Carregar apresentação
A apresentação está carregando. Por favor, espere

1
Fenótipos em asma Onde estamos? Para onde vamos?
Alberto Cukier Disciplina de Pneumologia - FMUSP

2
Diretrizes manejo asma SBPT 2012

4
Controle da asma com Ceinal isolado ou combinado com LABA…
SF 500 F 500 SF 250 F 250 SF 100 F 100 20 80 40 60 % Sem CEinal 500 µg beclo > < 1000 µg beclo Bateman. Am J Respir Crit Care Med 2004; 170: 836–844 ver 1.4 4 4

5
Não controle da asma com Ceinal isolado ou combinado com LABA…
% 100 80 60 40 20 Sem CEinal 500 µg beclo > < 1000 µg beclo Bateman. Am J Respir Crit Care Med 2004; 170: 836–844 ver 1.4 5 5

6
Quantos pacientes que são tratados de acordo com os consensos participariam dos estudos que definiram as condutas? Travers. Thorax 2007;62:219–223

7
Quantos pacientes que são tratados de acordo com os consensos participariam dos estudos que definiram as condutas? Mediana 6% (0-43%) Travers. Thorax 2007;62:219–223
 Travers. Thorax 2007;62:219–223.")
8
Publicações contendo ‘phenotype’, ‘asthma or wheeze’ e ‘paediatric or child’ no Pubmed
Spycher. Clin Exp Allergy 2010, 40:1130–1141

9
Haldar P. Am J Respir Crit Care Med 2008; 178: 218.
wider approach including clinical, physiologic, and pathologic parameters in a k-means cluster analysis has been performed by Haldar et al. (3). The authors studied two distinct asthma populations: a group from primary care with mild to moderate asthma and a group from secondary care with refractory asthma. In the mild asthma group, three clusters could be identified: (i) early-onset atopic asthma (airway dysfunction, asthma symptoms, and eosinophilic airway inflammation, frequent exacerbations requiring oral corticosteroids), (ii) obese noneosinophilic asthma (preponderance of female subjects, asthma symptoms, absence of eosinophilic airway inflammation), and (iii) benign asthma (middle-aged, little evidence of asthma symptoms, airway inflammation, airway hyperresponsiveness, and exacerbations). In the refractory asthma population, four clusters were identified: (i) early-onset atopic asthma (see earlier text), (ii) obese, noneosinophilic asthma (see earlier text), (iii) early-onset, symptom-predominant asthma (minimal eosinophilic disease), and (iv) eosinophilic inflammation-predominant asthma (few symptoms, late-onset disease, greater proportion of male subjects). The first two clusters were concordant; disease severity differed in cluster 1, which seemed to be strongly associated with a lack of patient compliance. Interestingly, degrees of eosinophilic inflammation and symptoms were discordant in clusters 2 and 3 of the refractory asthma group. This may give rise to overtreatment and treatment failure with inhaled corticosteroids in these groups. Haldar P. Am J Respir Crit Care Med 2008; 178: 218.
. The authors studied two distinct asthma. populations: a group from primary care with mild to moderate. asthma and a group from secondary care with refractory. asthma. In the mild asthma group, three clusters could be. identified: (i) early-onset atopic asthma (airway dysfunction, asthma symptoms, and eosinophilic airway inflammation, frequent. exacerbations requiring oral corticosteroids), (ii) obese. noneosinophilic asthma (preponderance of female subjects, asthma symptoms, absence of eosinophilic airway inflammation), and (iii) benign asthma (middle-aged, little evidence. of asthma symptoms, airway inflammation, airway hyperresponsiveness, and exacerbations). In the refractory asthma. population, four clusters were identified: (i) early-onset atopic. asthma (see earlier text), (ii) obese, noneosinophilic asthma. (see earlier text), (iii) early-onset, symptom-predominant. asthma (minimal eosinophilic disease), and (iv) eosinophilic. inflammation-predominant asthma (few symptoms, late-onset. disease, greater proportion of male subjects). The first two. clusters were concordant; disease severity differed in cluster 1, which seemed to be strongly associated with a lack of patient. compliance. Interestingly, degrees of eosinophilic inflammation. and symptoms were discordant in clusters 2 and 3 of the refractory asthma group. This may give rise to overtreatment. and treatment failure with inhaled corticosteroids in these. groups. Haldar P. Am J Respir Crit Care Med 2008; 178: 218.")
10
Moore WC. Am J Respir Crit Care Med 2010;181:315–23
Clusters no SARP In a study aimed at phenotype identification by clinical features alone, data from 726 subjects from a persistent asthma cohort were analyzed using an unsupervised hierarchical cluster analysis of 34 clinical variables, including age at onset, gender, body weight, degree of airflow limitation, reversibility of airflow limitation, and frequency of asthma exacerbation (39). The authors showed that the resulting fivepatient cluster could be correctly characterized on the basis of onlymerely three clinical parameters: pre- and postbronchodilator percentage of predicted forced expiratory volume in 1 s and age of onset of asthma. However, this cluster did not correlate with the terms “severe asthma” and “treatment refractory asthma.” Moore WC. Am J Respir Crit Care Med 2010;181:315–23
. The authors showed that the resulting fivepatient. cluster could be correctly characterized on the basis of. onlymerely three clinical parameters: pre- and postbronchodilator. percentage of predicted forced expiratory volume in 1 s. and age of onset of asthma. However, this cluster did not correlate. with the terms severe asthma and treatment refractory. asthma. Moore WC. Am J Respir Crit Care Med 2010;181:315–23.")
11
Wenzel S. Nature Medicine 2012;18:716

