciais complexas - crises secundariamente generalizadas

45
CRISE PARCIAL SIMPLES The Patient Guide to Epilepsy. CIBA-GEIGY, 1993.

47
The Patient Guide to Epilepsy.
CIBA-GEIGY, 1993.

48
PARCIAL SIMPLES => TCG
The Patient Guide to Epilepsy. CIBA-GEIGY, 1993.

49
=> PARCIAL COMPLEXA
PARCIAL SIMPLES => PARCIAL COMPLEXA => TCG Devinsky O, Craig JA. Clinical Symposia. Vol 46; N1. CIBA-GEIGY, 1994.

50
ILAE 2001

51
Um Síndrome epiléptico agrupa doentes que têm em comum:
- a idade de início das crises, - o(s) tipo(s) de crises, - a história natural / prognóstico - a presença ou não de outras alterações, - a resposta ao tratamento, - a genética - as alterações do EEG, - a existência ou não de lesão cerebral estrutural
 tipo(s) de crises, - a história natural / prognóstico. - a presença ou não de outras alterações, - a resposta ao tratamento, - a genética. - as alterações do EEG, - a existência ou não de lesão cerebral estrutural.")
52
ILAE 1989

53
ILAE 2001

54
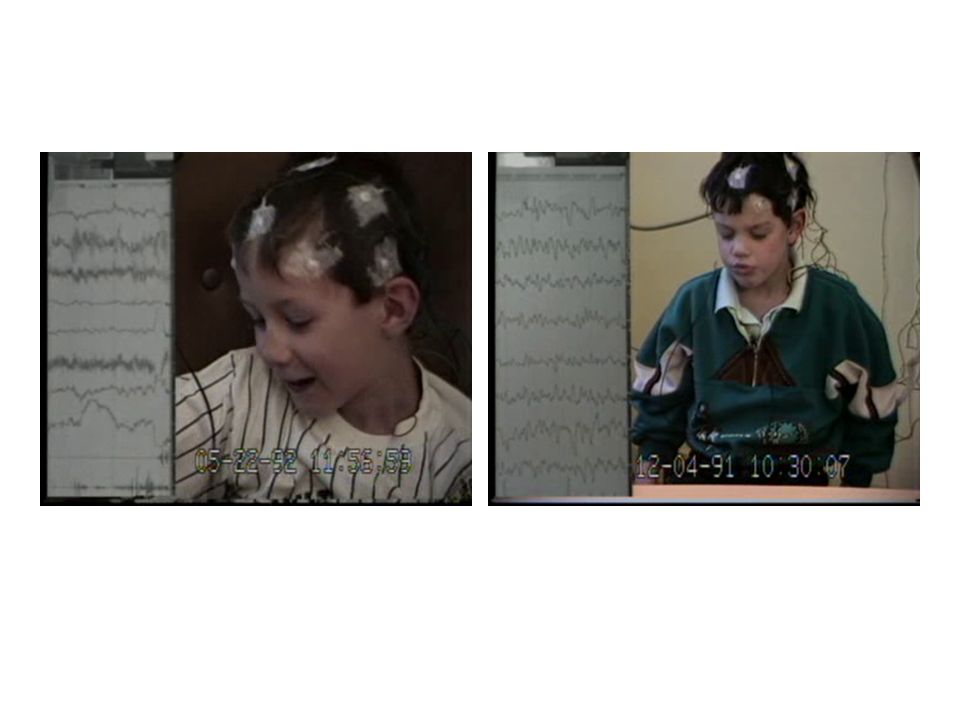
IDADE ESCOLAR - AUSÊNCIAS INFANTIS
- início entre os 4 e os 6 anos - ausências - várias crises por dia - crianças saudáveis (EN normal) - pode haver história de convulsões febris - pode haver uma história familiar positiva - o EEG tem paroxismos generalizados de complexos ponta-onda a 3 Hz frequentemente desencadeados pela HPP - os exames de imagem são normais
 - pode haver história de convulsões febris. - pode haver uma história familiar positiva. - o EEG tem paroxismos generalizados de complexos ponta-onda a 3 Hz frequentemente desencadeados pela HPP. - os exames de imagem são normais.")