12
Atópico Precoce Eosinofílico Obstrução fixa
Carvalho Pinto, RM. Resp Med 2012; 106:47

13
Não atópico Tardio Eosinofílico Obstrução fixa
Carvalho Pinto, RM. Resp Med 2012; 106:47

14
Atópico Tardio Eosinofílico Obstrução fixa
Carvalho Pinto, RM. Resp Med 2012; 106:47

15
Não atópico Precoce Não eosinofílico Obstrução fixa
Carvalho Pinto, RM. Resp Med 2012; 106:47

16
Miscelânea Carvalho Pinto, RM. Resp Med 2012; 106:47

17
Asma neutrofílica – pior resposta a CE inalatório
VEF1 Escore de sintomas -0,1 0,1 0,2 -20 -15 -10 -5 Neu Eo -0,2 Green. Thorax 2002;57:875–879 ver 1.4 17

18
Asma neutrofílica –resposta a macrolídeos
Basal Em tratamento Pós tratamento Simpson. Am J Respir Crit Care Med 2008; 177: 148–155

19
Tiotrópio em asma não controlada com beta 2 longa + CEinal
Kerstjens. NEJM 2012

20
Fenótipo asma grave e obesidade
Mais corticoide inalatório, cursos de corticoide oral, beta 2 de curta Mais refluxo e utilização de inibidores de bomba Menor CVF e capacidade de difusão Maior IMC, menor nível de IgE Mais eczema, menos pólipos nasais Gibeon D. Chest 2013;143:406

21
Influência de perda de peso sobre controle de asma e função pulmonar
Pre Post p<0.001 p=0.974 > 10% ≤ 10% > 10% ≤ 10% Submetido para publicação

22
Anderson. Lancet 2008; 372:1107

23
Project Objectives The airways diseases asthma and chronic obstructive pulmonary disease affect over 400 million people world-wide and cause considerable morbidity and mortality. Airways disease costs the European Union in excess of 56 billion per annum. Current therapies are inadequate and we do not have sufficient tools to predict disease progression or response to current or future therapies. Our consortium, Airway Disease PRedicting Outcomes through Patient Specific Computational Modelling (AirPROM), brings together the existing clinical consortia (EvA FP7, U-BIOPRED IMI and BTS Severe Asthma), and expertise in physiology, radiology, image analysis, bioengineering, data harmonization, data security and ethics, computational modelling and systems biology. We shall develop an integrated multi-scale model building upon existing models. This airway model will be comprised of an integrated micro-scale and macro-scale airway model informed and validated by omic data and ex vivo models at the genome-transcriptome-cell-tissue scale and by CT and functional MRI imaging coupled to detailed physiology at the tissue-organ scale utilising Europe's largest airway disease cohort. Validation will be undertaken cross-sectionally, following interventions and after longitudinal follow-up to incorporate both spatial and temporal dimensions. AirPROM has a comprehensive data management platform and a well-developed ethico-legal framework. Critically, AirPROM has an extensive exploitation plan, involving at its inception and throughout its evolution those that will develop and use the technologies emerging from this project. AirPROM therefore will bridge the critical gaps in our clinical management of airways disease, by providing validated models to predict disease progression and response to treatment and the platform to translate these patient-specific tools, so as to pave the way to improved, personalised management of airways disease.
, brings together the existing clinical consortia (EvA FP7, U-BIOPRED IMI and BTS Severe Asthma), and expertise in physiology, radiology, image. analysis, bioengineering, data harmonization, data security and ethics, computational modelling. and systems biology. We shall develop an integrated multi-scale model building upon existing. models. This airway model will be comprised of an integrated micro-scale and macro-scale airway model. informed and validated by omic data and ex vivo models at the. genome-transcriptome-cell-tissue scale and by CT and functional MRI imaging coupled to. detailed physiology at the tissue-organ scale utilising Europe s largest airway disease cohort. Validation will be undertaken cross-sectionally, following interventions and after longitudinal. follow-up to incorporate both spatial and temporal dimensions. AirPROM has a comprehensive data management platform and a well-developed ethico-legal. framework. Critically, AirPROM has an extensive exploitation plan, involving at its inception and. throughout its evolution those that will develop and use the technologies emerging from this. project. AirPROM therefore will bridge the critical gaps in our clinical management of airways. disease, by providing validated models to predict disease progression and response to. treatment and the platform to translate these patient-specific tools, so as to pave the way to. improved, personalised management of airways disease.")
24
Segurança de dados e ética Modelagem computacional
AIRPROM : Airway Disease PRedicting Outcomes through Patient Specific Computational Modelling Fisiologia Radiologia Análise de imagens Bioengenharia Harmonização de dados Segurança de dados e ética Modelagem computacional Biologia de sistemas.