55
ADOLESCÊNCIA - EPIL. MIOCLÓNICA JUVENIL
- início entre os 11 e os 14 anos - crises mioclónicas e TCG - adolescentes saudáveis (EN normal) - pode haver uma história familiar positiva - o EEG tem paroxismos generalizados de complexos ponta-onda ou poli-ponta-onda a 3,5-4 Hz - os exames de imagem são normais
 - pode haver uma história familiar positiva. - o EEG tem paroxismos generalizados de complexos ponta-onda ou poli-ponta-onda a 3,5-4 Hz. - os exames de imagem são normais.")
56
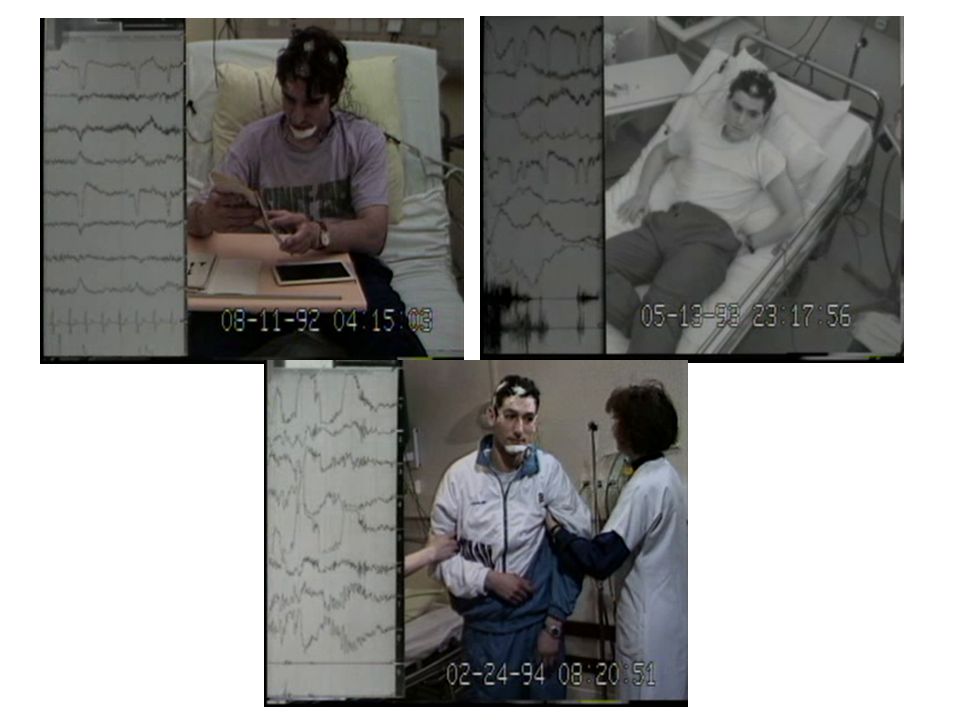
ADULTO - EPILEPSIA TEMPORAL
- início na idade adulta - as crises mais frequentes são de tipo parcial complexo e parcial simples, pode haver menos frequentemente TCG, - várias crises por mês, - pode haver história de convulsões febris, - no EEG existem pontas na região temporal correspondente, - na RMN-CE é frequente a existência de lesão estrutural do lobo temporal

57
ILAE 2001

58
Status epilepticus crises epilépticas
suficientemente prolongadas / com uma duração muito maior que o habitual para o mesmo tipo de crises ou repetidas a intervalos tão breves que produzam “um estado epiléptico mantido” / que não permitam o retorno ao estado basal em termos de função SNC >30 minutos >5-10 minutos WHO / ILAE vários sub-tipos de acordo com o tipo de crise em causa

59
Status convulsivo In: Simon Shorvon. Handbook of Epilepsy Treatment. 2nd edition. Blackwell Publishing, 2005

Apresentações semelhantes