25
Pediatric Research. online publication 27 February 2013. doi:10
Pediatric Research. online publication 27 February doi: /pr

26
Interface Focus 2013 3, 20120057, published 21 February 2013

27
Interface Focus 2013 3, 20120057, published 21 February 2013

28
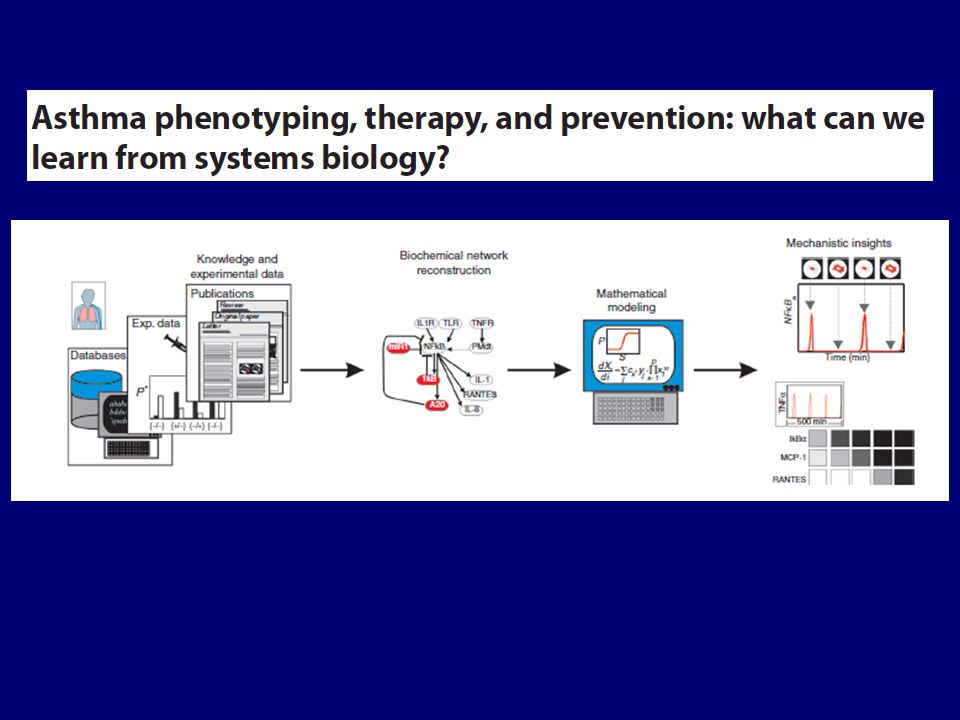
Pediatric Research. online publication 27 February 2013. doi:10
Pediatric Research. online publication 27 February doi: /pr

29
Medicina dos 4 P Personalizada Genoma pessoal Preditiva
Avaliação riscos a partir da personalização Preventiva A partir da predição pode-se prevenir Participativa O indivíduo tem de participar para resolver o que for detectado

Apresentações semelhantes
 – Lápides 1, 2, 3» «nomes gravados, 21 de Agosto de 2008» «Ultramar.TerraWeb»>")

 - Estudo ISAAC BRASIL, 1996 % Itabira.>")





 – Coordenador Ana Maria Menezes (RS) Ana Luisa Godoy Fernandes (SP) Marcus.>")










